A 50-Year-Old Woman with Painful Swelling of the Knee and Calf
February 6, 2019
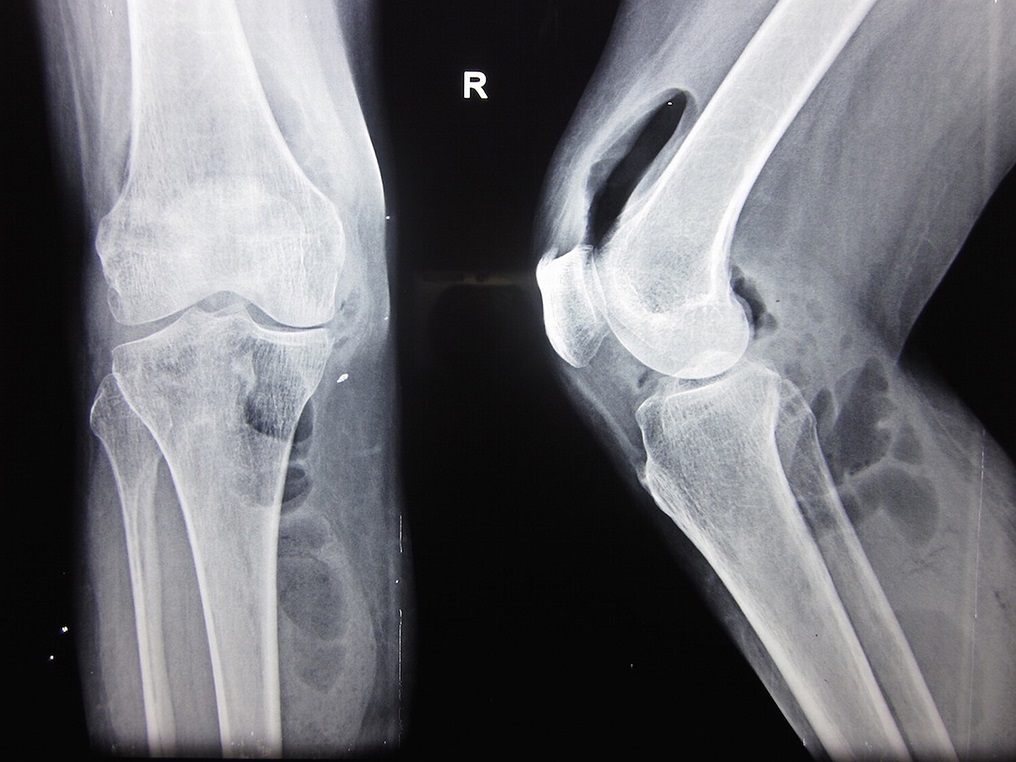
 Fig. 1
Fig. 1 Fig. 2
Fig. 2A 50-year-old woman presented to the emergency department with a painful swelling of the right knee and proximal part of the calf that she had had since 4 days earlier and high-grade fever since 2 days earlier. She had type-2 diabetes, which was being treated with 2.5 mg of glibenclamide daily. Her vital signs were stable. Local examination revealed a swelling, predominantly in the suprapatellar and posteromedial aspect of the proximal part of the calf. There were dilated veins over the suprapatellar region. The knee was tender on palpation, with redness, warmth, and fine crepitus. Range of motion was severely restricted and painful.
Initial laboratory data included a WBC (white blood-cell) count of 16,500/mm3 and a differential count of 90% polymorphonuclear cells with toxic granules and band forms and 10% lymphocytes. The ESR (erythrocyte sedimentation rate) was 80 mm/hr and the CRP (C-reactive protein) level was 94 mg/dL. Coagulation studies showed that the PT (prothrombin time) was 14.3 sec and the INR (international normalized ratio) was 1.07. A random blood sugar level was 449 mg/dL, and Hb (hemoglobin) A1c was 9.5%. Renal function tests showed that the BUN (blood urea nitrogen) was 39.1 mg/dL and serum creatinine was 2.6 mg/dL. Electrolytes were in the normal ranges.
A radiograph of the right knee revealed gas shadows in the suprapatellar pouch and in the soft tissues of the posteromedial aspect of the proximal part of the calf (Fig. 1). Ultrasound showed a collection of gas in the proximal part of the calf and the suprapatellar pouch. An arthrotomy was performed and partially necrotic synovium was debrided. There was a tear in the posterior capsule of the knee through which the joint space was communicating with the collection in the calf.
Gram staining of the sample showed an abundance of neutrophils and a few gram-negative bacilli.
The patient was diagnosed with septic arthritis, likely caused by an organism of the Enterobacteriaceae family. Clinical features, radiographic findings, serologic test results, and the high concentration of neutrophils in the debrided tissue indicated septic arthritis due to a gas-producing organism. The Gram stain showed gram-negative bacilli, providing an important clue to guide early antimicrobial therapy. Staphylococcus bacteria are gram-positive cocci, and Cutibacteria (formerly Propionibacteria) are gram-positive rods. Mycobacteria are slender rods that stain red with the acid-fast stain and are positive with the Gram stain. Several species of Enterobacteriaceae are gram-negative bacilli and are known to produce gas, therefore representing the most likely family of pathogens in this case.
The patient was started on 1.5 g of intravenous cefuroxime administered twice daily. On the third day, Citrobacter freundii was isolated on culture, and it was sensitive to cefuroxime. Intravenous cefuroxime was continued for 3 weeks, followed by oral cefuroxime for another 3 weeks. The patient’s initial postoperative course was uneventful. Range-of-motion exercises were started during the second week postoperatively. The wound healed at 2 weeks after surgery. However, the patient developed acute renal failure during the third week, which was treated by a nephrologist with fluid management and hemodialysis for 2 weeks. The patient’s creatinine level returned to 3.8 mg/dL. At the time of discharge (the eighth week of hospitalization), the range of knee motion was 0° to 100°, with mild terminal pain. At the 24-month follow-up, the range of knee motion was 0° to 130°. A radiograph at 2 years showed mild osteoarthritic changes (Fig. 2).
