 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4-A
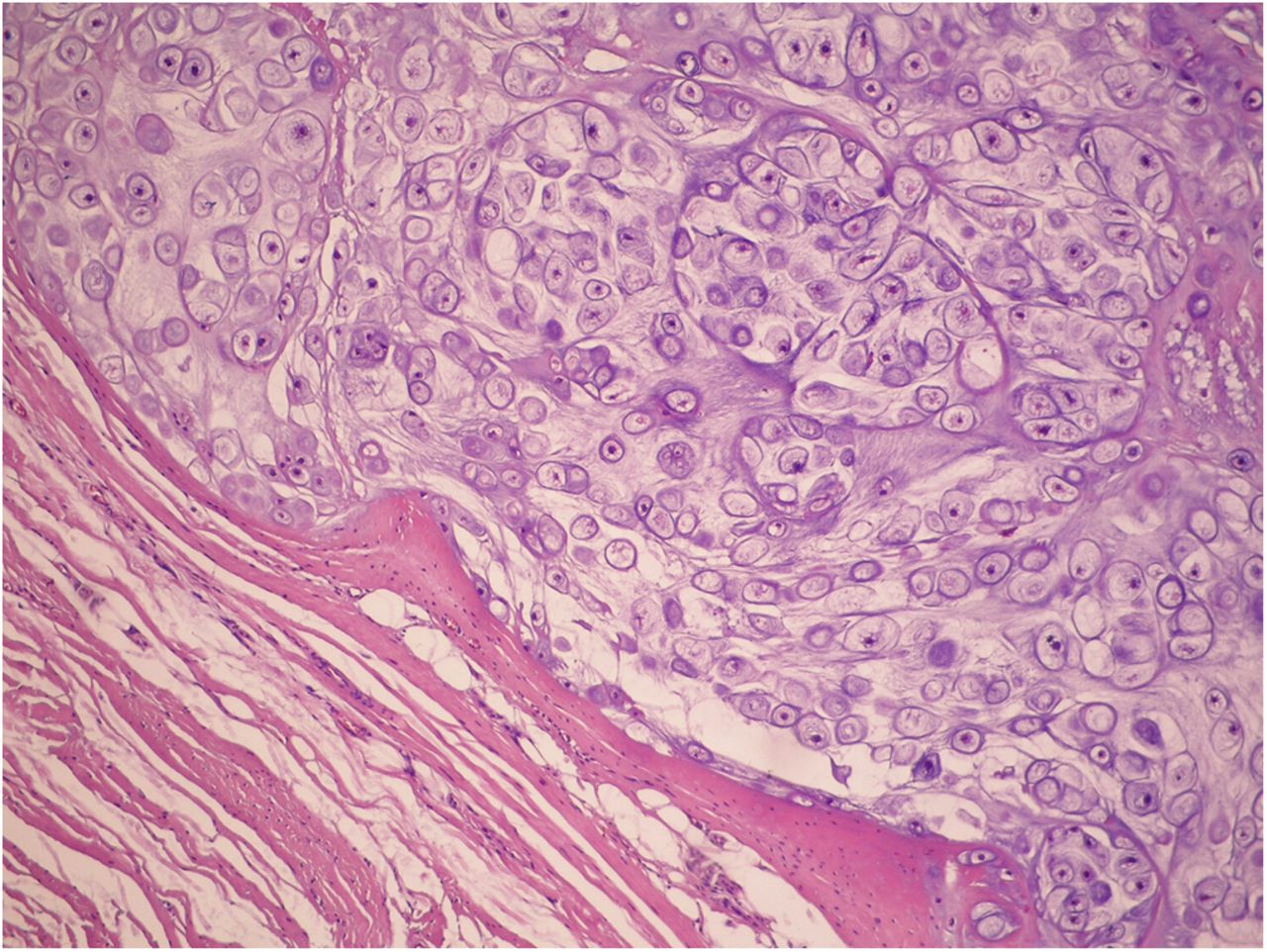
Fig. 4-A Fig. 4-B
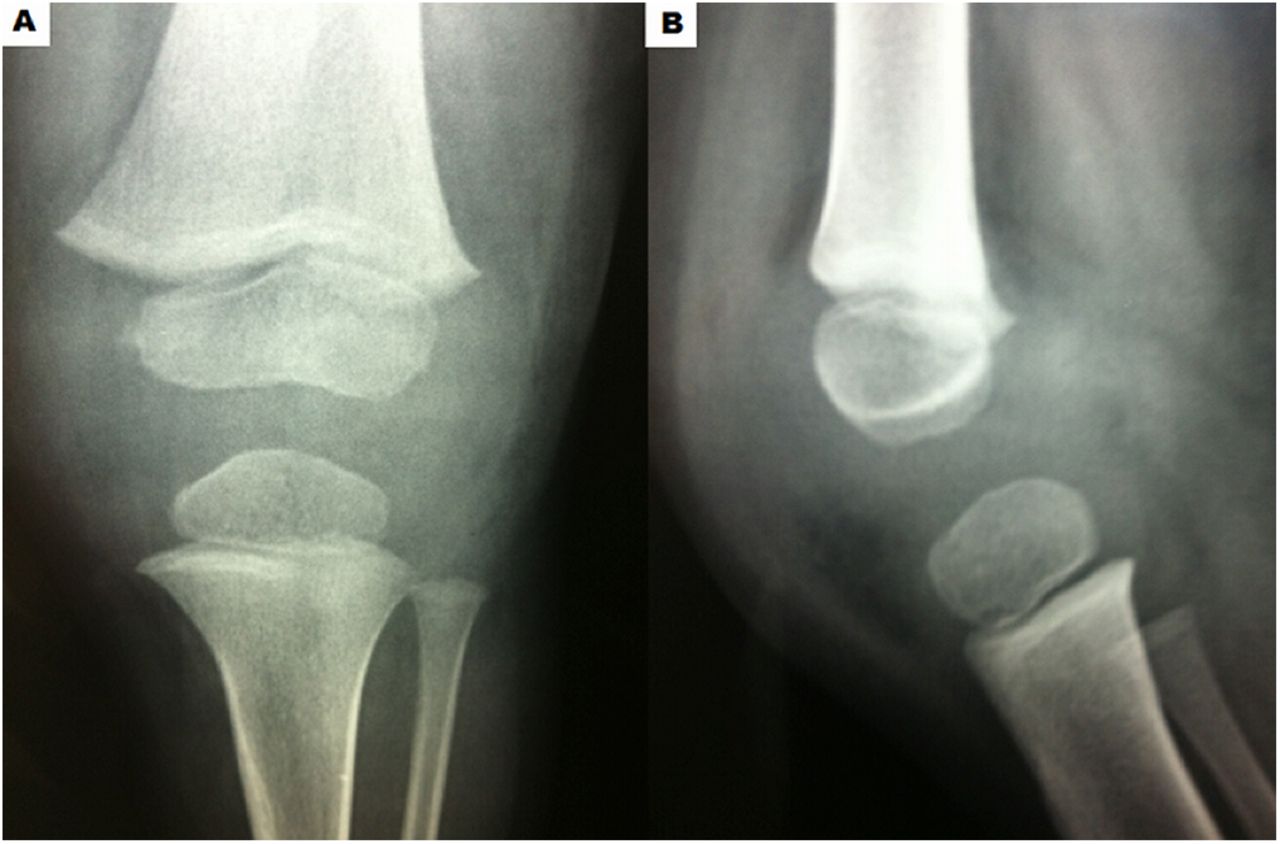
Fig. 4-BA 2-year-old boy presented to the emergency department in July 2014 with pain and lameness in the left knee, which had begun 30 days earlier and worsened in the last 7 days. He did not have clinical signs of infection. He was initially thought to have transient synovitis and received medications for his symptoms and recommendations to rest. He was discharged, and his family was instructed to bring him back in case of complications. After 2 weeks, the child returned to the hospital with worsening pain, lameness, loss of knee range of motion (20° to 100°), and joint effusion in the same knee. Radiographic examination did not show any abnormalities (Fig. 1). He was found to have an effusion, and joint aspiration yielded clear synovial fluid (9,000 white blood cells/mm3, normal glucose, 70% polymorphonuclear cells and 30% mononuclear cells, a positive [+] leukocyte esterase test result, crystals, and negative Gram staining), with negative culture results.
