A 64-Year-Old Woman with a Slow Growth on the Leg
July 19, 2017





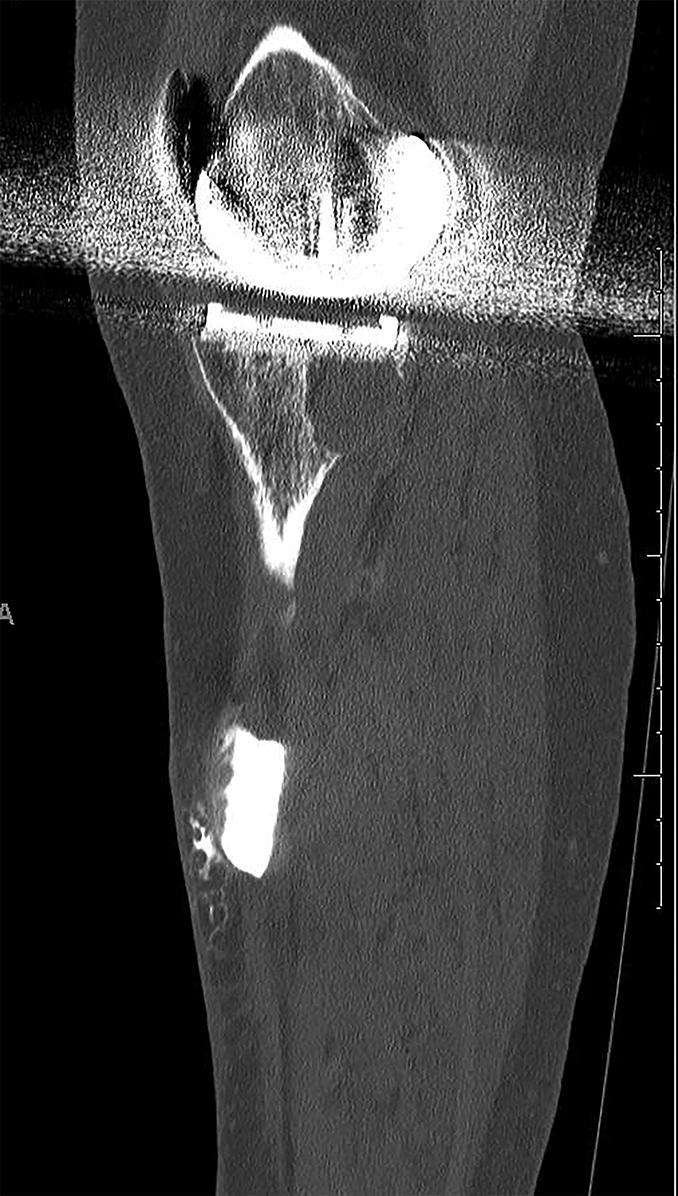
 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2-A
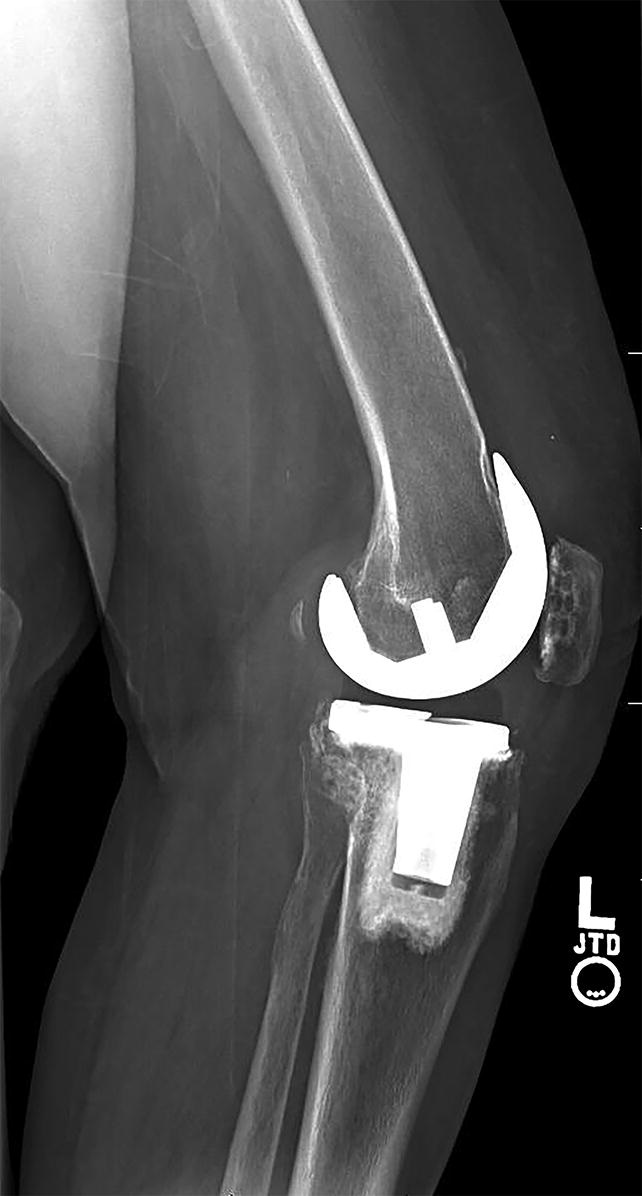
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 4-A
Fig. 4-A Fig. 4-B
Fig. 4-B Fig. 5-A
Fig. 5-A Fig. 5-B
Fig. 5-B Fig. 6-A
Fig. 6-A Fig. 6-B
Fig. 6-BA 64-year-old woman (height, 65 in [165.1 cm]; weight, 138 lb [62.6 kg]; body mass index [BMI], 23 kg/m2) with primary osteoarthritis had undergone bilateral total knee arthroplasty in 1998 at an outside institution. In December 2010, the patient presented to our tumor service with a large anteromedial soft-tissue mass of the left lower leg, which had been present for 1.5 years. The mass had started small, and grew at a slow rate over time. She first had noticed it while walking. There was no history of knee pain or swelling, and she indicated that she had no history of trauma, constitutional symptoms, infection, or malignancy.
On physical examination, well-healed scars from bilateral midline anterior longitudinal knee incisions were noted. On the left lower extremity, there was a 5 × 6-cm, nontender, immobile, very soft tissue mass medially at the midtibial level (Figs. 1-A and 1-B). There was no knee effusion, abnormal warmth, or apparent communication between the knee and the mass. The patient had full knee range of motion and a normal neurovascular examination.
Radiographs of the left knee demonstrated a tricompartmental hybrid posterior Cruciate Retaining (CR) NexGen total knee implant (Zimmer) (Figs. 2-A and 2-B). The femoral angle was 6° valgus, the tibial alignment was neutral, and the tibiofemoral angle was 6° valgus. There was no radiographic evidence of component loosening. There were radiolucencies in femoral lateral zones 1 and 3, but no evidence of mechanical loosening of the uncemented femoral component. The cemented metal-backed modular tibial component also had no evidence of loosening, and there was no evidence of a periprosthetic fracture. Magnetic resonance imaging (MRI) of the left leg with and without contrast revealed a homogeneous fluid-filled cyst extending down the anteromedial aspect of the leg. A bone scan showed no increased activity around the prosthesis or the mass. The white blood-cell (WBC) count was 8,300 cells/μL, the erythrocyte sedimentation rate was (ESR) 17 mm/hr, and the C-reactive protein (CRP) level was 1.2 mg/L, all within normal limits. At this point, the decision was made to proceed with aspiration of the cyst.
