A 47-Year-Old Man with Lost Feeling in the Shoulder
October 2, 2019




 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 1-C
Fig. 1-C Fig. 1-D
Fig. 1-D Fig. 2-A
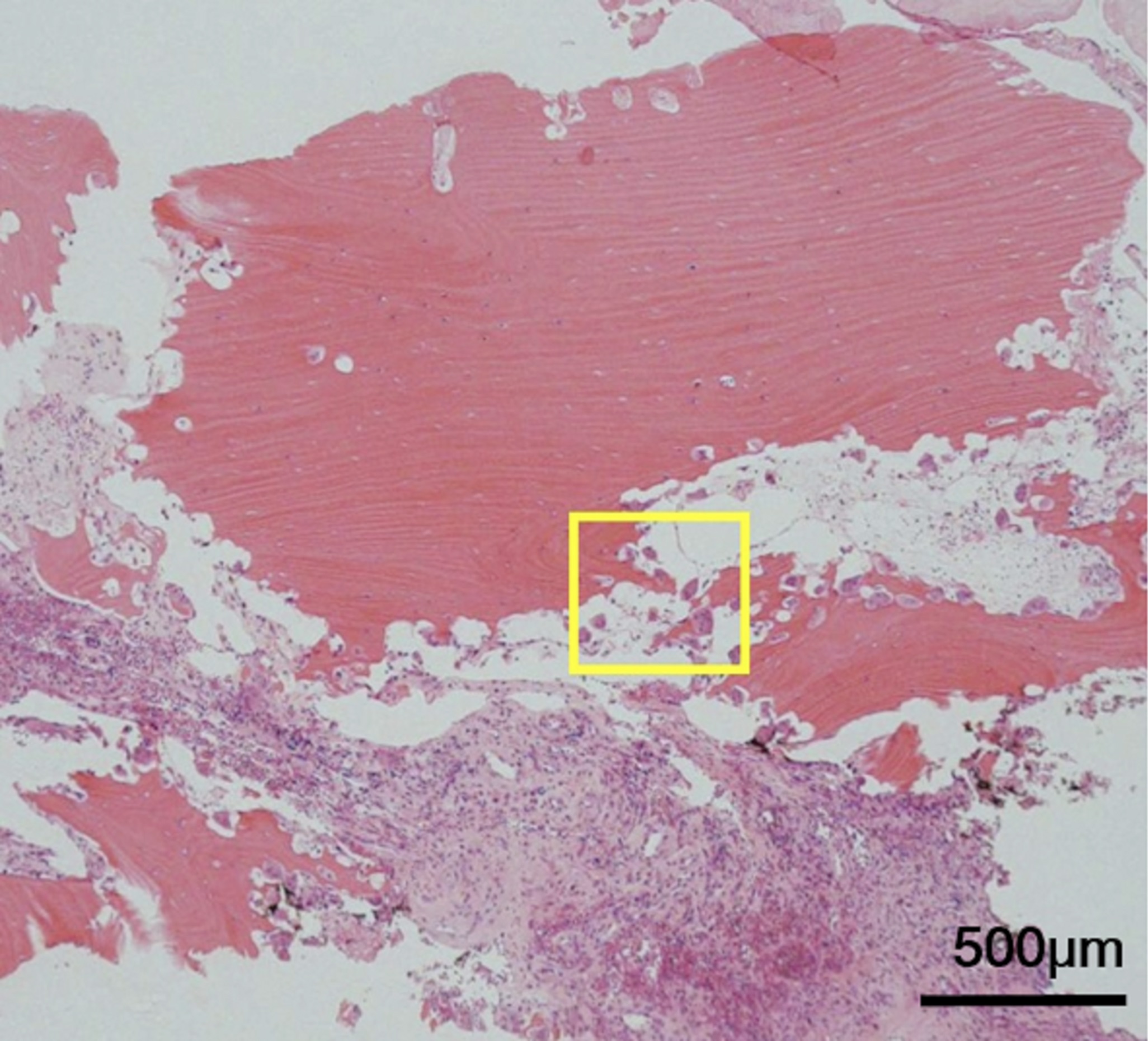
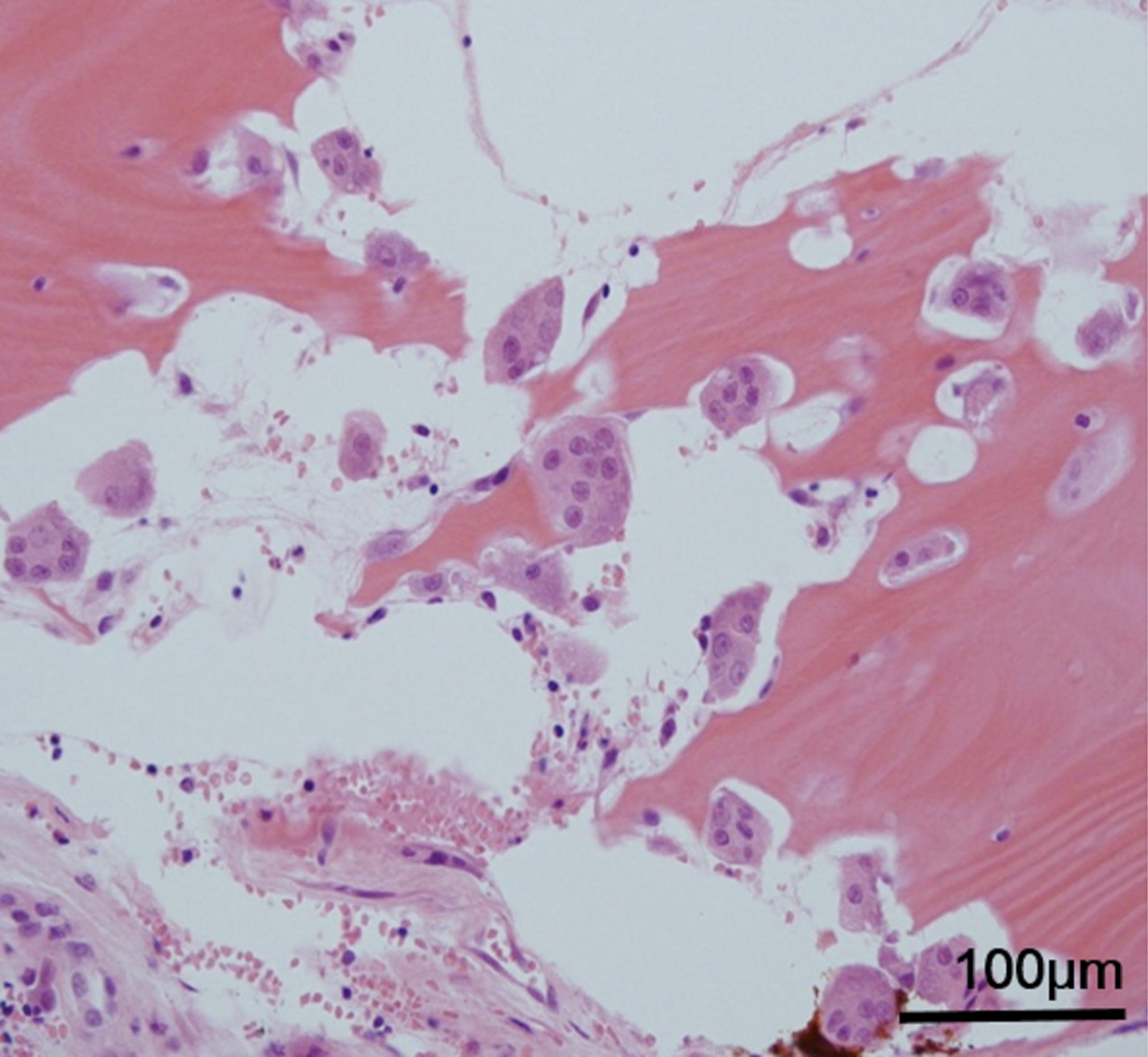
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-BA 47-year-old man was referred with progressive osteolysis of the left shoulder girdle (Figs. 1-A and 1-B). He had sustained the osteolysis for 6 years prior to his visit. He had a history of fractures of the left clavicle and scapula, induced by a fall. A physical examination showed loss of tactile sensation of the bony structure and muscle atrophy around the shoulder girdle. Radiographs and computed tomography images taken at the initial visit demonstrated osteolysis in the left shoulder (Figs. 1-C and 1-D).
The combination of clinical features, imaging findings, and histology led to the diagnosis of Gorham-Stout disease (also known as massive osteolysis or disappearing bone disease).
A blood workup showed no evidence of secondary hyperparathyroidism, renal osteodystrophy, inflammatory diseases, or myeloma. An open biopsy demonstrated proliferation of atypical vessels, with numerous osteoclasts in the resorption lacunae (Figs. 2-A and 2-B).
