A Fifty-one-Year-Old Man with a Knee Injury Following a Car Accident
July 6, 2016


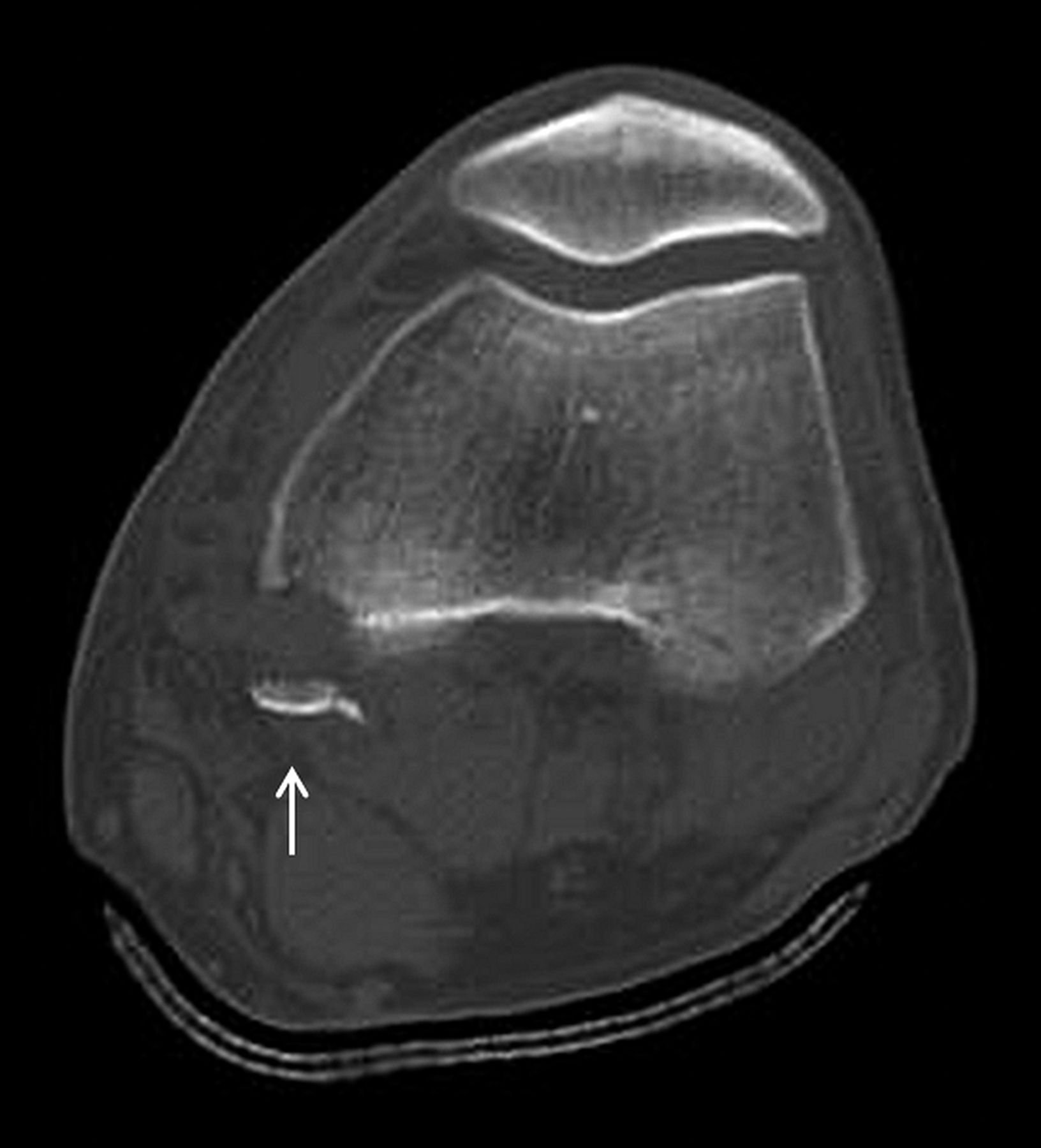



 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 4-A
Fig. 4-A Fig. 4-B
Fig. 4-B Fig. 5
Fig. 5 Fig. 6-A
Fig. 6-A Fig. 6-B
Fig. 6-BA fifty-one-year-old man was hit by a car while riding a motorcycle; he was immediately transferred to our hospital. At the initial examination, the left knee had dislocated posterolaterally. There was no neurovascular injury. Radiographs revealed complete posterior dislocation of the knee as well as a bone fragment in the posterior aspect of the femoral condyle (Figs. 1-A and 1-B). The inferior portion of the patella was also fractured. Computed tomography (CT) revealed a bone fragment in the popliteal space and the corresponding bone defect at the posterior part of the medial femoral condyle (Fig. 2-A). The anterolateral corner of the tibial plateau was depressed (Fig. 2-B). Magnetic resonance imaging (MRI) was obtained (Fig. 3-A). The anterior cruciate ligament (ACL), the posterior cruciate ligament (PCL), and the medial collateral ligament (MCL) all were completely torn. An intense signal change was present in the anterolateral corner of the tibial plateau (Fig. 3-B). Although the inferior pole of the patella was fractured, the patellar tendon remained intact.
The posterior dislocation of the knee was easily reduced manually; however, because of gross instability, the knee dislocated again, even after a cast had been applied. Therefore, surgical stabilization was performed five days after the injury. Under general anesthesia, the knee joint easily dislocated posteriorly (Fig. 4-A). Grade-3+ valgus instability was noteworthy at full extension and at 30° of flexion (Fig. 4-B). Arthroscopic inspection confirmed the complete ruptures of both the ACL and the PCL. The lateral meniscus was severely torn and interposed in the intercondylar space and was resected arthroscopically. The knee joint was exposed through a medial incision. The MCL was avulsed from the tibial attachment. The medial femoral and tibial condyles could be exposed easily because the joint capsule was severely torn. The bone fragment that was attached to the medial head of the gastrocnemius muscle was avulsed from the posterior part of the medial femoral condyle (Fig. 5). The fragment was reduced and fixed with a screw, which resulted in maintenance of joint reduction (Figs. 6-A and 6-B). Repair of the posteromedial joint capsule was impossible. The MCL was reattached to its tibial insertion by suture anchors, which restored valgus stability at full extension and at 30° of flexion. The depressed anterolateral corner of the tibial plateau was elevated, bone substitute was added for support of the articular fragment, and a screw was used for fixation. The patellar fracture was stable and required no surgical intervention.
The knee was immobilized in a cast for two weeks postoperatively; range-of-motion exercises were started thereafter. Partial weight-bearing was started at six weeks after surgery. One year postoperatively, the patient was able to ambulate without pain while wearing a soft PCL brace (Knee Grip PCL; ALCARE). Knee range of motion was from 0° to 125°. Grade-3 posterior instability and grade-3 anterior instability remained because of the insufficiency of the PCL and the ACL, for which a second-stage reconstruction is planned.
Proceed to Discussion >>Reference: Mio K, Matsuzaki K, Rikitake H, Nakaya T, Nemoto K, Chiba K. Avulsion fracture of the medial head of the gastrocnemius muscle associated with posterior dislocation of the knee: A case report. JBJS Case Connect. 2016 Apr 13;6(2):e24.