Ultrasound-guided aspiration of the cyst confirmed the presence of synovial fluid, with no evidence of malignancy or infection. Subsequent injection of radiopaque dye and a computed tomography (CT) arthrogram demonstrated considerable bone loss in the posteromedial aspect of the tibia beneath the modular tibial tray, consistent with osteolysis, as well as a small area of communication between the lower-extremity mass and the joint (Figs. 3-A and 3-B). Revision of the left total knee replacement was recommended.
An anterior midline longitudinal incision was made through a portion of the previous scar. Dissection was carried down through the subcutaneous tissues until the extensor mechanism was encountered. A deep incision was made with the medial parapatellar approach, entering the joint. We encountered clear synovial fluid, which was submitted as a culture specimen. A specimen of the synovial lining of the joint was submitted for frozen section analysis. Biopsy specimens were sent for evaluation.
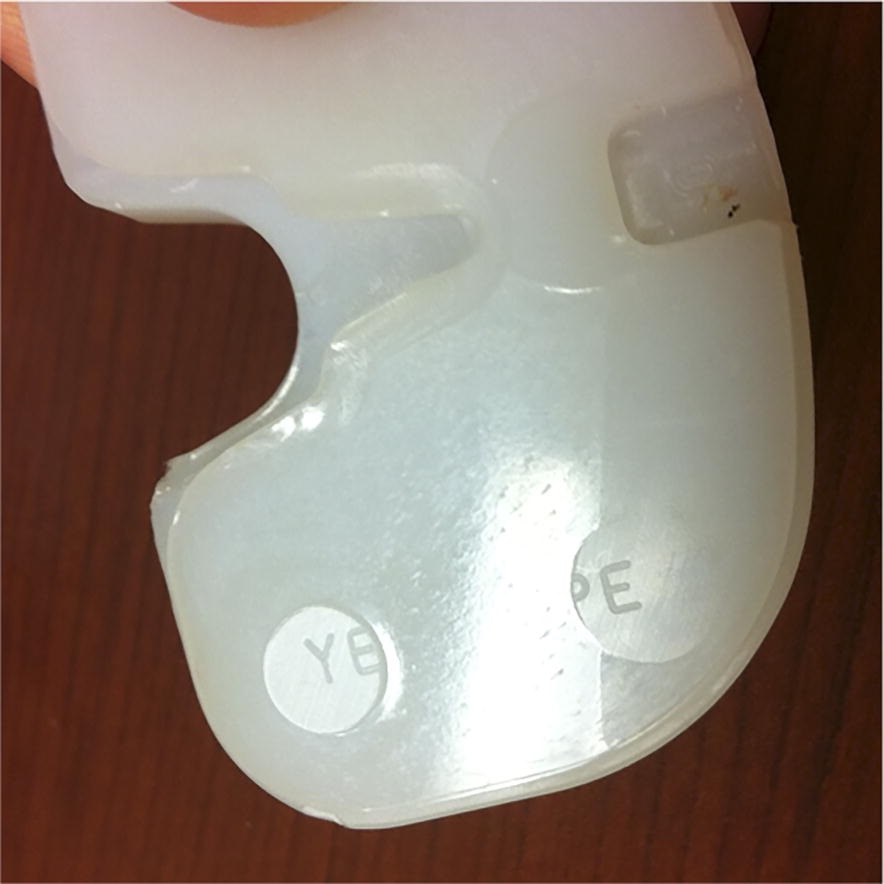
The polyethylene resin component (conventional polyethylene GUR 1050 gamma-sterilized in nitrogen) of CR design was easily removed from the tray. It demonstrated a 10-mm-thick size-4 insert with a direct compression-molded articulating surface with a machined undersurface. Examination of the insert revealed minimal wear, with polishing of the tibiofemoral articular surface. The peripheral groove on the polyethylene insert was in good shape, indicating that the locking mechanism was not compromised. Examination of the undersurface, however, demonstrated extensive backside wear in the posteromedial portion of the insert; there were elevated plateaus of polyethylene with the original markings where there were baseplate screw holes, but these were surrounded by areas with missing material (Figs. 4-A and 4-B).
