

 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4A fifty-six-year-old man presented with a three-month history of gradually worsening neck pain. The patient reported that the pain occasionally radiated to the right shoulder. He exhibited weakness with right arm flexion and right wrist dorsiflexion. On admission, he was afebrile. The C-reactive protein (CRP) level was <0.5 mg/dL, the erythrocyte sedimentation rate (ESR) was 17 mm/hr, and the leukocyte count was 8.6 × 103/μL, all within the normal range. Blood cultures on admission showed no growth after five days. The cardiac examination was unremarkable for any rhythm abnormalities or murmurs. We did not pursue a work-up for endocarditis because the patient did not have any clinical symptoms or laboratory abnormalities.
Notably, the patient reported a history of twelve surgeries on the right leg secondary to a motorcycle accident. He ultimately had required implant removal in the right foot because of osteomyelitis. These surgeries had been performed at a remote location and the records were not available to us. Additionally, the history was notable for hepatitis C, a 34-pack-year smoking history, and previous intravenous drug use (the latest had been seven months prior to admission). Radiographs were made (Fig. 1). Prior to presentation, the patient had undergone magnetic resonance imaging (MRI) without contrast at an outside hospital (Fig. 2).
The patient was diagnosed with osteomyelitis of C5 and C6. The patient underwent instrumented anterior spinal fusion from C5 to C7 with an anterior C5-C6 cervical discectomy, a C6 corpectomy with a Harms cage replacement, and spinal debridement. During the surgery, the C5-C6 disc space revealed purulent and necrotic tissue, and specimens were taken for culture. The C6 body appeared friable and unable to maintain implant purchase; hence, a corpectomy was performed and a Harms cage was placed with fixation to both C5 and C7. One week later, the patient underwent a C5-C7 instrumented posterior spinal fusion for stabilization of the C6 corpectomy (Fig. 3). Intraoperative cultures exhibited growth of Strenotrophomonas maltophilia. Susceptibility testing was performed in the laboratory. The minimum susceptible (S) inhibitory concentrations were reported as follows: levofloxacin, 0.5 S; trimethoprim/sulfamethoxazole (TMP-SMX), <20 S; and ticarcillin-clavulanate, 0.75 S.
The infectious diseases department was consulted, and the patient was discharged on TMP-SMX double strength (DS) (160 mg/800 mg three times a day) and levofloxacin (750 mg daily). At the six-week follow-up, the levofloxacin therapy was discontinued and the TMP-SMX DS therapy was reduced to twice a day. At that time, the ESR was 2 mm/hr and the CRP level was 0.11 mg/dL. The patient was instructed to continue the TMP-SMX therapy for an additional five months as suppressive treatment.
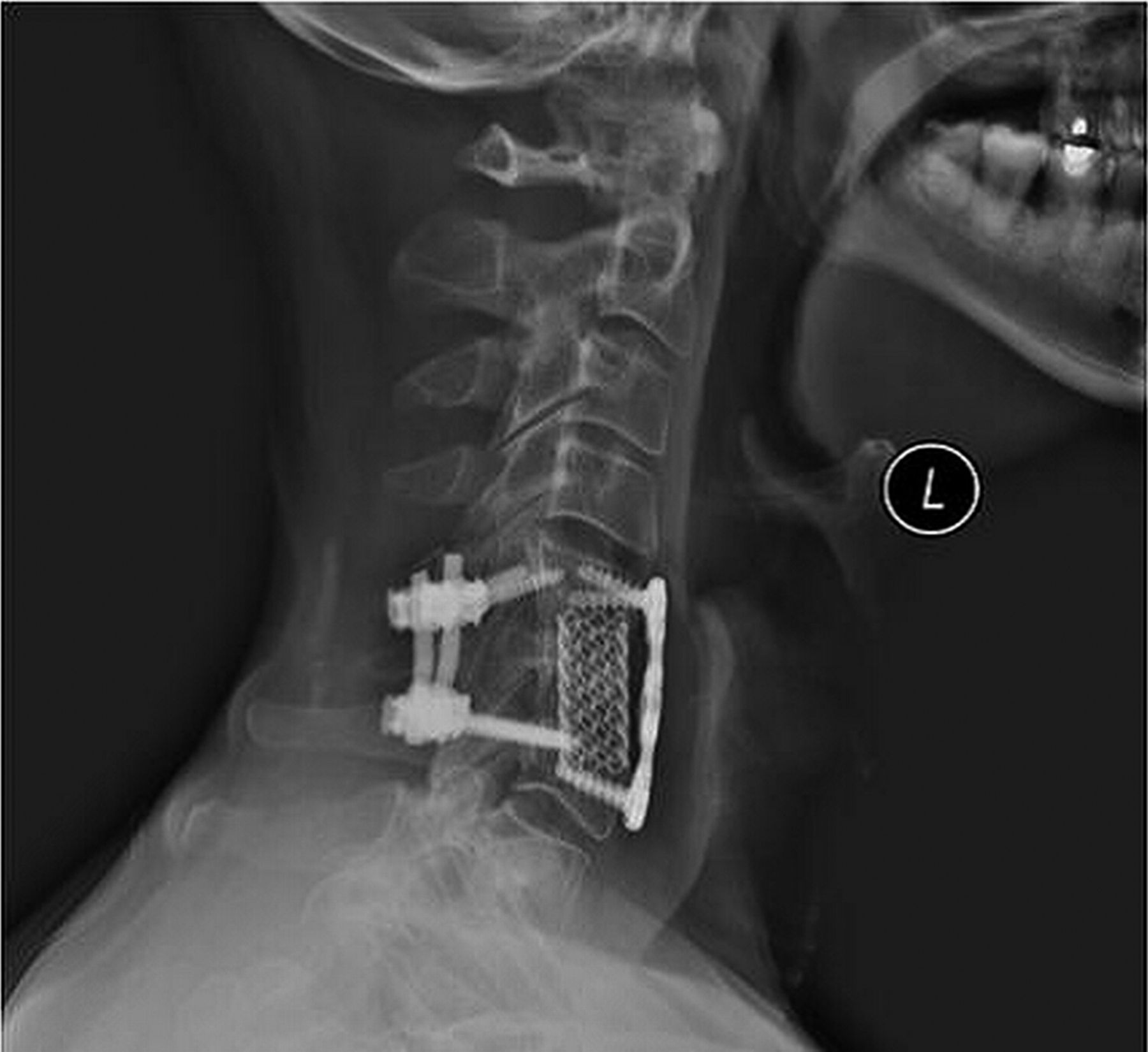
There were no complications during the postoperative course. The last follow-up was at twelve months postoperatively. At that time, the patient had no symptoms of arm pain and exhibited 5/5 strength bilaterally in the upper extremities. However, he did note that he had experienced intermittent tingling over the lateral aspect of the left side of the neck and face that had resolved spontaneously. Radiographs demonstrated that the instrumentation was in appropriate alignment without any loosening or migration (Fig. 4).
Proceed to Discussion >>Reference: Ilyas H, Tabaie S, Place H. Diagnosis, treatment, and outcome of Stenotrophomonas maltophilia discitis and cervical osteomyelitis: A case report and review of the literature. JBJS Case Connect. 2016 Apr 13;6(2):e23.