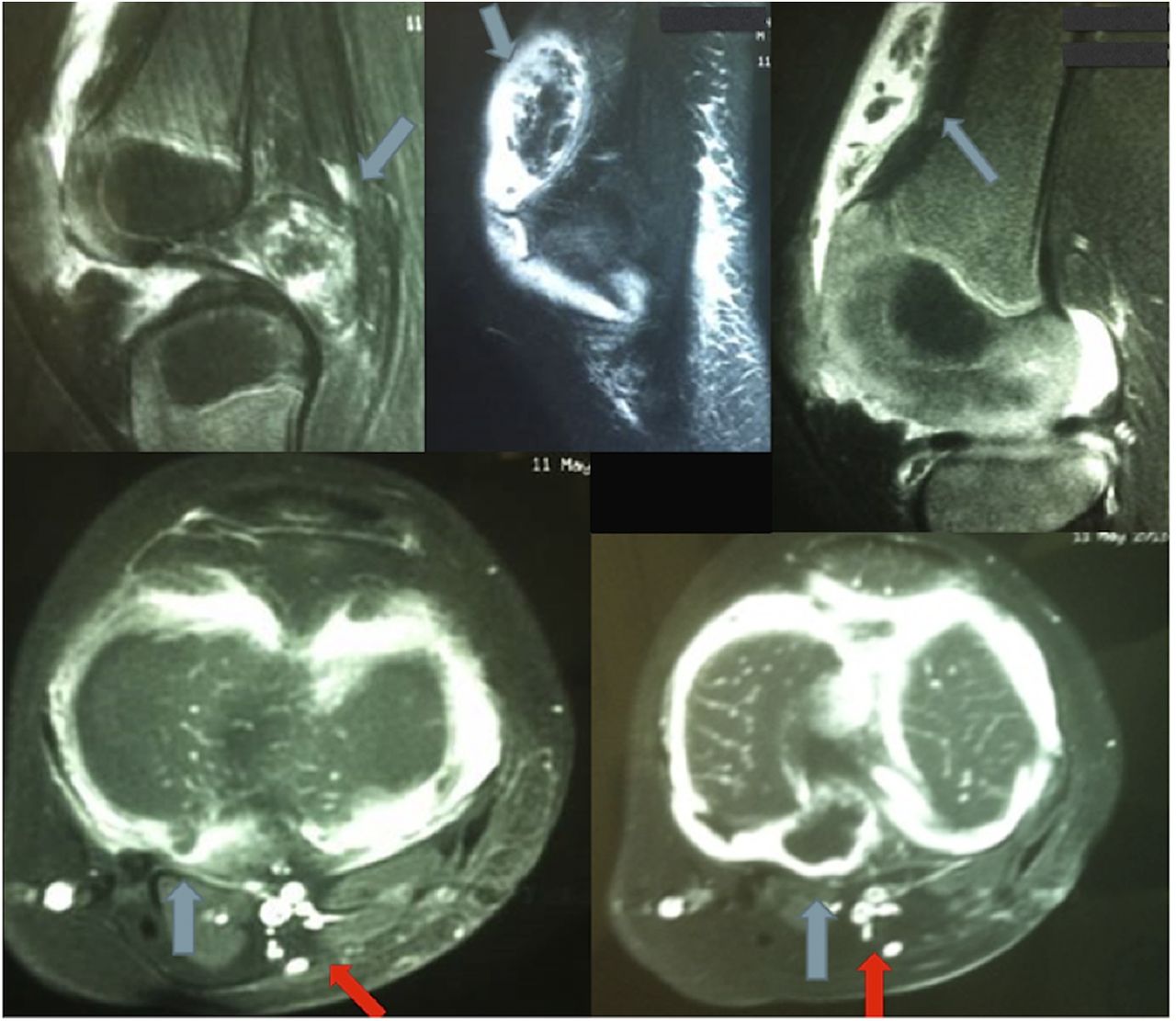
As the diagnosis was not clear, magnetic resonance imaging (MRI) of the left knee was performed. This showed several loose bodies in the anterior compartment of the knee and a large osteochondral fragment in the posterior compartment (Fig. 2).