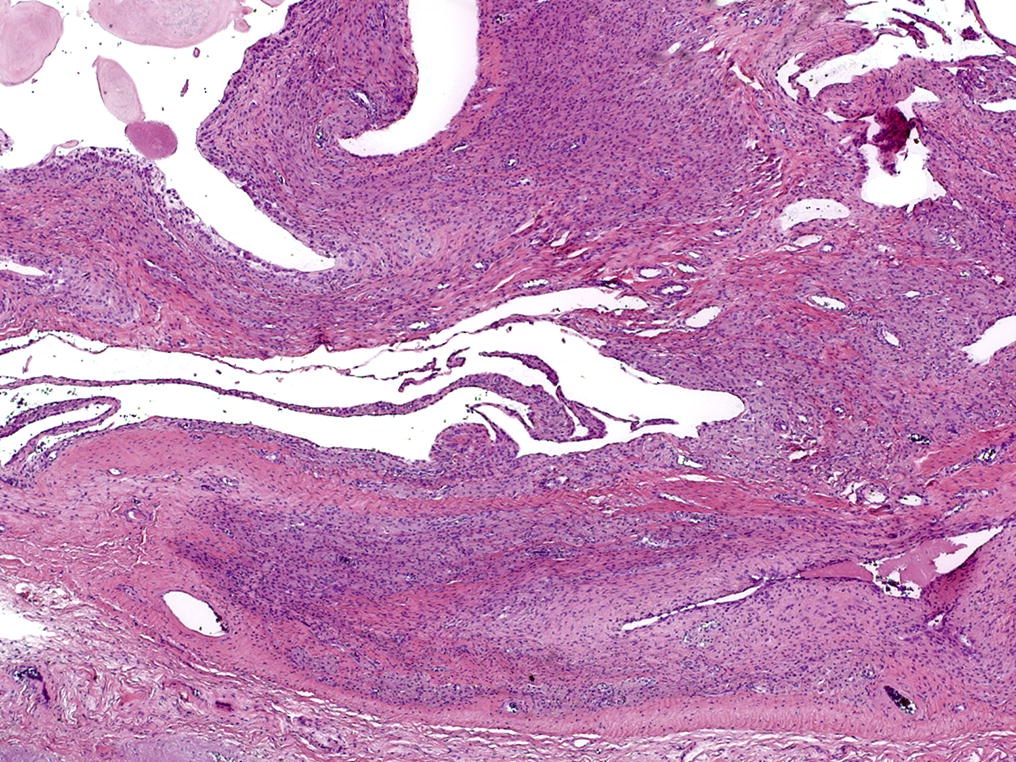
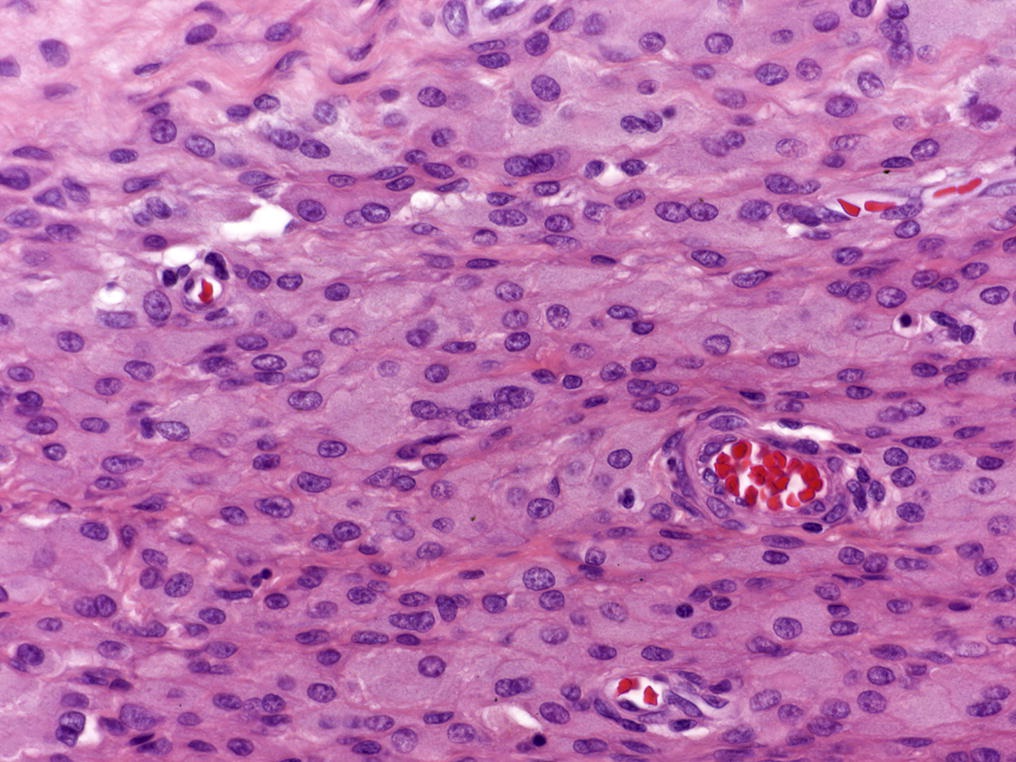
Next, a synovectomy was performed. Soft tissue was elevated off of the proximal-medial aspect of the tibia. The extensor mechanism was shifted laterally, and the knee was flexed. The knee was well balanced, and the 3 components of the replacement were all solidly fixed, with no evidence of mechanical loosening. The polyethylene insert was removed from the tibial tray. Examination of the insert revealed some polyethylene wear on the articular surface of the plastic, but more impressive loss of material on the backside of the posteromedial portion of the tibial insert (Figs. 4-A and 4-B). The patient was diagnosed with wear debris reaction. Probing of the posteromedial corner of the tibia with a curet revealed a channel that was dissecting into a bone-cyst defect underneath the tibial component. A blunt clamp was used to probe down into the cystic lesion of the anterolateral tibial region. Once the cyst was entered, a copious amount of thick purplish-brown fluid was evacuated through the knee joint. The cyst was irrigated with pulsatile lavage through the channel communicating with the joint. Fluid specimens encountered while probing the cystic bone lesion posteromedially, as well as fluid specimens from the tibial soft-tissue cystic mass, were obtained. This area was curetted again and irrigated thoroughly, and bone-grafting with allograft chips was performed. The pathology report on the intraoperative fluid samples confirmed tiny fragments of fibrous tissue with sheets of macrophages, consistent with the preoperative aspiration analysis, consistent with the preoperative aspiration analysis (Figs. 5-A and 5-B).
