A 37-Year-Old Man with Continuing Left Knee Pain
January 2, 2019
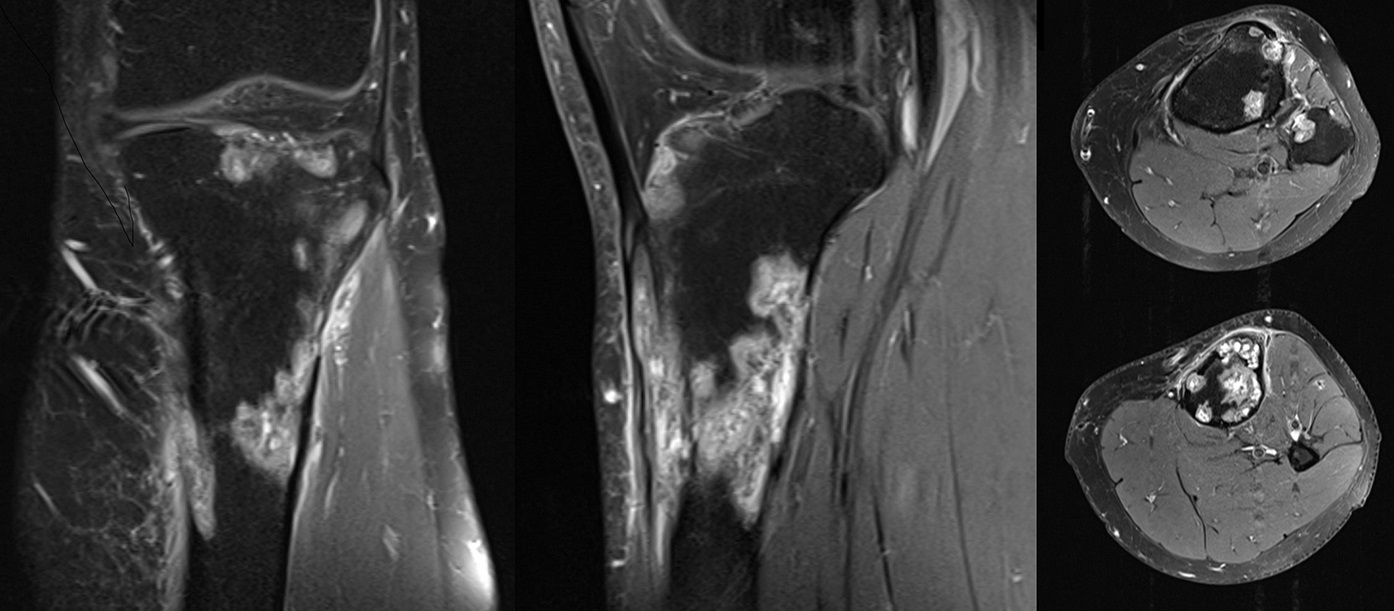
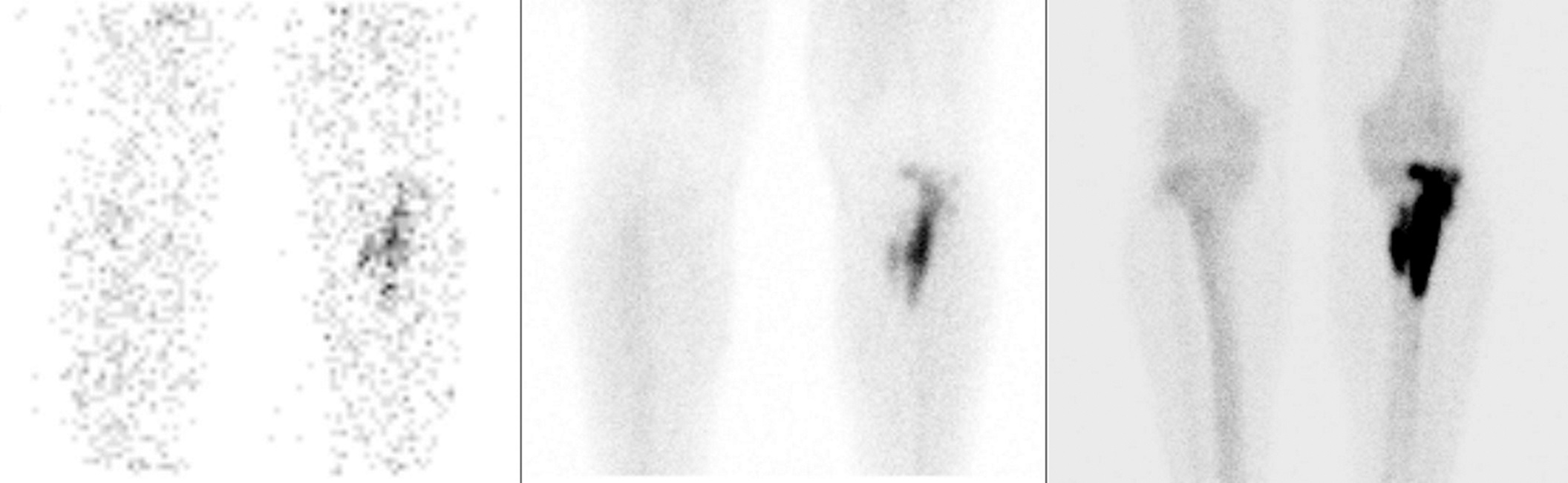


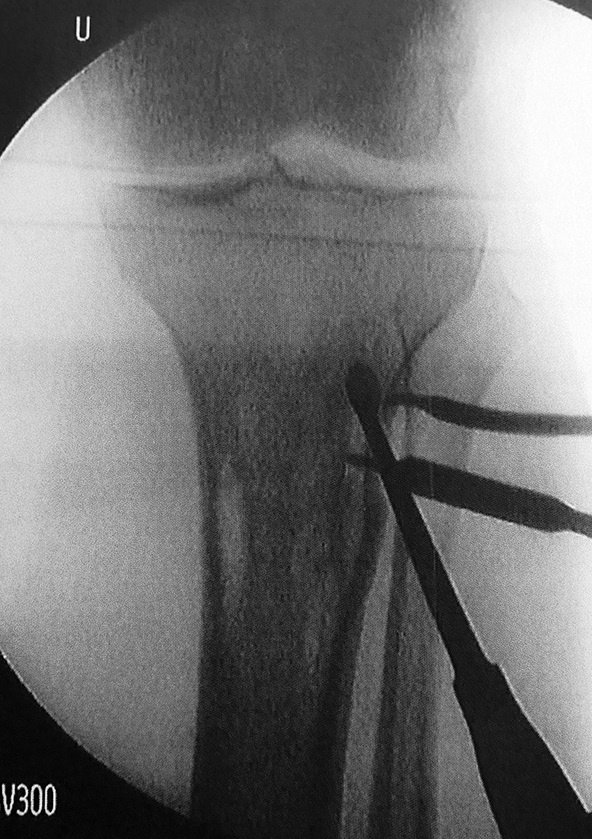
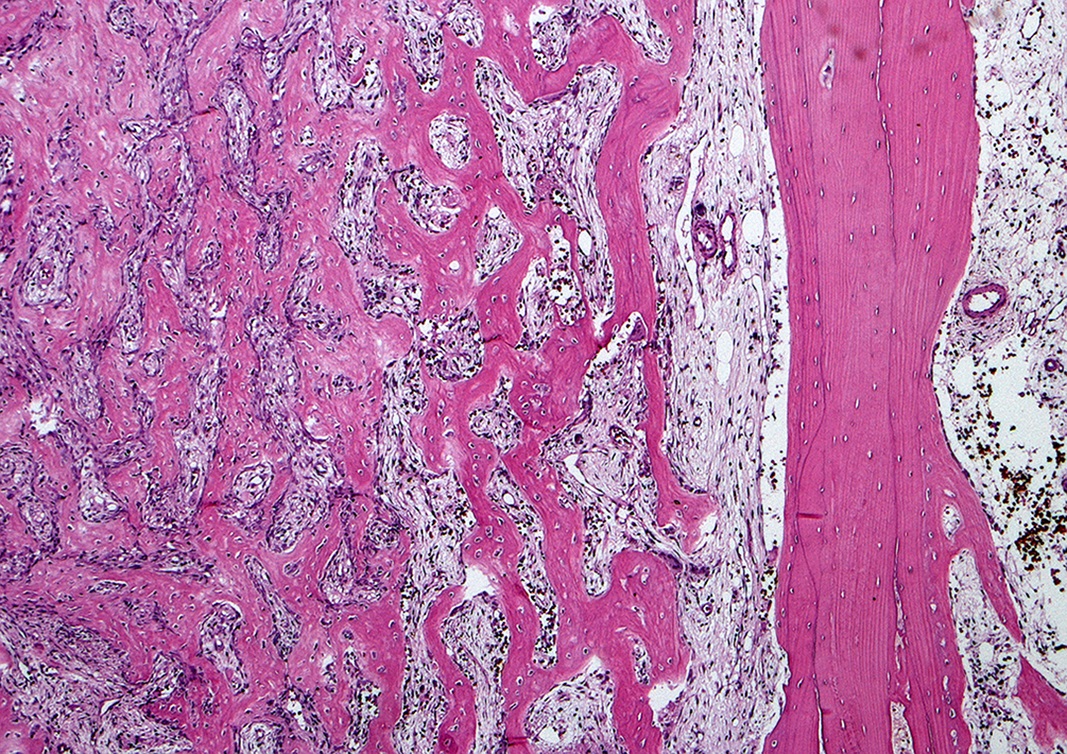
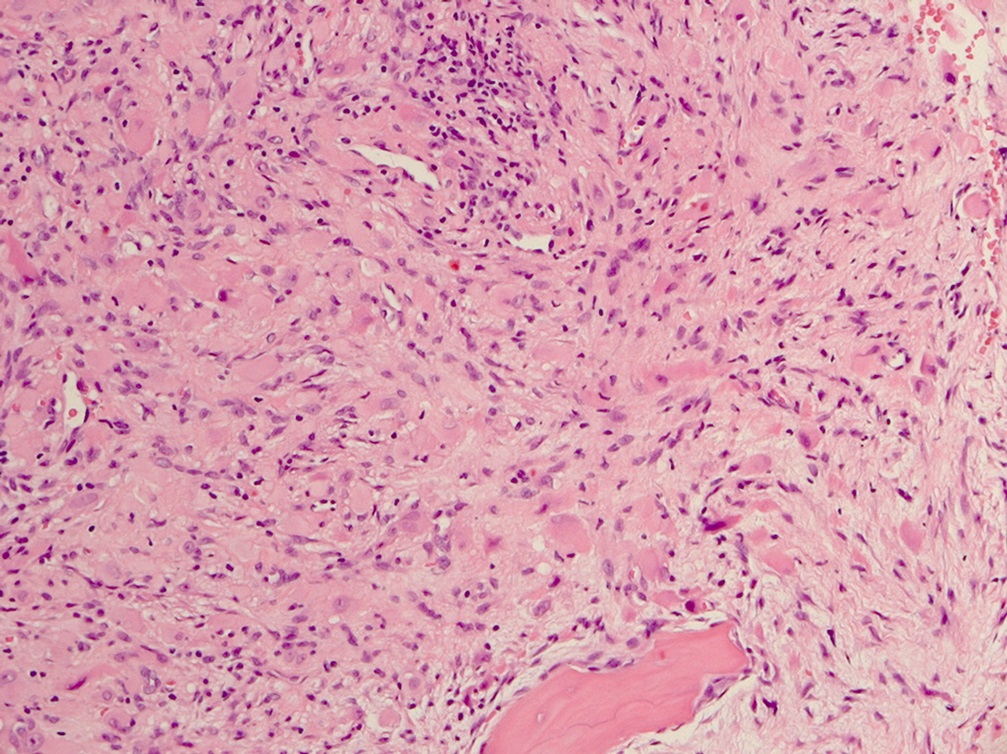
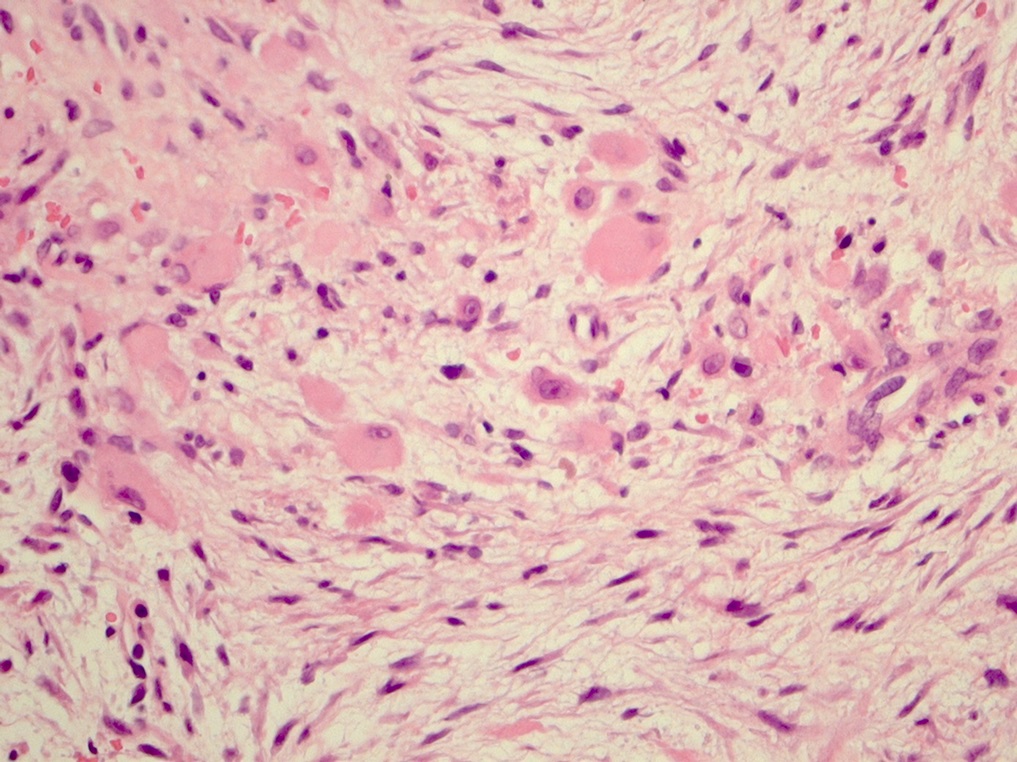
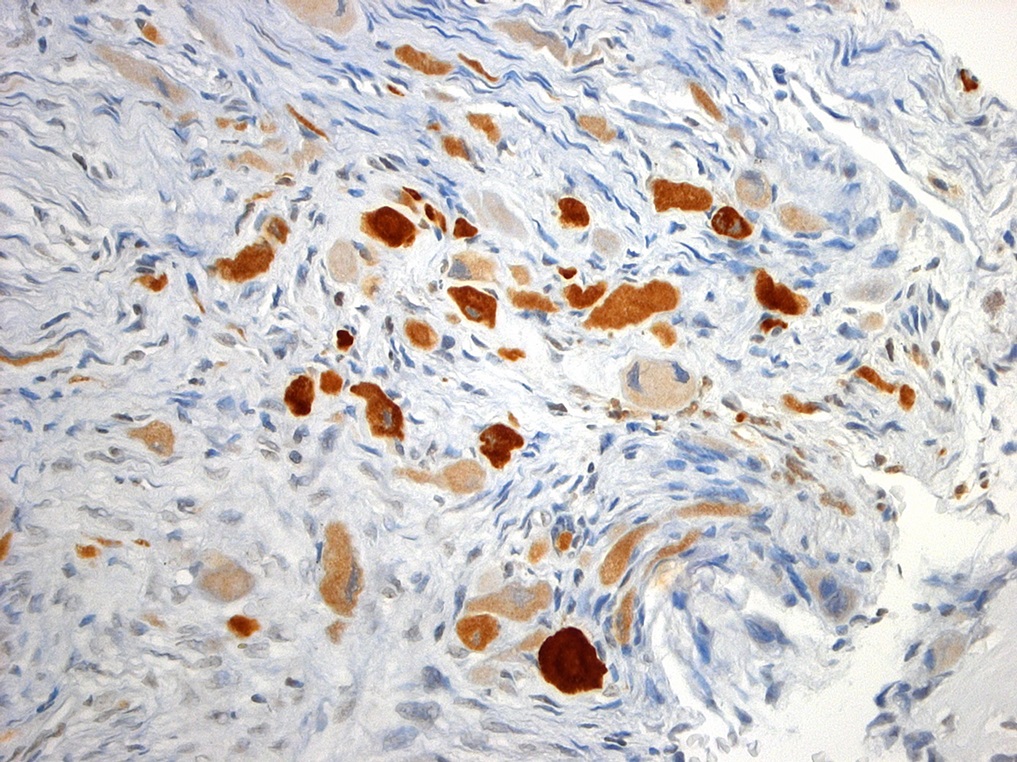
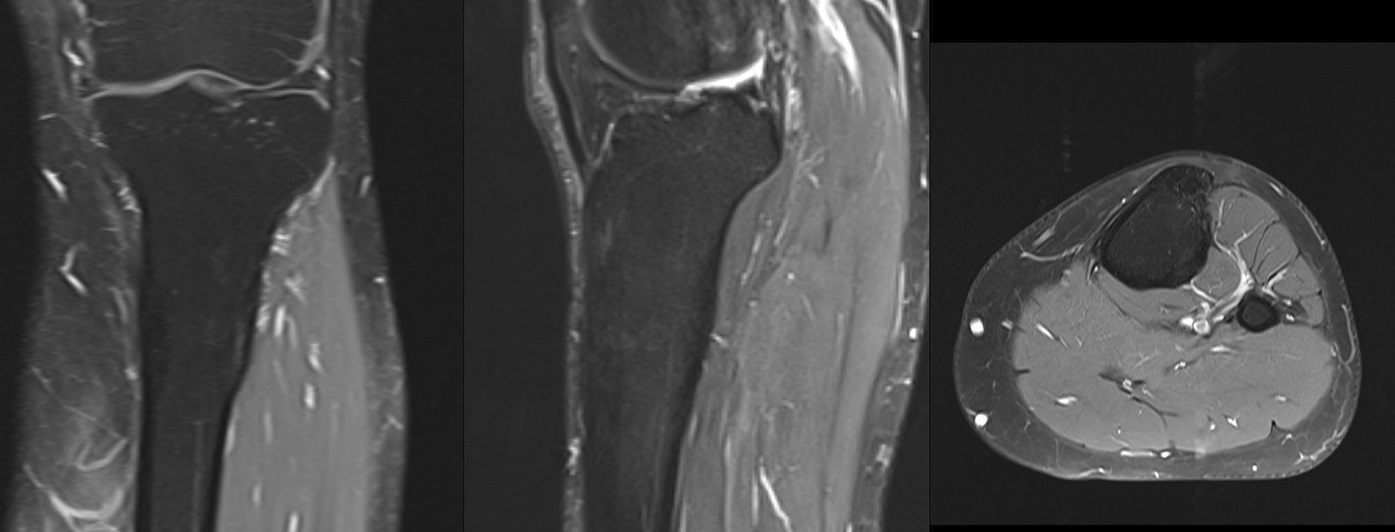
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 6
