

 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4-A
Fig. 4-A Fig. 4-B
Fig. 4-B Fig. 5-A
Fig. 5-A Fig. 5-B
Fig. 5-B Fig. 5-C
Fig. 5-CA thirty-three-year-old male runner presented with insidious onset of diffuse pain about the left knee. The discomfort had increased initially with stair climbing and activities that emphasized forceful knee extension against resistance. He had localized the pain to the anterior aspect of the knee and initially had attributed the symptoms to overuse. Three months of self-imposed activity modification and nonsteroidal anti-inflammatory medications had failed to manage the symptoms. He then sought the attention of his primary care physician. At that time, he was having discomfort with routine walking. Radiographs were obtained and interpreted as normal. He was diagnosed with an overuse syndrome and continued activity modification and use of nonsteroidal medications; ice was recommended for acute symptom exacerbation.
The following month, the patient demonstrated no improvement, and the prior radiographs were sent to a musculoskeletal radiologist for interpretation. A computed tomography (CT) scan of the knee was ordered and the patient was referred to an orthopaedic surgeon. The consulting surgeon evaluated the patient and the previous studies and ordered a magnetic resonance imaging (MRI) scan.
The patient presented to our clinic with increasing left knee pain and the inability to bear weight when the knee was flexed. He required ibuprofen for acute pain exacerbation and crutches for walking. He had no relevant medical, family, or social history.