S. maltophilia is a gram-negative, nonfermenting bacillus that is ubiquitous and found in natural water reservoirs, in soil, and on plants. Originally isolated in 1944, it was previously identified as Bacterium bookeri, Pseudomonas maltophilia, Xanthomonas maltophilia, and, ultimately, S. maltophilia in 1993.
We are currently aware of four documented cases of osteomyelitis due to S. maltophilia. We are unaware of any reported cervical spine osteomyelitis with this organism or of vertebral infections with this organism that required surgical intervention. The patient in one of the documented cases had vertebral involvement in the lumbosacral spine, as described by Landrum et al. That patient had developed an S. maltophilia spine infection following two L5-S1 discectomies. The patient subsequently had been treated medically with six weeks of vancomycin and levofloxacin therapy. Two months after the initial presentation, the patient had developed relapse of osteomyelitis with the same organism and had been treated medically with six weeks of TMP-SMX and ticarcillin-clavulanate therapy, as well as a subsequent additional six months of TMP-SMX therapy. Two of the previously documented cases identify S. maltophilia osteomyelitis in association with a farm-machine-related injury (e.g., a corn-harvesting machine). Our patient did not reside in an agricultural environment and was unable to recall any traumatic events or injuries prior to becoming symptomatic. On multiple follow-up visits, however, he inquired about being able to return to riding a lawnmower and reported that as one of his preferred activities.
Our patient underwent prompt surgical treatment because of the presence of a neurologic deficit, evidence of extensive bone damage, and the presence of a retropharyngeal abscess. Between 44% and 59% of patients with cervical osteomyelitis present with a neurologic deficit. Additionally, in a literature review, Barnes et al. cited a case series in which 53% of cases presented with a paravertebral or epidural abscess. Although not utilized with our patient, MRI with gadolinium-based contrast would have been the preferred method of imaging because it best delineates collections of fluid, inflammation, and abscesses. Schimmer et al. identified that the presence of even one of these factors warrants surgical intervention as soon as possible. Given the notable prevalence of a neurologic deficit and the presence of an abscess in our patient, we believe that a large portion of cervical osteomyelitis cases warrant consideration for prompt surgical treatment.
Identifying the role of antibiotic management for vertebral osteomyelitis is challenging because of the lack of data. Currently, there are no guidelines in the United States or randomized controlled trials identifying specific treatments or duration of treatment. Determination of the duration of antibiotic treatment in our patient involved monitoring inflammatory markers, notably the CRP level, in the clinical course.
In conclusion, osteomyelitis of the cervical spine is rare but may have potentially catastrophic sequelae if not identified and treated promptly. A substantial proportion of patients present with a neurologic deficit or a paravertebral abscess. The presence of either scenario warrants consideration for surgical intervention and collaboration with an infectious diseases specialist. In our patient, osteomyelitis due to S. maltophilia was successfully treated with a combination of surgical debridement with cervical fusion and prolonged antibiotic treatment.
Reference: Ilyas H, Tabaie S, Place H. Diagnosis, treatment, and outcome of Stenotrophomonas maltophilia discitis and cervical osteomyelitis: A case report and review of the literature. JBJS Case Connect. 2016 Apr 13;6(2):e23.

What is the diagnosis?
Hemangioma of the vertebral bodies C5 and C6
Metastatic carcinoma of the C5 and C6
Giant cell tumor of C5
Osteomyelitis of C5 and C6
Osteoblastoma of C6