Fig. 6 Fig. 7
Fig. 7 Fig. 8
Fig. 8 Fig. 9
Fig. 9 Fig. 10
Fig. 10 Fig. 11
Fig. 11 Fig. 12
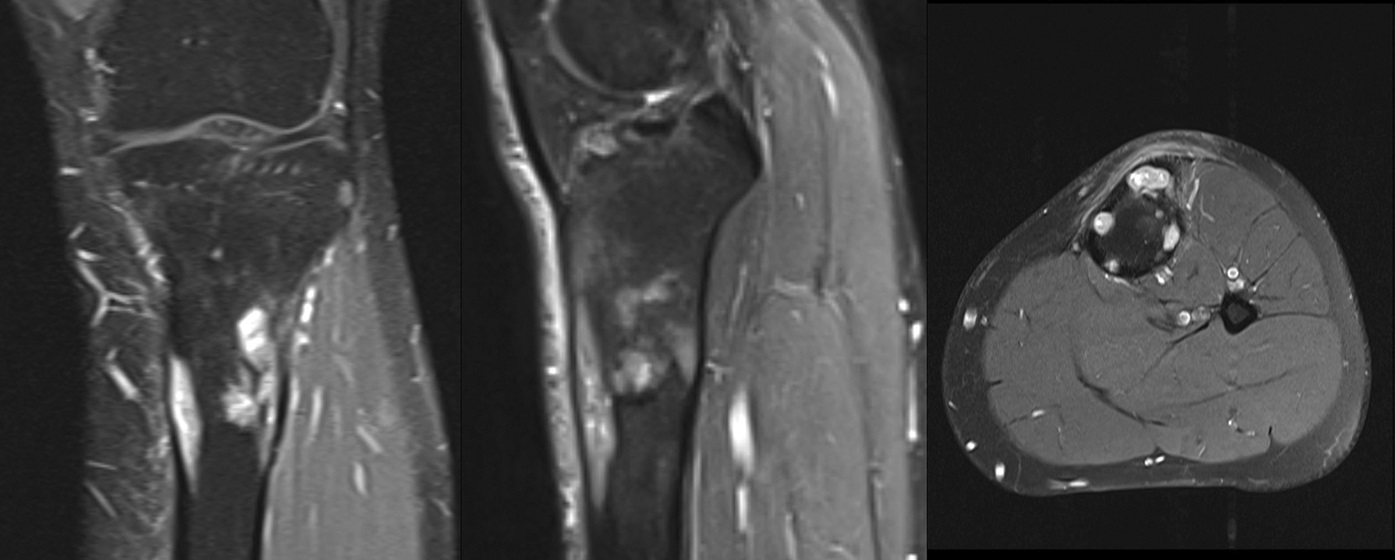
Fig. 12A 37-year-old man with no prior symptoms sustained a rotational injury to the left knee while running down stairs in October 2009. Because of continuing pain, magnetic resonance imaging (MRI) was performed; it showed multifocal, partially confluent osteolytic lesions