On physical examination, the patient appeared to be a healthy young man who was alert and interactive. The left lower extremity had normal sensory and vascular function. The left thigh had obvious atrophy compared with the right. Midthigh circumference measurements showed the right to be 46.5 cm and the left to be 38.5 cm. Active and passive range of motion were full, with pain reported at maximum flexion for both maneuvers. The principal knee ligaments were intact. The patella was tender to palpation. The patient could perform a straight-leg raise; however, the maneuver elicited substantial pain.
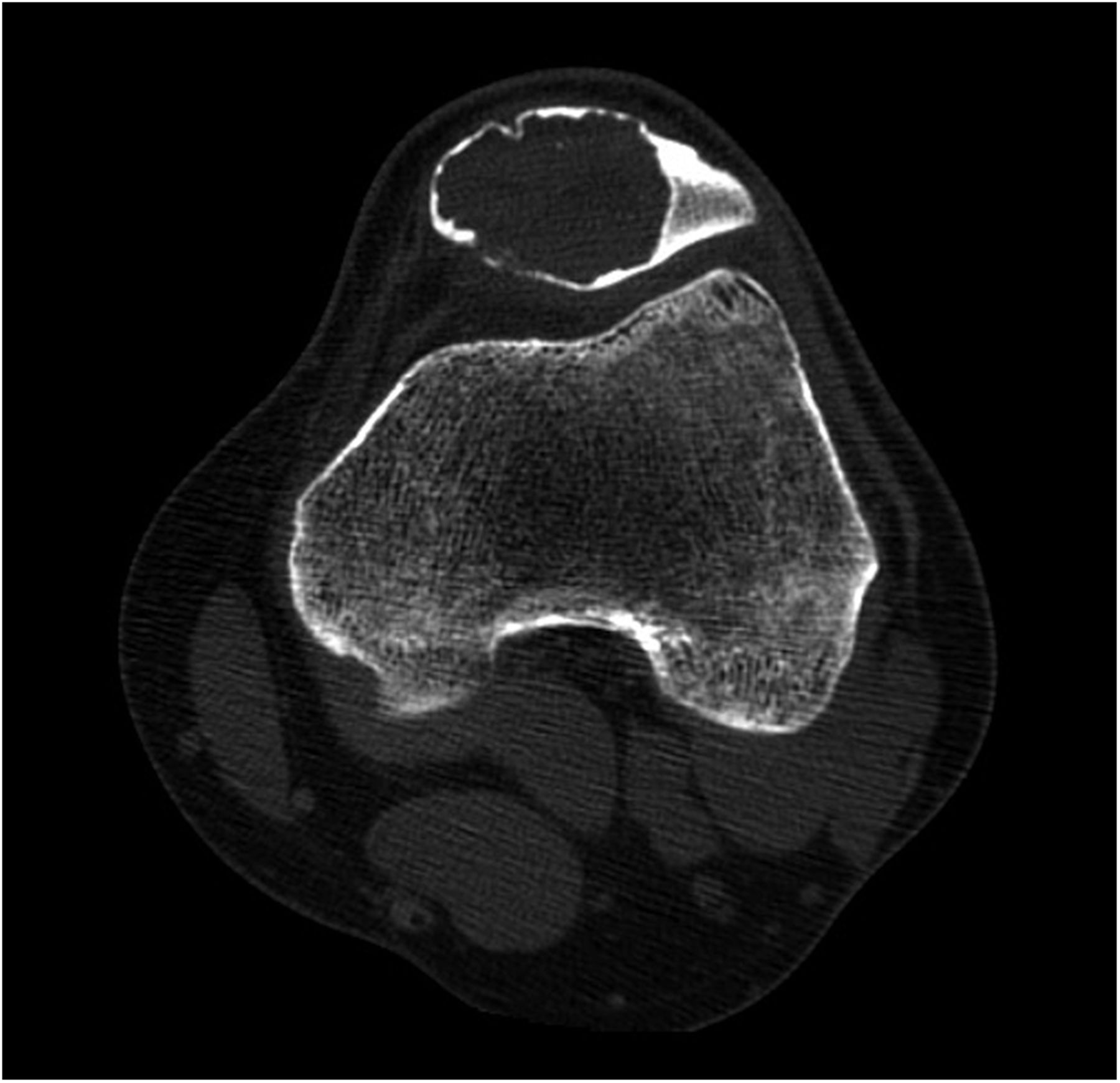
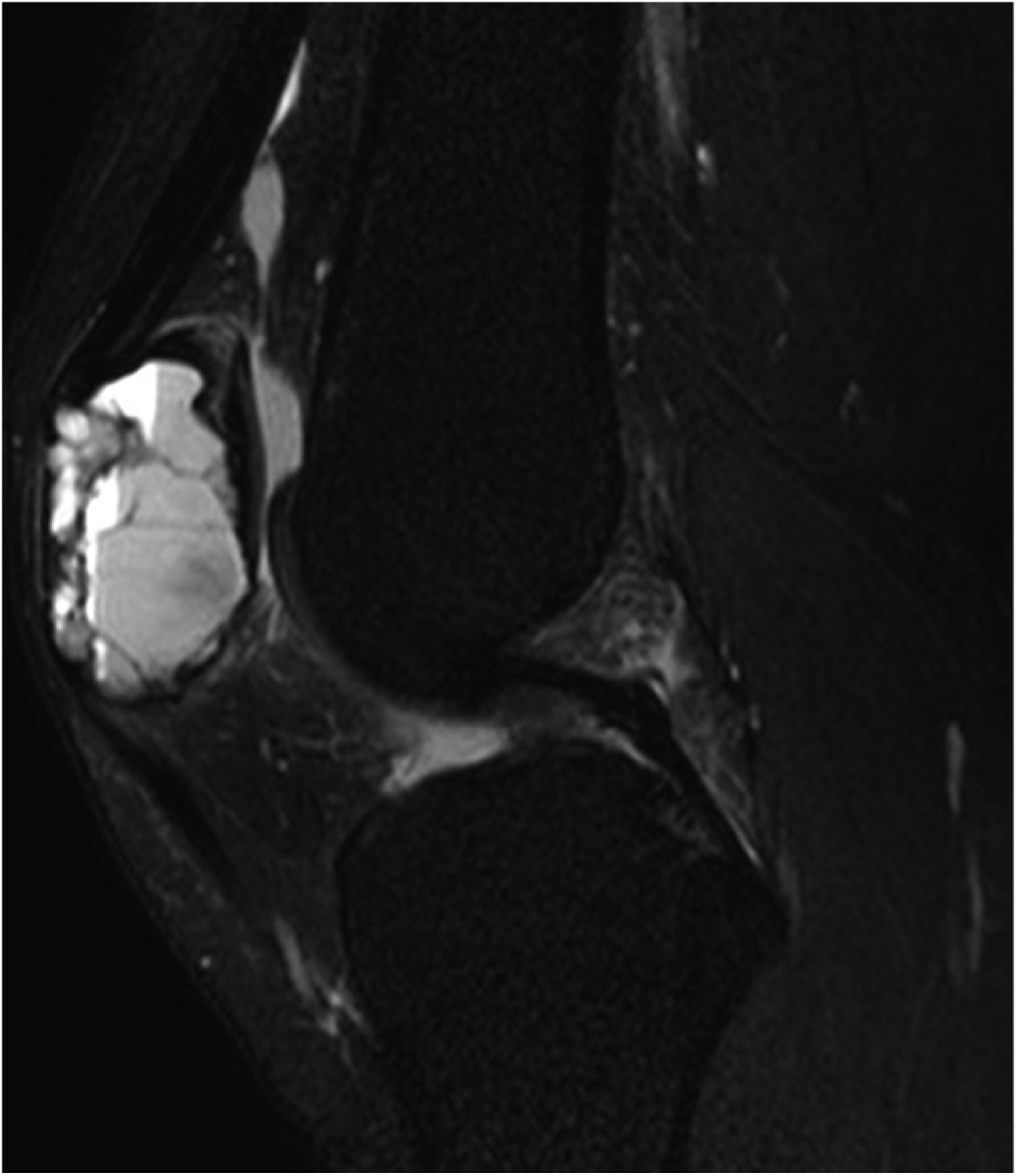
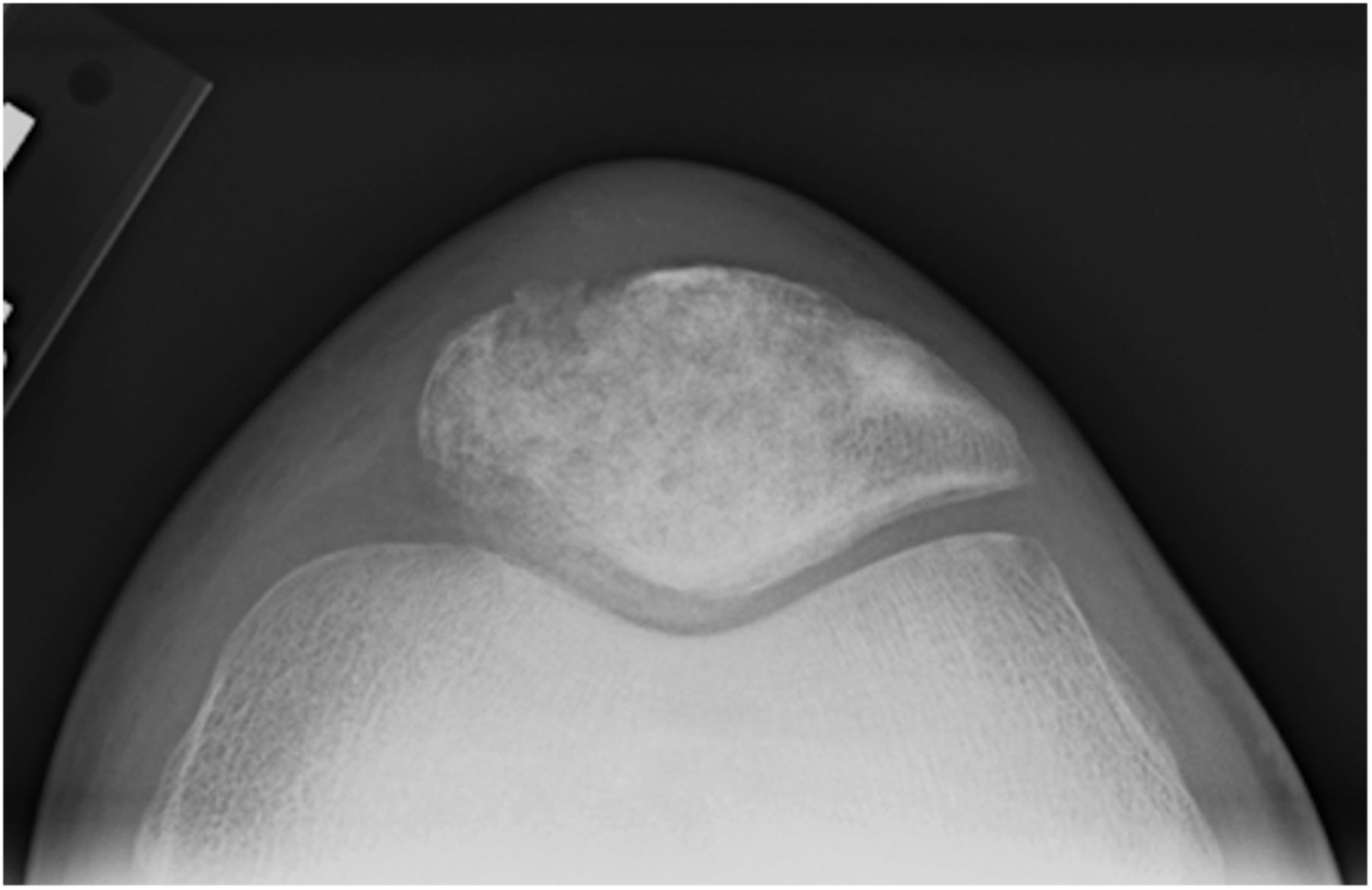
The prior radiographic studies were reviewed. Radiographs (Figs. 1-A and 1-B), CT scan (Fig. 2), and MRI (Fig. 3) were examined.