A new size-4 10-mm-thick Prolong Highly Crosslinked Polyethylene insert (Zimmer) was implanted (Figs. 6-A and 6-B). The patient had an uneventful postoperative course, and there were no signs of infection or recurrence of the cyst at the follow-up visits. A telephone survey was performed 4 years after the revision surgery. The patient stated that the knee had remained pain-free with excellent range of motion and no recurrence of the mass.
Proceed to Discussion >>Reference: Sabeh K, Carter A, Rosenberg AE, Robinson R. Diaphyseal tibial soft-tissue mass after total knee arthroplasty: a case report. JBJS Case Connect. 2017 May 10;7(2):e28.
There is a paucity of literature describing extra-articular soft-tissue masses forming as a result of osteolysis and wear debris consisting of polyethylene particulate material. The initial evaluation of a mass in the setting of a total knee arthroplasty encompasses a broad differential diagnosis, including benign or malignant lesions, infection, metallosis-reactive granulomas, and osteolysis. The differential diagnosis for benign lesions includes, but is not limited to, lipomas, peripheral nerve sheet tumors, giant cell tumors of the tendon sheath, hemangiomas, and myxomas. Malignant lesions include soft-tissue sarcomas (mainly synovial sarcomas, fibrosarcomas and liposarcomas, malignant peripheral nerve sheath tumors, muscle tumors such as leiomyosarcomas, and angiosarcomas). To our knowledge, there have been only a few prior studies and reports of masses as a result of osteolysis after total knee arthroplasty. In 1 study, Vernon et al. demonstrated an osteolytic cystic lesion extending into the tibial diaphysis, but there was no mention of a soft-tissue component.