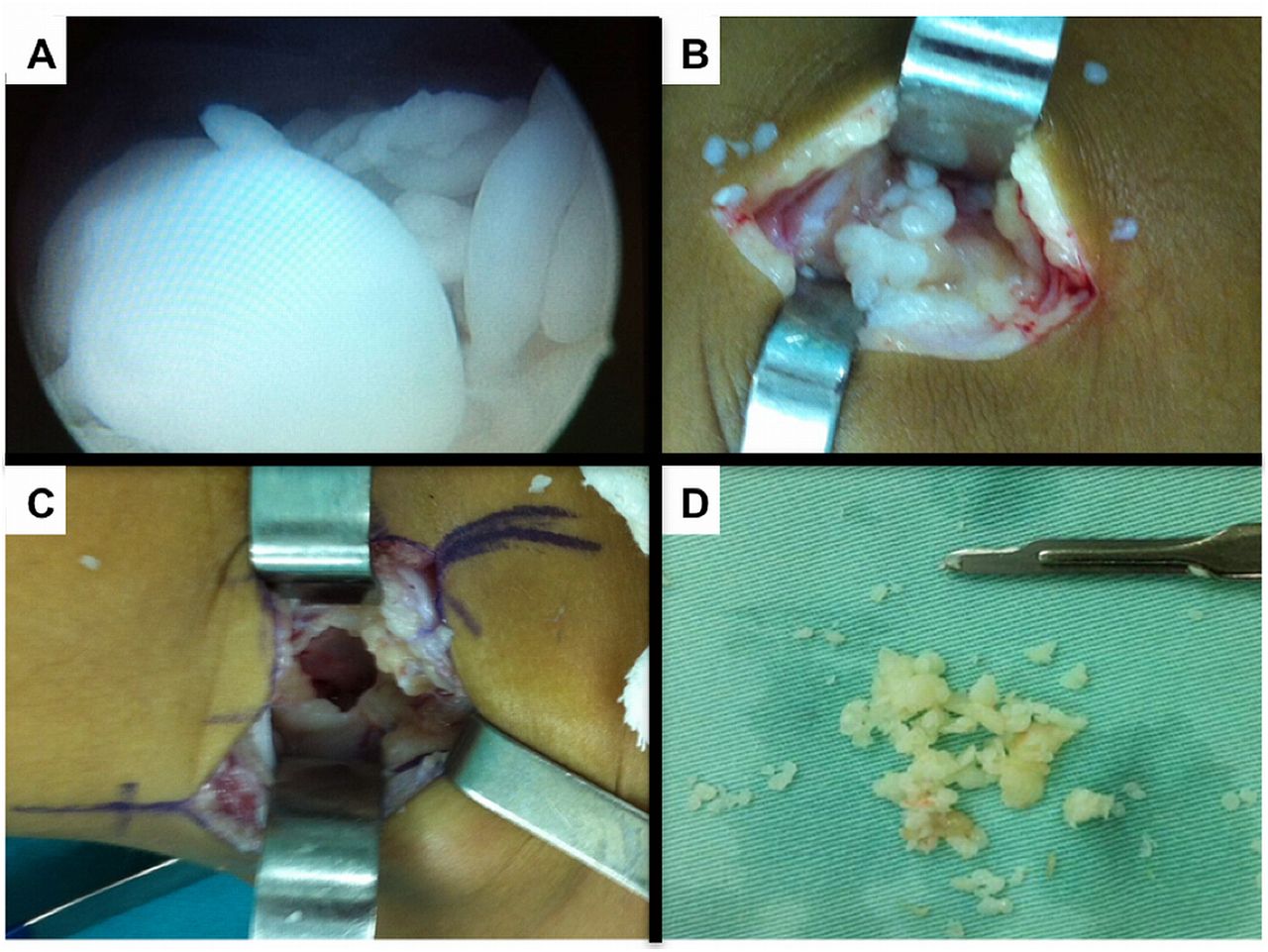
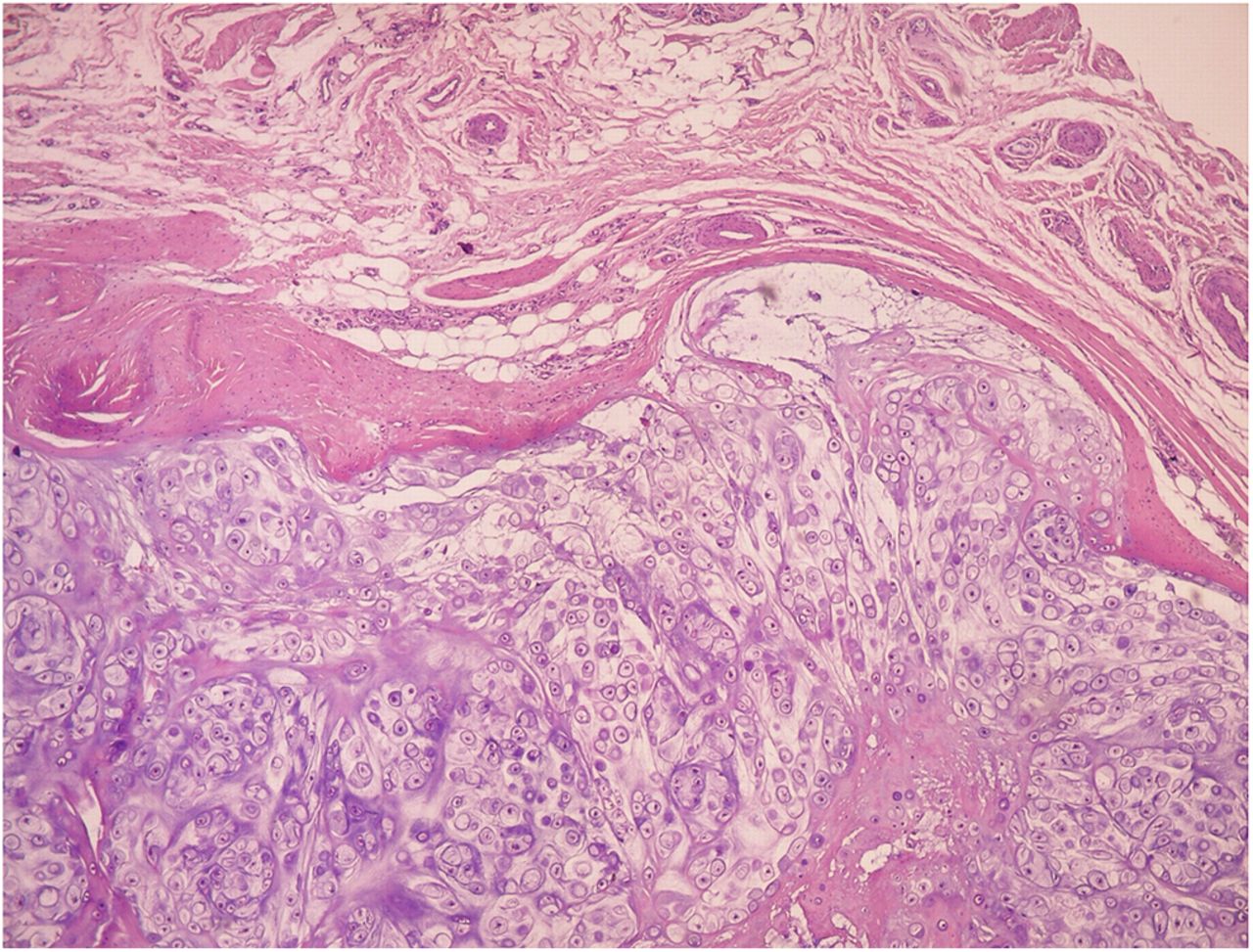
Arthroscopic surgical treatment was initially chosen for the anterior knee compartment, but it was not possible to completely remove all of the loose bodies, so open total synovectomy with anterior and posterior approaches was used (Fig. 3). The collected material was sent for histopathological examination (Figs. 4-A and 4-B).
The combination of multiple intra-articular and peri-articular nodules of cartilage and the histology showing well-differentiated hyaline cartilage yields the diagnosis of synovial chondromatosis (SC).
The patient was discharged after 48 hours, and weight-bearing and early complete range of motion were encouraged. Rehabilitation involved quadriceps strengthening exercises and exercises to restore range of motion and proprioception. At 18 months postoperatively, the patient was asymptomatic, with no joint swelling or pain, no evidence of any ligamentous instability or meniscal abnormality, and a functional range of motion (0° to 132°) without any impairment of activities.