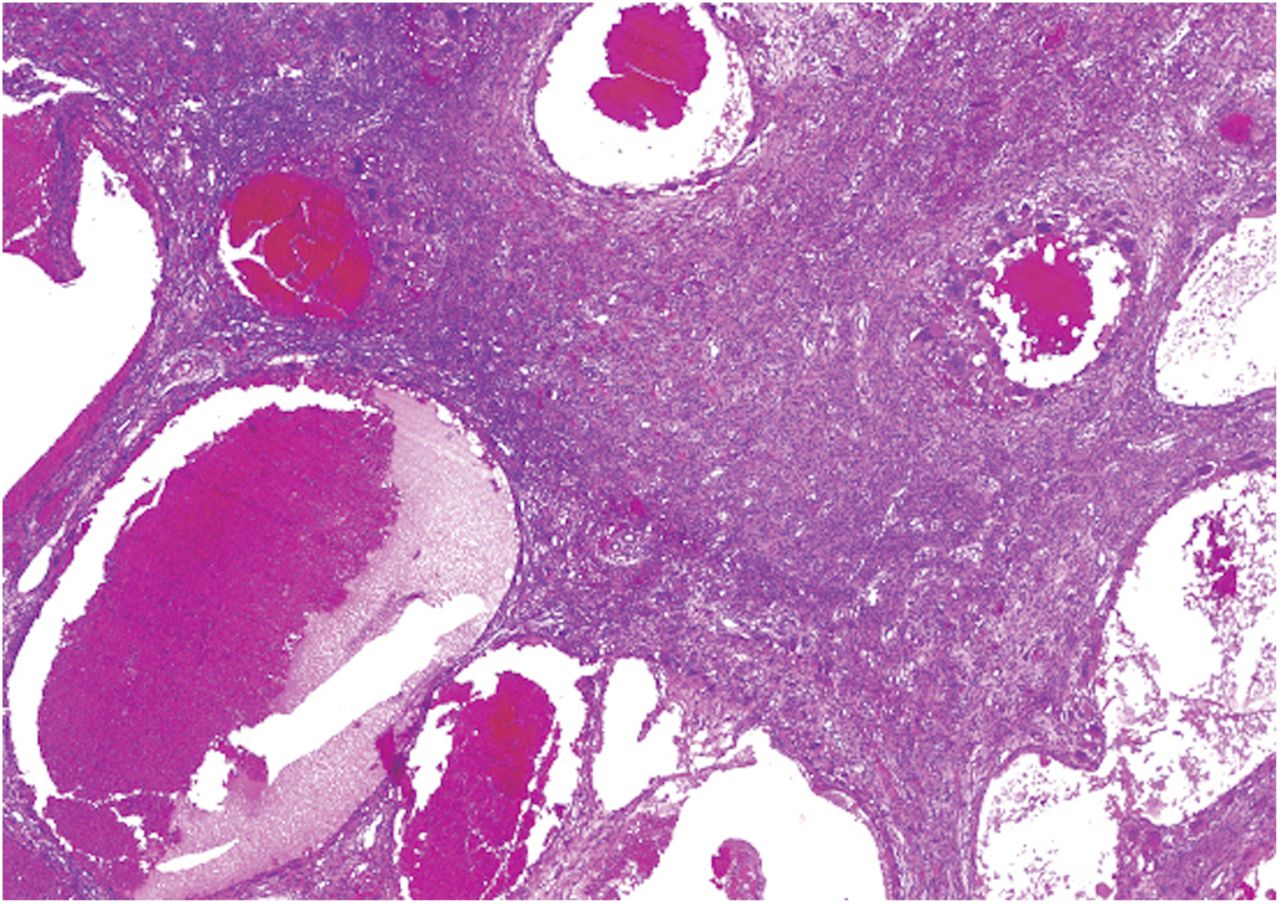
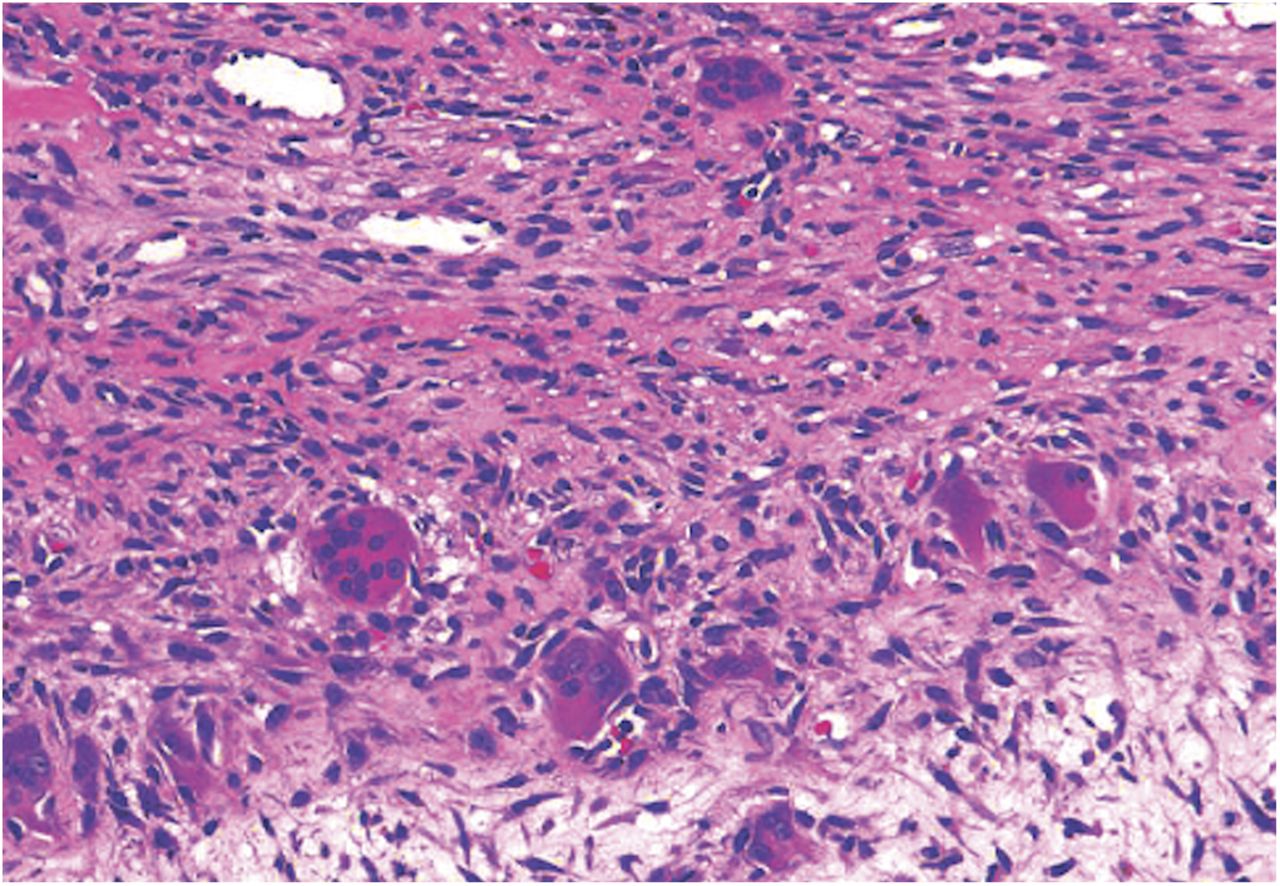
Potential diagnoses and treatment options were discussed with the patient. After informed consent and preoperative screening, the patient was brought to the operating room and a frozen section was obtained. The subsequent permanent histology is shown in Figures 4-A and 4-B.