Pamidronate 30 mg was intravenously administered and repeated 7 times throughout the year after its first administration, ultimately suppressing the progressive osteolysis (Fig. 3-A). Thereafter, bisphosphonate therapy was shifted to the daily oral administration of alendronate 5 mg and continued for about 4 years. At the most recent follow-up at 9 years after the discontinuation of bisphosphonate therapy, no clinical or radiologic signs of disease progression or recurrence were observed (Fig. 3-B).
Proceed to Discussion >>Reference: Matsumoto T, Naito M, Hirose J, Nakada I, Morikawa T, Tanaka S. Gorham-Stout syndrome of the shoulder girdle successfully controlled by antiresorptive agents: a report of 2 cases. JBJS Case Connect. 2019 Apr-Jun;9(2):e0285.
Gorham-Stout disease causes spontaneous progressive bone destruction in association with vascular or lymphatic angiomatosis. The disease can affect any bones but has a predilection for the ribs, cranium, spine, clavicles, and pelvic girdles. Areas of bone resorption can arise in a single bone or in multiple contiguous bones. Nine cases of isolated manifestations of Gorham-Stout disease in the shoulder have been reported.
Immunohistochemical staining of biopsy specimens has revealed that the abnormal proliferation of the endothelial capillaries observed in Gorham-Stout disease is lymphatic in origin and that the osteolysis is due to an increased number of stimulated osteoclasts. The mechanism underlying the osteoclast activation induced by the proliferation of lymphatic vessels in Gorham-Stout disease remains unclear. The uncontrolled proliferation of lymphatic endothelial cells is theorized to be driven by various growth factors, including members of the vascular endothelial growth factor (VEGF) family. Devlin et al. showed that a serum sample taken early in the course of treatment had an elevated interleukin-6 level and that the serum markedly increased osteoclast-like multinucleated cells in the cultures of normal human bone marrow and their bone-resorbing activity. Hirayama et al. also showed that the serum of patients with Gorham-Stout disease displayed increased osteoclast differentiation and bone resorption of monocyte cultures from age and sex-matched controls. In the present case, the level of a marker of bone resorption, TRAP-5b, was increased before treatment, whereas histopathology revealed osteoclasts in the resorption lacunae and in front of the segmented bones, suggesting that osteoclasts played a key role in bone destruction.
Owing to the lack of consensus on the therapeutic strategies for Gorham-Stout disease, several different approaches have been described in the literature. Surgical strategies consist of resection of the affected lesions and reconstruction using bone grafts or prostheses. Radiation therapy reportedly has varying success. The use of many pharmacologic agents has been attempted for treatment, including vitamin D, interferon α-2b, calcium, calcitonin, low-molecular-weight heparin, low anticoagulant, adrenal extracts, and androgens. Although none of these agents have a solid reputation, bisphosphonates have been demonstrated to successfully arrest the bone resorption in some cases of Gorham-Stout disease. Meanwhile, our current expanded understanding of the molecular mechanisms underlying Gorham-Stout disease promises that the pathway of lymphangiogenic growth factors can be a good treatment candidate. Thalidomide, which plays a role in downregulating VEGF expression, was reportedly successful in terminating the progression of bone destruction in Gorham-Stout disease with a combination of other options including radiotherapy and bisphosphonate. Its teratogenic potential in pregnant women and neurotoxicity are the primary side effects of thalidomide. The mammalian target of rapamycin inhibitor, sirolimus, was reportedly successful in 3 Gorham-Stout disease cases: as a single treatment in one case, in combination with zoledronate in another case, and in combination with zoledronate and surgery in the other case, but 2 of the 3 cases had characteristic adverse effects of sirolimus including metrorrhagia, mucositis, and hyperlipidemia.
RANKL is a member of the tumor necrosis factor family that critically regulates osteoclast formation, activation, and survival by binding to its receptor activator of nuclear factor-κB. Because the osteoclast is the only cell capable of bone degradation, RANKL is a critical mediator of bone resorption. Denosumab is a human monoclonal antibody to RANKL, and its effectiveness in inhibiting bone resorption has been proven in the treatment of osteoporosis, bone metastasis, multiple myeloma, and rheumatoid arthritis. However, to the best of our knowledge, the use of denosumab for GSD has been reported in only one case of a 29-year-old man with mandibular involvement; however, the treatment outcome is unknown.
Reference: Matsumoto T, Naito M, Hirose J, Nakada I, Morikawa T, Tanaka S. Gorham-Stout syndrome of the shoulder girdle successfully controlled by antiresorptive agents: a report of 2 cases. JBJS Case Connect. 2019 Apr-Jun;9(2):e0285.


What is the diagnosis?
Angiosarcoma
Osteomyelitis
Lytic phase of Paget disease
Gorham-Stout disease
Giant cell tumor of bone