We present a rare case of avulsion fracture of the insertion of the medial head of the gastrocnemius muscle associated with posterior dislocation of the knee. Reduction and fixation of the fragment resulted in maintenance of joint reduction despite residual instability due to the multiligamentous injuries. The reduction of the bone fragment attached to the medial head of the gastrocnemius muscle was crucially important to regain stability of the knee.
Radiographs showed a bone fragment in the posterior aspect of the femoral condyle; however, its origin could not be detected initially. It was also difficult to identify the depression fracture of the anterolateral corner of the tibial plateau on radiographs. CT confirmed the origin of the avulsion fragment as well as the presence of the depression fracture of the anterolateral corner of the tibial plateau. MRI also clearly revealed the attachment of the medial head of the gastrocnemius muscle to the bone fragment, as well as the ligamentous disruptions. The anterolateral corner of the tibial plateau was depressed, and the posteromedial side of the knee was severely damaged. Therefore, we suspected that the knee had been hyperextended with concomitant severe valgus stress. Increased mechanical tension to the medial head of the gastrocnemius muscle by knee hyperextension and contraction of the gastrocnemius muscle likely produced the avulsion fracture. The medial gastrocnemius avulsion fracture contributed to the gross instability and difficulty in maintaining joint reduction.
For posteromedial stability of the knee, the PCL and the posteromedial capsule are important. The PCL is considered to be the primary restraint to tibial posterior subluxation at all angles of knee flexion apart from near full extension. The posteromedial capsule is shown to tighten and resist tibial posterior draw in the extended knee. We could not identify data confirming the contribution of the gastrocnemius muscle to posterior stability; however, the gastrocnemius muscle is considerably active on electromyograms in PCL-deficient knees.
Describing the treatment of an avulsion fracture of the medial head of the gastrocnemius muscle, Maehara and Sakaguchi reported a case that required surgery because of persistent pain. Patterson et al. reported another case that was treated nonoperatively because the patient had limited loss of range of motion and no substantial instability. In our patient, surgery was indicated because joint stability could not be obtained by casting alone. Considering the injury mechanism in this patient, restoration of the stability in the posteromedial corner of the knee was important. The fixation of the bone fragment to the medial femoral condyle prevented recurrent dislocation of the knee despite residual instability due to the multiligamentous injuries. Because this procedure was critical for maintenance of joint reduction, reconstruction of the PCL and the ACL was planned for a later date in order to prevent excessive arthrofibrosis and restriction in range of motion. This case indicates that the reattachment of a bone fragment that is attached to the medial head of the gastrocnemius muscle is crucially important to regain the stability of the knee.
Reference: Mio K, Matsuzaki K, Rikitake H, Nakaya T, Nemoto K, Chiba K. Avulsion fracture of the medial head of the gastrocnemius muscle associated with posterior dislocation of the knee: A case report. JBJS Case Connect. 2016 Apr 13;6(2):e24.





What is the diagnosis?
Popliteus tendon avulsion
Medial head of the gastrocnemius avulsion
PCL avulsion
Ligament of Wrisberg avulsion
Posterior horn of the medial meniscus avulsion