Pertinent observations from the imaging studies include the radiolucent lesion within the medial patella (Figs. 1-A and 1-B), a homogeneous radiolucent process without central mineralization evident on the CT (Fig. 2), and evidence of a fluid-filled lesion with multiple compartments and fluid-fluid levels in the MRI (Fig. 3). The biopsy shows a fibrous connective tissue stroma with interspersed blood-filled cysts (Fig. 4-A), and numerous osteoclast-type giant cells (Fig. 4-B). This combination of findings indicates an aneurysmal bone cyst. No other underlying lesion was identified.
After the frozen section was interpreted, the cyst was curetted, with consideration given to maintaining patellar articular surface integrity, and then filled with allograft bone chips with careful use of a tamp and mallet. Given the thinness of the subchondral bone, no bone graft adjuvant was used because of the risk of articular penetration and cartilage damage. The patient was discharged home with a knee immobilizer and crutches for walking.
At the two-year follow-up, the affected knee had a range of motion from 0° to 130°; the patient had no activity limitations, and radiographs demonstrated incorporation of the bone graft (Figs. 5-A, 5-B, and 5-C).
Proceed to Discussion >>Reference: Henderson ER, Stein MI, Gebhardt MC. Aneurysmal bone cyst of the patella mimicking patellofemoral syndrome: a case report. JBJS Case Connect. 2014 May 28;4(2):e39.
Mechanical pain is caused by soft-tissue or osseous derangements that result in abnormal force transfer to local mechanoreceptors and free nerve endings. Common diagnoses associated with mechanical anterior knee pain include patellofemoral arthritis, patellar or quadriceps tendinitis, pathologic plicae, Hoffa syndrome, lateral patellar compression syndrome, and meniscus injury. Articular cartilage destruction may be a primary cause of anterior knee pain or exacerbate preexisting symptoms because of malalignment that disposes to injury. Less common but potentially serious diagnoses must also be considered, including infection and inflammatory arthritides. Neoplasms and other tumorlike conditions are often not mentioned in the regular differential diagnosis of anterior knee pain. The most common patellar tumors are chondroblastomas, giant cell tumors of bone, and aneurysmal bone cysts.
Aneurysmal bone cysts are defined by the World Health Organization as tumors composed of blood-filled spaces with septae of connective tissue and reactive woven bone. These lesions have an incidence of 0.15 per million and tend to affect patients in the second decade; there is no sex predilection. Aneurysmal bone cysts generally arise in the metaphysis of long bones and the posterior spinal elements; occurrence in the patella is rare.
The differential diagnosis of anterior knee pain is broad; however, it can be narrowed through careful history taking and physical examination. Radiographic studies should be employed early and interpreted by physicians facile in musculoskeletal imaging to confirm clinical suspicion or reveal uncommon causes of a routine presentation. In our patient, the rarity of this condition juxtaposed with the nonspecific symptoms and signs of its presentation, as well as the failure to correctly interpret the radiographs, contributed to a delay in diagnosis and appropriate management. While exceedingly uncommon, bone tumors should always be included in the differential diagnosis when evaluating patients with musculoskeletal symptoms consistent with common conditions because failure to do so may lead to delayed diagnosis and management.
Reference: Henderson ER, Stein MI, Gebhardt MC. Aneurysmal bone cyst of the patella mimicking patellofemoral syndrome: a case report. JBJS Case Connect. 2014 May 28;4(2):e39.


What is the diagnosis?
Giant cell tumor of bone
Aneurysmal bone cyst
Chondroblastoma
“Geode” (osteoarthritic cyst)
Non-ossifying fibroma