


 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 6
Fig. 6A 16-year-old boy was referred for an 18-month history of pain and stiffness affecting the left wrist. The pain eventually resolved, but substantial stiffness remained in both wrist flexion and extension. On palpation, there was diffuse swelling at the volar aspect of the wrist with no discrete palpable lesion. Radiographs demonstrated a bony abnormality on the volar surface of the lunate (Fig. 1). Computed tomography (CT) indicated that the lesion touched the adjacent scaphoid and triquetrum (Fig. 2). Magnetic resonance imagining (MRI) revealed a 1 × 2 × 1.1-cm lesion of the volar carpal bones with peripheral calcifications and was initially thought to be a calcified hematoma or nonunited volar pole injury of the lunate.
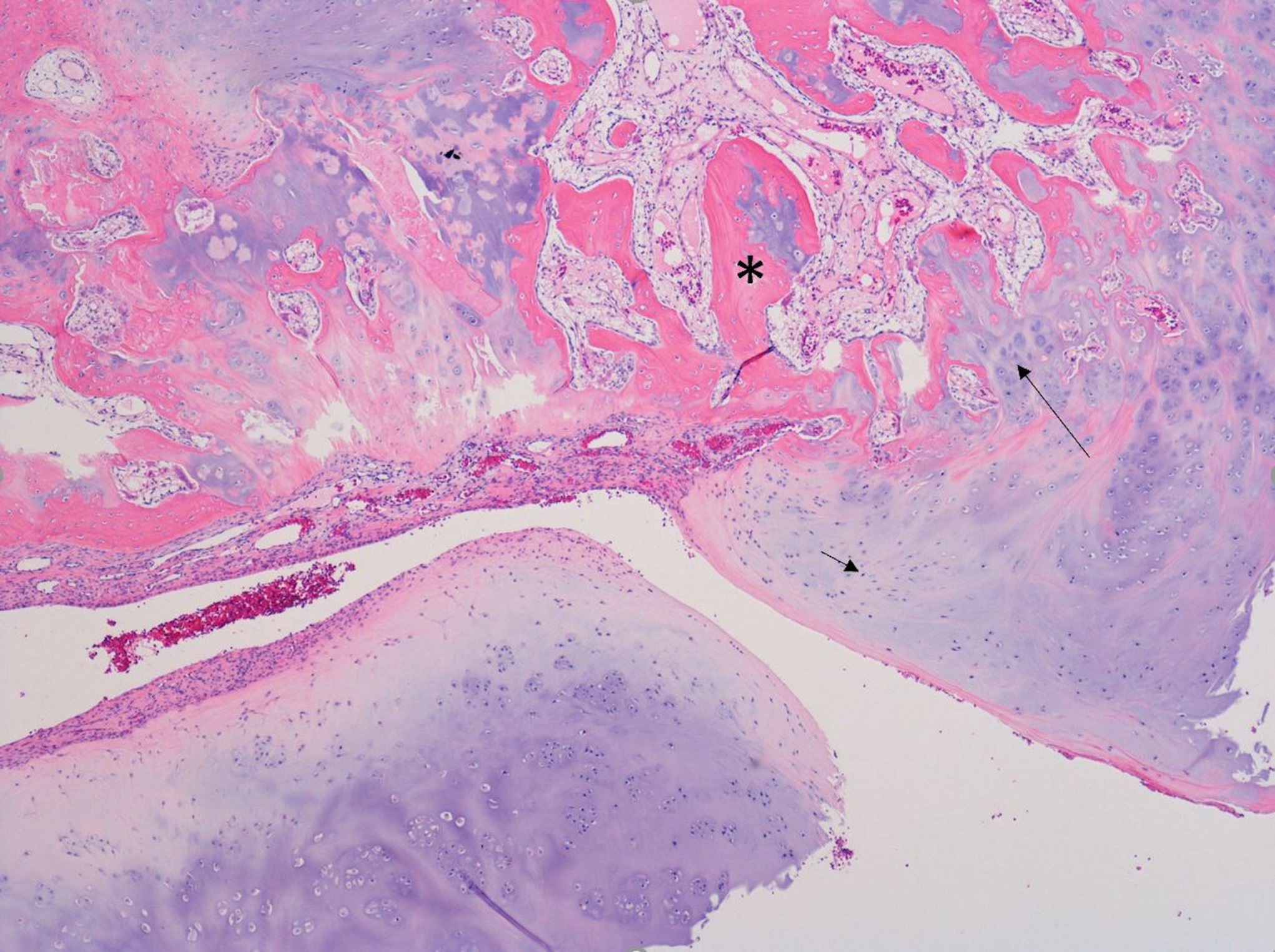
Surgical excision through a palmar approach with a Z-shaped incision was performed to treat restricted range of motion. Care was taken to protect the palmar cutaneous branch of the median nerve. The transverse carpal ligament was released in a longitudinal fashion to expose the carpal tunnel. On exposure of the carpal bones, the lesion of the lunate was visualized and excised (Fig. 3). Neighboring carpal bones did not have involvement or surface damage on visual inspection. The remaining area of the lunate bone was curetted until normal-looking bone was seen, and the wound was closed in the usual fashion. The histology of the lesion is shown in Figure 4.