in the proximal dia-meta-epiphyseal region of the tibia, as well as a focal lesion in the proximal fibular metaphysis, which exhibited similar signal characteristics. Cortical breakthrough was seen at the tibial tuberosity and at the fibula into the tibiofibular joint (Fig. 1). A bone scan that was performed 6 weeks later showed high technetium-99m (99mTc) uptake in all 3 phases (Fig. 2). Radiographs showed osteolytic lesions that corresponded with the MRI findings (Fig. 3).
A percutaneous core needle biopsy performed in January 2010 showed foci of increased, nonspecific osteoblastic and osteoclastic activity, and 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) showed focal activity of the osteolytic lesions that corresponded with the MRI of the tibia and the fibula (Fig. 4). To achieve a definitive diagnosis, an open biopsy was performed in February 2010 (Fig. 5).
Histology revealed lamellar bone with cortical thinning and large adjoining areas of reactive woven bone that were embedded in a fibrocellular stroma with prominent osteoblasts. Multiple confluent islands of fibrous stroma contained scattered groups of plump eosinophilic cells. An immunohistochemical panel found that these cells strongly expressed vimentin and pan-cytokeratin (Figs. 6 through 9), but were negative for epithelial membrane antigen (EMA), CD68, CD31, desmin, and actin.
Based on the clinical, imaging, and histologic findings, the diagnosis of osteofibrous dysplasia (OFD) with rhabdoid elements was made.
Two weeks following the open biopsy, the patient was pain-free. Because the lesions had been discovered incidentally after the rotational injury of the knee injury, we decided to proceed with observation.