Osteolysis in and of itself can mimic infection or septic arthritis, presenting as a tender, warm, and swollen joint or an abscess-like swelling around the joint. In those instances, a step-by-step approach is warranted, which includes laboratory testing (WBC count with differential, ESR, and CRP level), radiographs, MRI, and bone scans; if there is a concern for communication with the joint, a CT arthrogram can be valuable. A CT arthrogram was performed in our case (after the laboratory testing, MRI, and bone scan had ruled out malignancy), revealing the presence of communication between the knee joint and the diaphyseal mass (Figs. 3-A and 3-B).
The patient described herein had a normal BMI of 23 kg/m2, was only modestly active, had received a 10-mm-thick insert with the initial total knee arthroscopy (which had been performed 12 years earlier), and had a well-fixed, well-aligned implant. The implant was a CR NexGen total knee of conventional polyethylene (GUR 1050 gamma-sterilized in nitrogen). Survivorship of this implant has been described by Park and Kim, who reported no cases of osteolysis in 100 total knee replacements at the 14-year follow-up. Similarly, Hack et al. reported only 1 case of lateral tibial osteolysis without loosening of the component at the 10-year follow-up of 224 patients with total knee arthroplasty. Additionally, we performed an extensive literature search, and, to our knowledge, there are no reports of this particular implant causing osteolysis listed on the Manufacturer and User Facility Device Experience (MAUDE) database or other data registries.
The generation of polyethylene wear particles can originate from the tibial bearing surface, the tibial post, the patella, and the undersurface of the tibial insert (backside wear). There are multiple factors that can influence the generation of polyethylene wear debris in modular total knee replacements. These include patient factors (e.g., body weight and activity level, which determine the amount of load across the joint), knee and implant alignment, length of implantation, type of polyethylene, insert sterilization, insert thickness, articular surface geometries, and the tibial insert locking mechanism. Minor deviations in the mechanical axis and the coronal and sagittal planes, as well as rotational malalignment, can lead to eccentric wear and generation of wear debris.
Modular designs have allowed surgeons to have various options while performing a total knee arthroplasty. However, this comes at a price of increased wear between the backside of the nonarticulating surface of the polyethylene insert and the metal tibial tray. This modularity, as well as the mechanism used to lock the insert in the tray, can lead to inevitable micromotion at the interface. This micromotion results in increased propensity for wear by virtue of creating polyethylene particles. Subsequently, macrophages and other inflammatory cells exposed to these particles produce proinflammatory cytokines, leading to increased osteoclastic activity, bone resorption, and, ultimately, osteolysis, as in our patient.
In summary, this case report describes an unusual presentation of osteolysis as a mid-diaphyseal soft-tissue mass in the distal aspect of the tibia without any knee joint symptoms or findings indicative of component loosening on physical examination. Failure of this implant occurred 12 years after the index procedure in a healthy, thin, and relatively sedentary patient with a well-aligned implant. We believe that the primary contributing factor to failure in this case likely was the generation of polyethylene wear debris due to relative micromotion between the conventional polyethylene insert and the modular tibial component.
Reference: Sabeh K, Carter A, Rosenberg AE, Robinson R. Diaphyseal tibial soft-tissue mass after total knee arthroplasty: a case report. JBJS Case Connect. 2017 May 10;7(2):e28.


What is the diagnosis?
Plasmacytoma
Wear debris reaction
Pigmented villonodular synovitis
Staphylococcus epidermidis infection
Hemangioma of bone