The imaging studies and histology were interpreted as dysplasia epiphysealis hemimelica (Trevor disease).
The patient was seen in 3-month and 1-year follow-ups. He was neurovascularly intact with no pain on palpation of the left wrist. He had full range of motion in the wrist in flexion, ulnar deviation, and radial deviation. However, he continued to have decreased extension of 20° from neutral. On radiography (Figs. 5 and 6), no bony abnormalities were seen as a cause for the restricted extension range findings. The patient was advised to continue with physiotherapy and wrist range-of-motion exercises for further improvements.
Proceed to Discussion >>Reference: Ali MI, Padhye KP, Flood M, Schollenberg E, Logan KJ. Dysplasia epiphysealis hemimelica/Trevor disease: report of a lesion solely involving the lunate bone: a case report. JBJS Case Connect. 2019 Dec;9(4):e0511.
Dysplasia epiphysealis hemimelica (DEH) is a condition of increased cell growth at the epiphysis resulting in asymmetric skeletal deformity. It is characterized by its unilateral, hemimelic effect on a given epiphysis. DEH has been classified into 3 categories: (1) localized: isolated to a single epiphysis; (2) classic: affecting multiple epiphyses of the same limb; or (3) generalized: affecting epiphyses of an entire limb. It is more common in males with a 3:1 (male:female) ratio and on the medial aspect of an epiphysis. It is not known to be hereditary or have a risk of a malignant transformation.
Although DEH lesions are described as a cartilaginous overgrowth similar to that of osteochondromas, many differences have been described in the literature. First, it is an overgrowth lesion that occurs at the epiphysis, whereas an osteochondroma originates from the metaphysis. Second, multiple osteochondromas have been linked to the exostosin (EXT) pathways, whereas DEH has not. Third, along with several immunohistological differences, the cartilaginous cap of the osteochondromas exhibits different zones of chondrocyte maturation, whereas DEH shows growth plate proliferation with no recognizable organization.
On radiographs, the epiphyseal lesions appear to be multicentric with several ossification centers, which could sometimes cause metaphyseal widening. CT can be used for its early detection of epiphyseal ossification and cortical abnormalities. MRI is superior in its ability to separate between the cartilaginous cap of DEH, adjacent bone cartilage, and the effects of the DEH lesion on the unaffected epiphysis. Secondary structural involvement on soft tissues such as ligament and tendinous insertions can also be seen on MRI, allowing for surgical planning.
Lesions of the lower extremity are most commonly described in the literature. These sites include the distal part of the femur, the tibia or fibula, and the tarsus. Upper-extremity studies have shown involvement of the glenoid, humerus, radius, and ulna. In addition, multiple carpal bones including the scaphoid, trapezium, lunate, hamate, and capitate have been reported. However, all lesions of the lunate bone have been associated with bordering bony structures (distal part of the ulna, scaphoid, triquetrum, trapezium, trapezoid, capitate, and hamate), and a DEH lesion of only the lunate was not found in the literature.
The natural history of DEH is cessation of proliferation at the time of growth plate fusion, with links to early union. With no reported progression to malignancy in the literature, asymptomatic lesions tend to be conservatively managed. The indications for surgical treatment include pain, skeletal deformity, and decreased range of motion. Juxta-articular lesions, as described by Kuo et al., are often treated by excision. Lesions with intra-articular involvement have had conservative and surgical approaches, both reporting positive outcomes. Given the rarity of intra-articular lesions and subsequent scarcity of evidence, no clear consensus regarding treatment exists.
Although there have been previous case reports of DEH lesions involving the lunate, this report remains, to our knowledge, the only reported case of a solitary lesion to the lunate with no other bony involvement. In this case report, DEH of the left lunate was confirmed on imaging and histopathologic examination and was treated surgically because of stiffness and decreased range of motion (flexion and extension). Postoperatively, the patient had no further pain and no skeletal deformity and regained full range in flexion while terminal extension was restricted.
Reference: Ali MI, Padhye KP, Flood M, Schollenberg E, Logan KJ. Dysplasia epiphysealis hemimelica/Trevor disease: report of a lesion solely involving the lunate bone: a case report. JBJS Case Connect. 2019 Dec;9(4):e0511.


What is the diagnosis?
Periosteal chondroma
Myositis ossificans
Dysplasia epiphysealis hemimelica (Trevor disease)
Parosteal osteosarcoma
Melorheostosis