Proceed to Discussion >>Reference: Nemade PS, Aggarwal RA, Pisal T, Roy K. Emphysematous septic arthritis of the knee caused by Citrobacter freundii: a case report and review of the literature. JBJS Case Connect. 2016 Apr-Jun;6(2):e51.
Emphysematous septic arthritis is a rare condition. Few cases with gas collection in or around the joint associated with septic arthritis have been reported in the literature. Clostridium species, Streptococcus milleri, and members of the Enterobacteriaceae family such as Escherichia coli, Klebsiella pneumoniae, and Serratia liquefaciens were the causative organisms reported in the previous cases. To our knowledge, the current report is the first to describe emphysematous septic arthritis caused by C. freundii.
Members of the Citrobacter genus are gram-negative, aerobic (facultatively anaerobic), non-spore-forming, nonencapsulated, motile rods belonging to the family Enterobacteriaceae and are frequently found in the gastrointestinal flora of human beings. They ferment glucose and other carbohydrates, with the production of acid and gas. Citrobacter has 11 different species, of which C. freundii and C. diversus have been recognized as etiological agents in humans. Citrobacter infections are usually found in neonates, immunocompromised hosts, and debilitated elderly patients. Neonatal Citrobacter infections include meningitis and cerebral abscesses and are not associated with any particular underlying conditions. As an opportunistic pathogen in the immunocompromised and elderly, it commonly causes infections of the urinary tract, respiratory tract, wounds, bone, peritoneum, endocardium, meninges, and intestines.
C. freundii rarely causes bone and joint infection. In a large case series on Citrobacter infections by Lipsky et al., 3.7% of isolates were from patients with osteomyelitis. Most of them were isolated as a part of polymicrobial flora. Chuang et al. reported a case of necrotizing fasciitis and osteomyelitis due to a cefotaxime-resistant strain of C. freundii. The pathogenesis of reported Citrobacter infections of bones and joints appeared to be by direct extension to bone from an infection in contiguous soft tissue in patients with vascular compromise.
Septic arthritis due to C. freundii is extremely rare; to our knowledge, only 2 cases of C. freundii septic arthritis have been reported. Bruehl and Listernick reported a case of septic arthritis of the elbow in an 8-month-old infant due to C. freundii. The patient was treated with aspiration of pus from the elbow followed by parenteral cephalosporins for 2 weeks, and completely recovered without any sequelae. Stricker et al. reported a case of septic arthritis and osteomyelitis of the elbow in a previously healthy 5-year-old boy caused by dual infection with C. freundii and Haemophilus influenzae type b. The patient was treated successfully with intravenous fosfomycin for 4 weeks and had a good outcome. In contrast to osteomyelitis, both of these cases had a hematogenous mode of infection.
C. freundii is a notorious pathogen, and studies have shown that many isolates tend to be multi-drug-resistant. A recent study showed that nearly 54% of isolates had extended-spectrum beta lactamase production. Penicillin, ampicillin, and first-generation cephalosporins were found to be ineffective against C. freundii. Sensitivity to piperacillin-tazobactam ranged from 59% to 90%. A recent study showed that 100% of isolates were sensitive to imipenem. Because of the varied sensitivity pattern and high rate of drug resistance, we recommend that treatment should be individualized to each patient on the basis of culture and sensitivity testing.
Diabetic patients are known to develop “emphysematous” infections such as emphysematous pyelonephritis, emphysematous cystitis, emphysematous cholecystitis, and emphysematous epididymo-orchitis. Diabetes is the most common comorbidity associated with emphysematous septic arthritis. Huang and Tseng analyzed the gas produced in patients with emphysematous pyelonephritis and found large amounts of hydrogen and carbon dioxide in most cases. They concluded that mixed acid fermentation by Enterobacteriaceae and butyric acid fermentation by anaerobes produced these byproducts, which accounted for gas production in tissues in cases of emphysematous urinary tract infections. Yang and Shen hypothesized that the gas chamber production in tissues is a process that involves increased gas production, impaired transportation of gas by vascular compromise, creation of a gas chamber, equilibrium of the gas chamber and tissue gas, and expansion or collapse of the gas chamber. In our patient, the presence of glucose in the joint fluid due to the uncontrolled diabetes coupled with an immunocompromised state and poor vascularity provided an excellent medium for growth of bacteria followed by production and subsequent accumulation of gas in the joint cavity. Because of the excess pressure in the joint cavity, the gas escaped into the posteromedial aspect of the calf through the tear in the joint capsule.
In conclusion, we report a case of emphysematous septic arthritis, in a 50-year-old woman with uncontrolled diabetes, caused by C. freundii infection. The constellation of clinical signs and symptoms was characteristic. The patient recovered well following an arthrotomy and treatment with antibiotics. To our knowledge, this is the first described case of emphysematous septic arthritis caused by C. freundii.
Reference: Nemade PS, Aggarwal RA, Pisal T, Roy K. Emphysematous septic arthritis of the knee caused by Citrobacter freundii: a case report and review of the literature. JBJS Case Connect. 2016 Apr-Jun;6(2):e51.

What is the diagnosis?
Septic arthritis, likely caused by an organism of the Enterobacteriaceae family
Septic arthritis, likely caused by a Staphylococcus organism
Septic arthritis, likely caused by Cutibacterium (formerly Propionibacterium)
Soft-tissue aneurysmal bone cyst extending into the joint
Septic arthritis, likely caused by Mycobacteria