An Eighteen-Year-Old Man with a Sports-Related Ankle Fracture
March 16, 2016
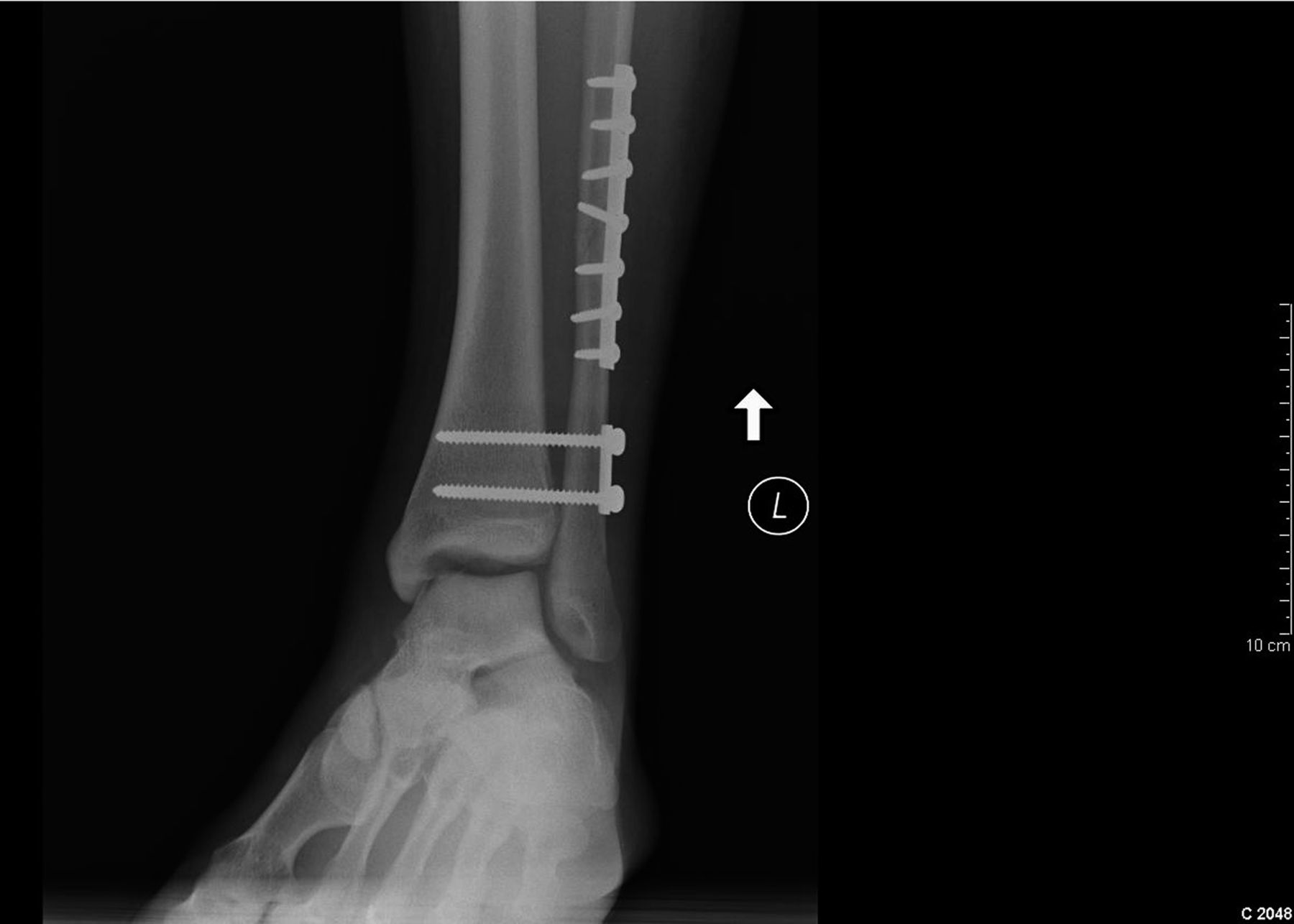

 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 3-C
Fig. 3-C Fig. 3-D
Fig. 3-D Fig. 3-E
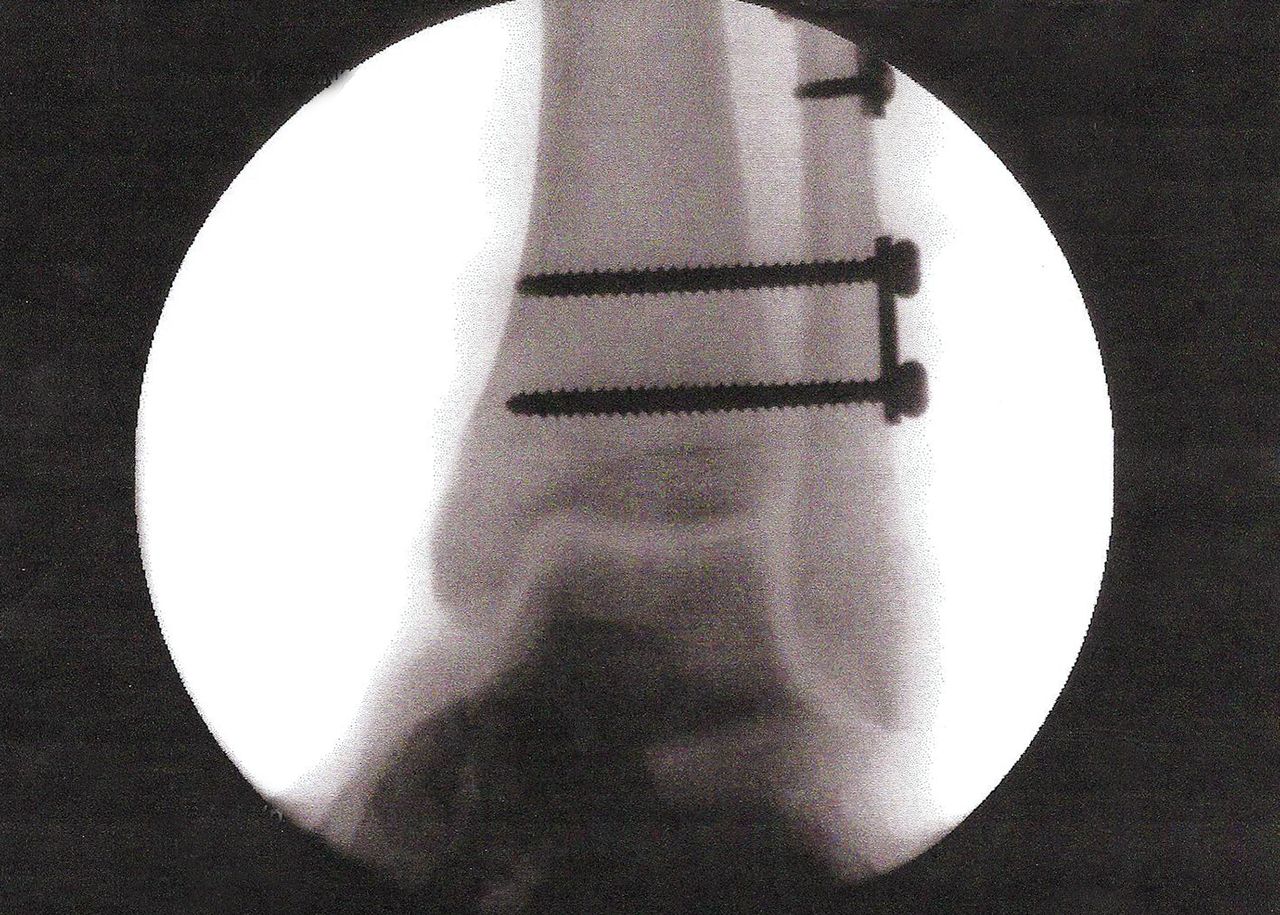
Fig. 3-EAn eighteen-year-old male patient sustained a fracture-dislocation of the left ankle while playing rugby. The injury consisted of a fracture of the fibular shaft 10 cm proximal to the ankle joint (OTA/AO fracture classification of C1), a syndesmotic disruption, and a lateral dislocation of the talus. The patient was originally seen in the emergency department of a local hospital, where the evaluating physician noted “an obvious deformity” of the ankle; a closed reduction was performed, and a splint was applied. The patient was subsequently seen by a local orthopaedic surgeon and underwent open reduction and internal fixation (ORIF) with a plate and screws placed laterally across the fracture and a separate two-hole plate with non-lag screws placed distally for fixation of the syndesmosis. This initial surgery was performed at an outside institution. During this initial surgery, the syndesmosis was clamped to reduce the tibiofibular clear space. Postoperative radiographs demonstrated what appeared to be an anatomic reduction of the fibula and syndesmosis, but with distal translation of the talus with respect to the tibial plafond and an increase in the tibiotalar clear space (Figs. 1-A and 1-B). Computed tomography (CT) scans were obtained, and the patient was referred to our office for further evaluation and treatment. At our institution, axial CT images were obtained.