Proceed to Discussion >>Reference: Temponi EF, Mortati RB, Mortati GMH, Mortati LB, Sonnery-Cottet B, de Carvalho Júnior LH. Synovial chondromatosis of the knee in a 2-year-old child: a case report and review of the literature. JBJS Case Connect. 2016 Aug 24;6(3):e71.
As far as we can determine, this case report presents the youngest child with SC of the knee reported in the English-language literature. Within the knee, SC predominantly occurs in the anterior compartment, such as the suprapatellar pouch, infrapatellar fat pad, and anterior interval. The posterior compartment is an uncommon location for SC. Despite being a benign disease, diagnosis and early treatment are important. Monitoring of patients should be performed routinely for the diagnosis and early treatment of possible recurrences, preventing future osteoarthritis of the knee joint.
SC usually occurs in a single joint, most commonly the knee (70%), hip (20%), or elbow (7.9%), although at least 33 different locations have been described. SC occurs most commonly in young adults (1 per 100,000 individuals in the general adult population and even more rarely in children) and is more common in males (1.8:1). It is rare in adolescents and even rarer in children. SC can be classified into primary and secondary forms as the latter can arise after pathological conditions such as trauma, infections (e.g., tuberculosis), osteoarthritis, degenerative osteopathy, cysts, osteochondritis dissecans, and neuropathic osteoarthropathy. The primary form has a high rate of recurrence, and the secondary form responds well to surgical excision and is not likely to recur after surgical removal.
Although radiographs can be useful to demonstrate loose or calcified bodies, SC may not be detected in up to 30% of cases if the nodules lack calcification. CT (computed tomography) has become an important tool because of its higher sensitivity compared with radiography for the detection of ongoing calcification around lobules of cartilage within nodules or loose bodies. Several authors have described the role of MRI in diagnosing SC. It usually reveals low to intermediate signal intensity in T1-weighted images and high signal intensity in T2-weighted images, with hypointense calcifications in both types of images. The characterization of the nodules may differ depending on the stage of formation. Younger lesions appear homogeneous with lobulated borders, and they appear as an area of isointense to slightly hyperintense signal on T1-weighted images.
Surgical treatment includes removal of loose bodies and open or arthroscopic synovectomy. Although controversies exist surrounding the effectiveness of synovectomy for preventing recurrence of primary SC, a synovectomy is generally recommended. Radiation therapy and chemotherapy usually have no role in the treatment of SC, and surgical excision remains the preferred treatment modality. However, a case reported by Chong et al. did demonstrate that radiation therapy was effective for refractory SC of the knee. Jeffreys reviewed 17 cases and concluded that removal of the loose bodies alone was preferable to synovectomy and that complete synovectomy was not indicated because of risk of stiffness of the knee joint. However, Ogilvie-Harris and Saleh compared the outcomes between a group of patients treated with removal of loose bodies alone and a similar group treated with arthroscopic synovectomy for SC of the knee, and they demonstrated that the group treated with arthroscopic synovectomy had significantly lower recurrence rates (p = 0.02). Recurrence was subsequently successfully treated with open synovectomy. Samson et al. reported on a limited cohort with good functional results after arthroscopic treatment, and Murphy et al. described 32 patients treated with open removal of loose bodies and affected synovium, only 1 of whom had a recurrence. In cases of generalized extensive SC of the knee, an open procedure appears to yield a better chance for disease eradication compared with an arthroscopic one.
Even though it is a benign disease, SC can be very destructive. It may lead to cartilage degeneration from mechanical wear caused by intra-articular loose bodies, and it may be associated with subsequent osteoarthritis. Malignant transformation to chondrosarcoma is a rare complication, with a relative risk of 5%, and is closely linked to recurrence. Malignant transformation should be suspected in chronic cases with sudden worsening of symptoms.
Reference: Temponi EF, Mortati RB, Mortati GMH, Mortati LB, Sonnery-Cottet B, de Carvalho Júnior LH. Synovial chondromatosis of the knee in a 2-year-old child: a case report and review of the literature. JBJS Case Connect. 2016 Aug 24;6(3):e71.
What is the diagnosis?
Osteochondritis dissecans
Osteochondromatosis
Chondrosarcoma
Synovial chondromatosis
Periosteal chondroma