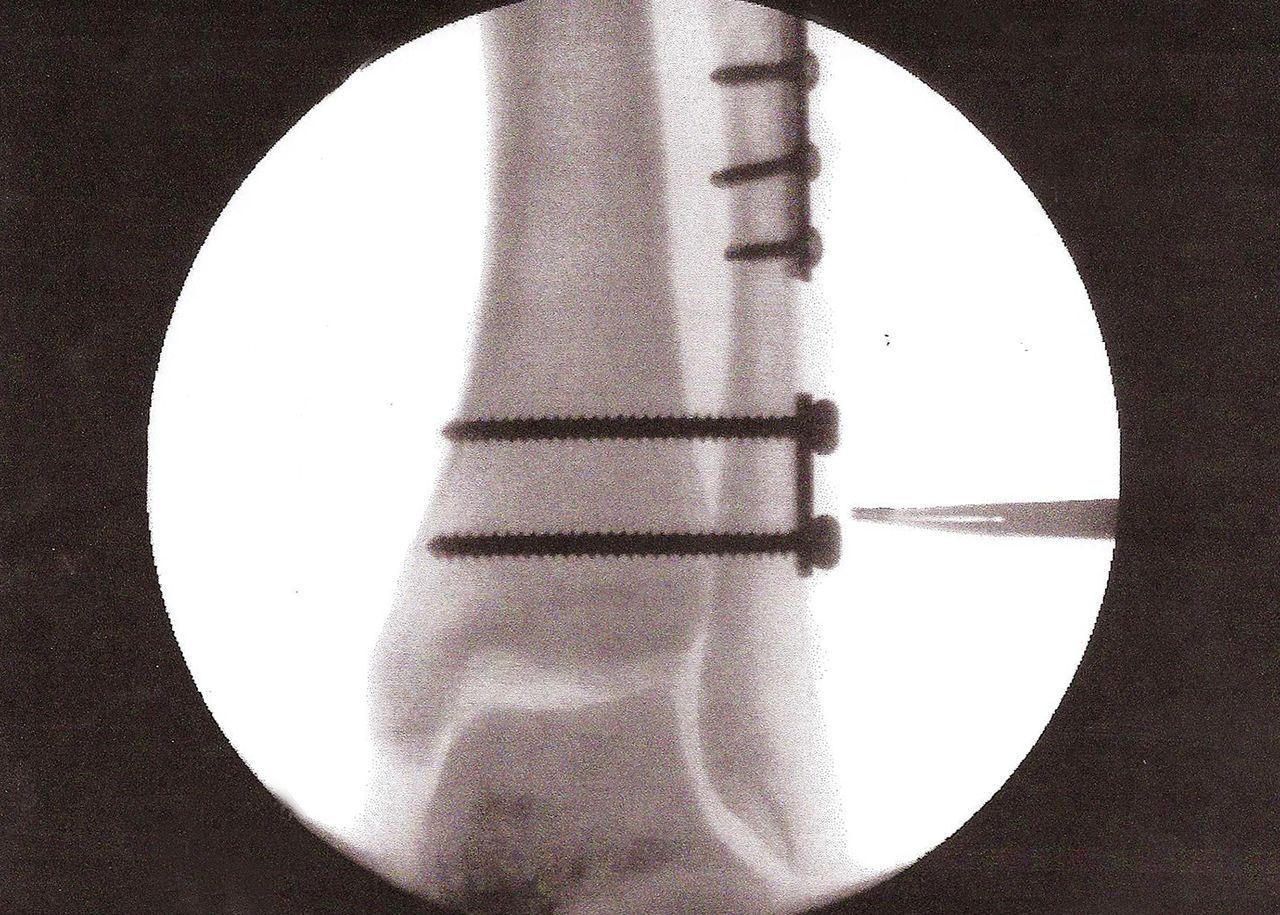
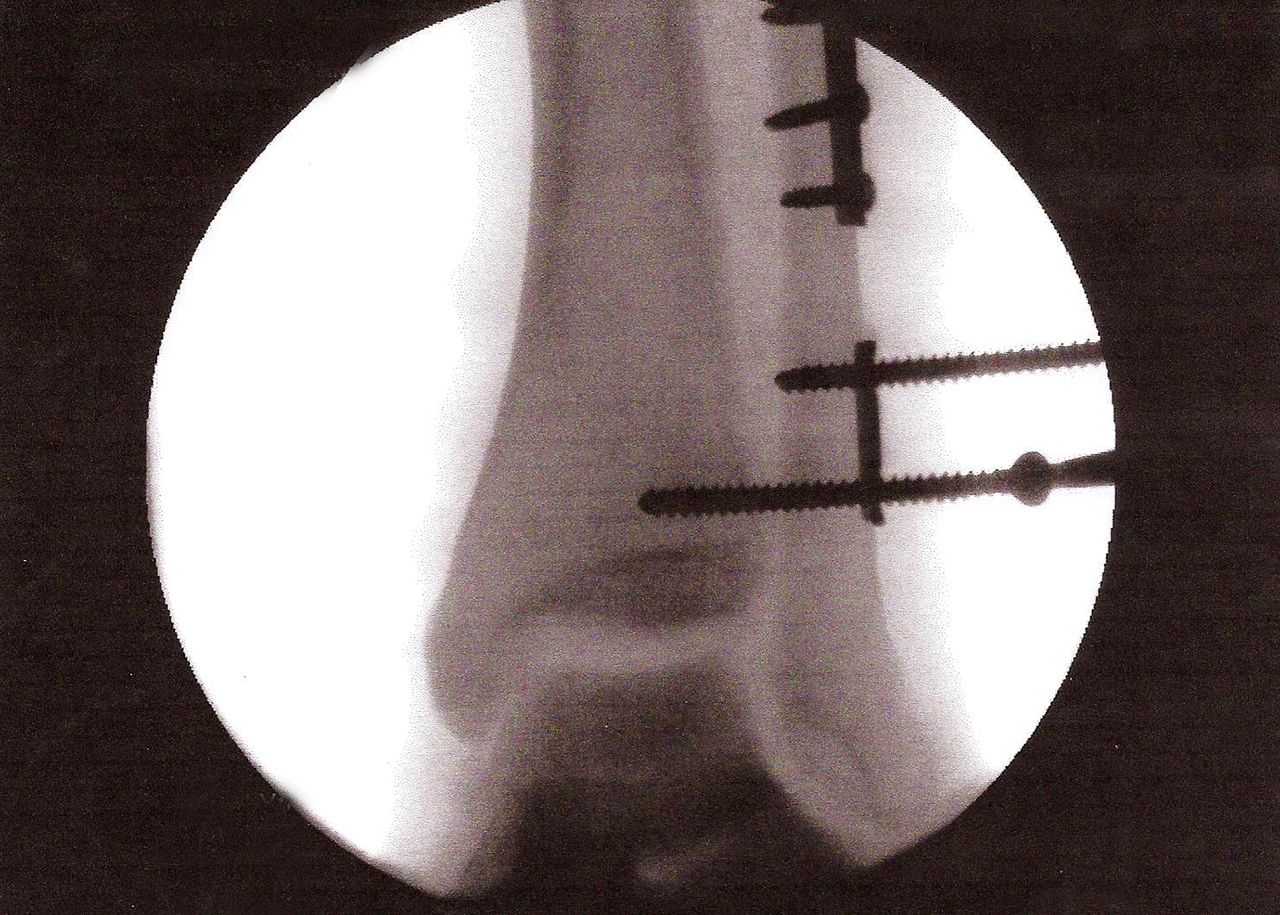
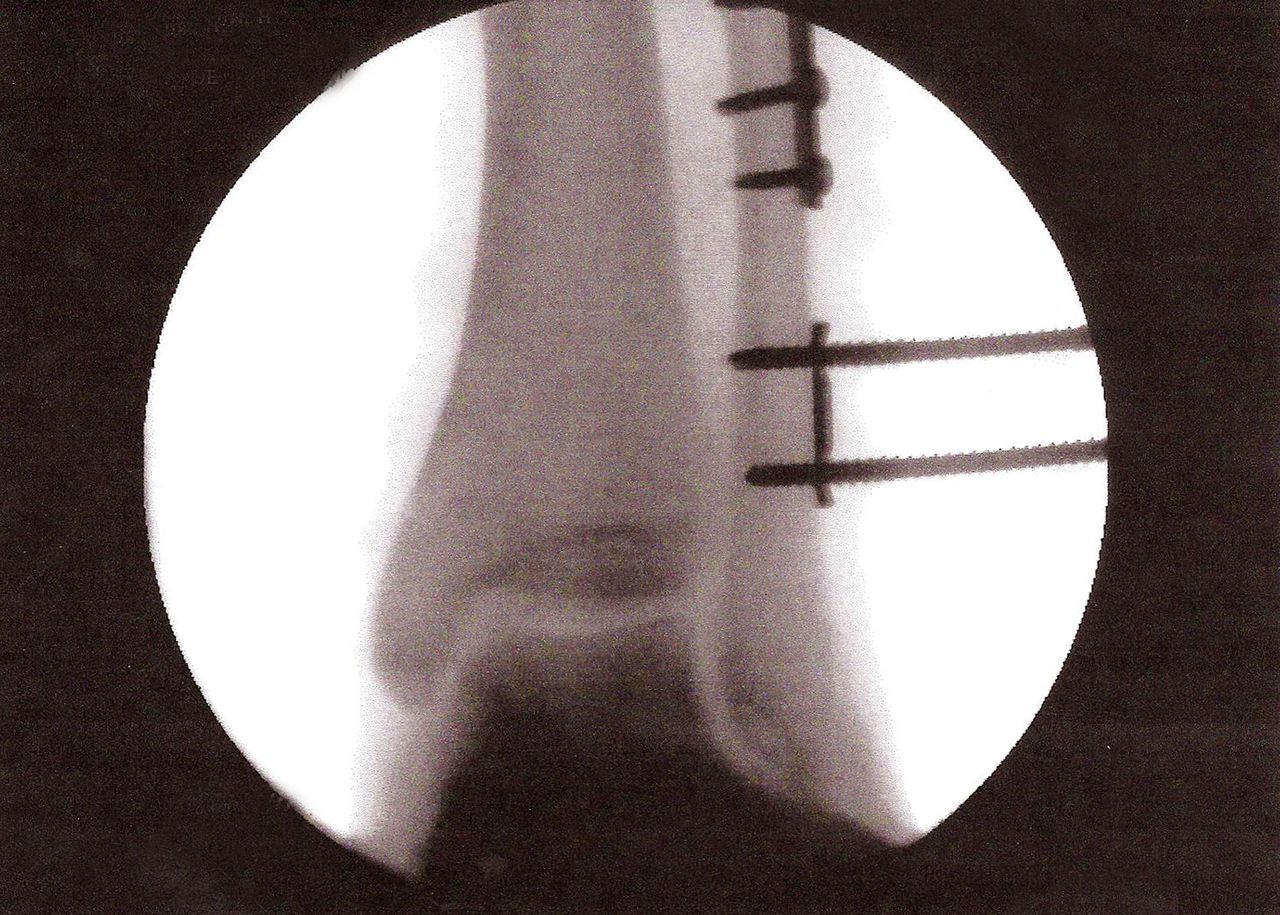
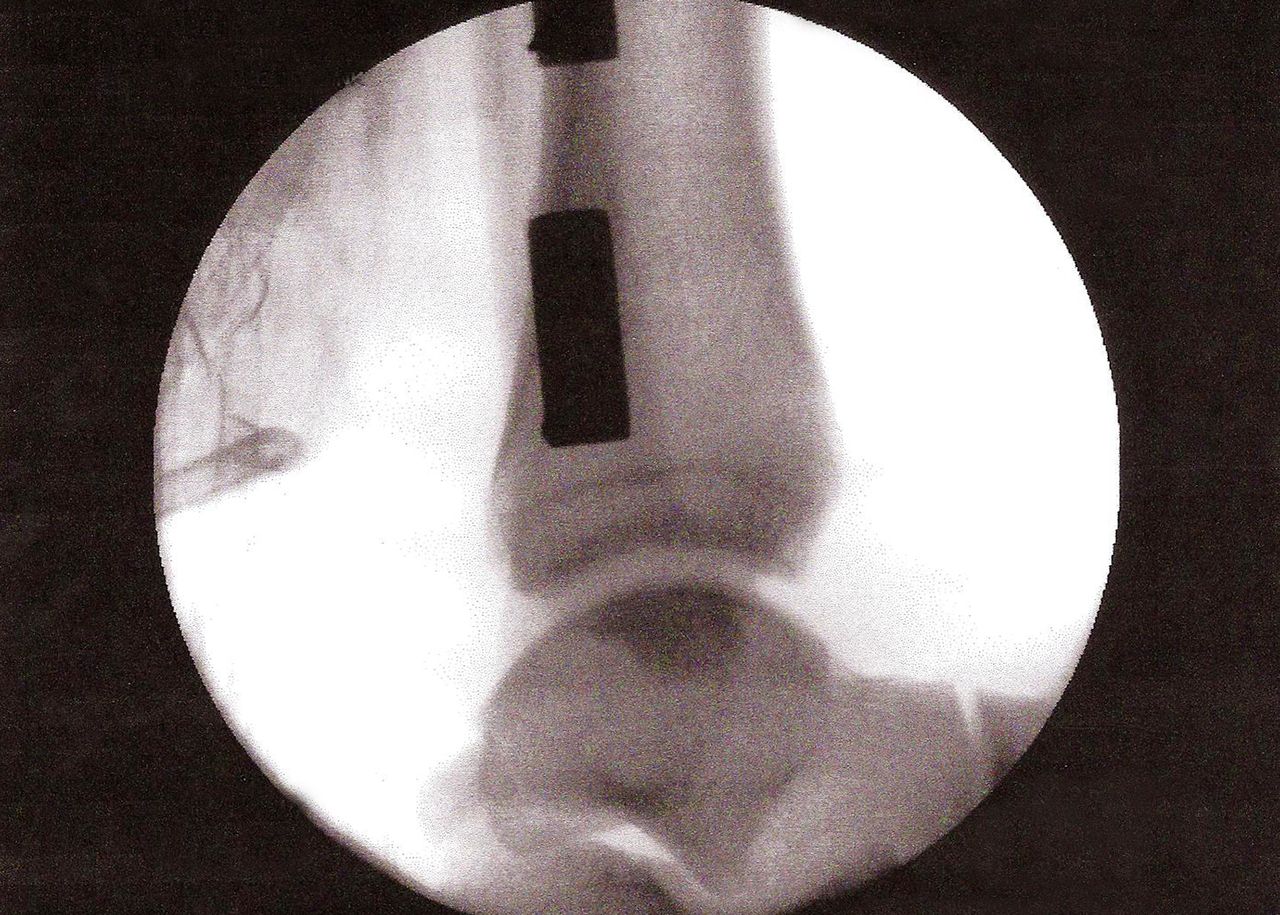
The axial CT images revealed that the distal aspect of the fibula was well reduced in the incisura without substantial anterior or posterior translation, or internal or external rotation, while coronal images confirmed distal translation of the talus with widening of the tibiotalar clear space as seen on radiographs (Figs. 2-A and 2-B). At the initial surgery, when the syndesmosis was clamped to reduce the tibiofibular clear space, it had been over-corrected. A wider clear space was normal for this patient, as a comparison radiograph showed that the clear space for the contralateral ankle was also wider than conventional standards. We determined that the patient had had an over-tightening of the syndesmosis. We performed a procedure to reposition the talus. The two syndesmotic screws were backed out of the distal aspect of the tibia while remaining engaged in the distal aspect of the fibula, allowing the syndesmosis to relax. A gentle impact to the plantar aspect of the foot with the palm of the surgeon’s hand allowed the talus to translate a few millimeters proximally, closing down the tibiotalar clear space while increasing the tibiofibular clear space and reducing the tibiofibular overlap to a degree that was symmetrical to that of the contralateral ankle. The syndesmotic screws were then advanced into the tibia through the previous screw tracks, engaging both tibial cortices (Figs. 3-A through 3-E). A short-leg splint was applied, and the patient was instructed to remain non-weight-bearing on the left side. Postoperatively, he was kept non-weight-bearing for two weeks in the splint and for an additional six weeks in a short-leg cast. He then was allowed to progress to full weight-bearing as tolerated in a removable stirrup. The syndesmotic screws were removed at five months postoperatively. The patient was asymptomatic after screw removal. Serial radiographs showed a well-maintained reduction. The patient’s most recent follow-up was twenty-nine months following the index procedure. He had returned to playing Division-I college rugby and had no complaints or limitations.
Proceed to Discussion >>Reference: Gesink DS, Anderson JG. Over-tightening of the syndesmosis after ankle fracture: A case report. JBJS Case Connect. 2015 Oct 14;5(4):e85.
Two recent studies have revealed that malreduction of the syndesmosis after surgical fixation occurs with alarming frequency with both open and closed methods. The most common malreductions appear to be translational (lateral, anterior, and posterior) and rotational (both internal and external), but infrequent mention is made of medial translation or over-tightening of the syndesmosis. In a cadaver study, Tornetta et al. addressed the question of whether over-tightening of the syndesmosis is possible. Lag-screw syndesmotic fixation was performed on cadaveric ankle specimens in maximum plantar flexion after sectioning the Achilles tendon but leaving the remainder of the ankle ligaments and capsule intact. They found no significant difference in ankle range of motion before and after syndesmotic fixation. No mention was made, however, of whether there was any distraction at the tibiotalar joint in any of the specimens. A clinical study by Mukhopadhyay et al. evaluated nineteen ankles after syndesmotic fixation with the use of bilateral CT scans. Using a measurement they referred to as “MD” (mean diastasis of the injured side compared with the noninjured side), they found that two of nineteen ankles had CT evidence of over-reduction of the syndesmosis, although the clinical importance of this finding, if any, was not discussed. We present the case of an ankle fracture-dislocation in which the syndesmosis was reduced and fixed using a standard technique resulting in what appears to be over-tightening of the syndesmosis, with distraction of the tibiotalar joint and an increase in the tibiotalar clear space seen on postoperative radiographs. To the best of our knowledge, there are no other cases in the literature describing a similar occurrence of over-tightening of the syndesmosis resulting in distal talar translation. The study by Mukhopadhyay et al. suggests that, on the basis of their postoperative CT measurements, over-tightening is possible, although this appears to be the exception rather than the rule. Furthermore, the study by Tornetta et al. found no difference in ankle range of motion after lag-screw fixation of the syndesmosis with the ankle in plantar flexion; however, their study was performed with the capsule and all ligaments about the ankle intact. It appears that over-tightening of the syndesmosis to the point that it becomes clinically relevant is extremely uncommon, but on the basis of the present case, we believe it is possible. We theorize that subtle differences in anatomy between individuals in conjunction with a fracture-dislocation of the ankle with substantial disruption of the ankle capsule and supporting ligaments may allow over-tightening of the syndesmosis with distal talar translation in rare cases. We recommend careful scrutiny of the intraoperative mortise view of the ankle to evaluate for any potential distraction of the talus or increase in the tibiotalar clear space. When measurements of the tibiofibular clear space or tibiofibular overlap suggest excessive widening of the syndesmosis even in the presence of an anatomically reduced mortise, comparison radiographs of the contralateral ankle will help define the normal parameters for the syndesmosis in any particular patient. Contralateral radiographs of the ankle should therefore be considered as an important adjunct to the preoperative or intraoperative evaluation for ankle fractures with syndesmotic disruption.
Reference: Gesink DS, Anderson JG. Over-tightening of the syndesmosis after ankle fracture: A case report. JBJS Case Connect. 2015 Oct 14;5(4):e85.


Shortening of the fibula at the fracture site
Over-tightening of the syndesmosis
Osteochondral fracture of the talus
Impaction fracture of the distal part of the tibia
Lengthening of the fibula at the fracture site