MRI that was acquired 3 months later (Fig. 10) showed marked regression of the different foci, and the most recent imaging (Figs. 11 and 12) showed complete regression and reconstituted bone. At the 7-year follow-up in August 2017, the patient was asymptomatic and pain-free.
Proceed to Discussion >>Reference: Exner GU, von Hochstetter AR, Pfirrmann CWA. Osteofibrous dysplasia with rhabdoid elements in a 38-year-old man with spontaneous regression over five years: a case report. JBJS Case Connect. 2018 Jul-Sep;8(3):e51.
OFD, also known as a Kempson-Campanacci lesion, is a rare, benign fibro-osseous lesion that predominantly affects the tibia. Classic adamantinoma is a malignant biphasic tumor with nests or sheets of epithelial cells that are surrounded by spindle cells with an osteofibrous component. OFD-like, or differentiated, adamantinoma differs in that the keratin-expressing epithelial cells are present as small scattered groups that are visible with hematoxylin and eosin staining; however, they may be so sparse that they are overlooked unless they are rendered visible with immunohistochemical staining for keratin. Classic and OFD-like adamantinomas share similarities in location and appearance, making their distinction even more complicated. There is some controversy regarding distinguishing differentiated adamantinoma from the classic form with regard to the amount of epithelial component that is compatible with the differentiated form and whether progression from differentiated to classic adamantinoma can occur.
Accordingly, there is no consensus regarding the best treatment for OFD. Campanacci and Laus recommended delaying surgery as long as possible because of frequent spontaneous regression. However, based on an analysis of 16 patients, Lee et al. recommended radical extraperiosteal excision in all cases of OFD. An analysis of 73 patients (42 with OFD) with follow-up for >3 years revealed no evidence of progression from OFD to adamantinoma. Resection with clear margins was deemed necessary only for patients with classic adamantinoma.
To our knowledge, this is the second described case of OFD with rhabdoid elements. In a prior case, a 25-year old man with a localized lesion in the fibula was diagnosed with differentiated adamantinoma with rhabdoid elements; he had been treated with resection. At the 34-month follow-up, the patient was well, and there was no evidence of recurrence or metastasis. Our patient, who had only a limited open biopsy and no additional intervention, showed complete regression of the lesion.
Although it is generally accepted that there is a spectrum of OFD ranging from OFD-like adamantinoma to “classic” adamantinoma, the terminology is somewhat confusing. In light of the analysis of 73 consecutive patients with this group of lesions (21 of them with classic adamantinoma) in whom none of the OFD and OFD-like adamantinomas progressed to “classic” adamantinomas, with our patient, we preferred the diagnosis of OFD with rhabdoid elements.
“Rhabdoid” is the descriptive term for a morphologic appearance of cells that resemble rhabdomyoblasts, but, unlike the latter, do not express desmin. The expression of pan-cytokeratin in these cells, however, is noteworthy in the setting of OFD because it raises the question of a potential malignant lesion. Because the only difference between OFD and OFD-like adamantinoma is the readiness with which keratin-expressing epithelial cells can be detected (i.e., with immunohistochemistry or on routine hematoxylin and eosin-stained sections, respectively), it appears that the 2 forms represent a single pathologic process “exhibiting only a quantitative difference in their epithelial component.” The terms differentiated adamantinoma and OFD-like adamantinoma are used interchangeably with lesions in which few single or grouped pan-cytokeratin-positive cells are readily identifiable on routine stains.
Why OFD, especially when left untreated in young patients, has the potential to regress spontaneously remains unclear. We also do not have an answer as to why the lesions regressed in our patient after a small incisional biopsy. It could be conjectured that touching the lesion may have elicited an autoimmune response.
In summary, we believe that this case reinforces the importance of a careful clinical and pathologic evaluation for patients within the spectrum of OFD that ranges from OFD-like adamantinoma to classic adamantinoma.
Reference: Exner GU, von Hochstetter AR, Pfirrmann CWA. Osteofibrous dysplasia with rhabdoid elements in a 38-year-old man with spontaneous regression over five years: a case report. JBJS Case Connect. 2018 Jul-Sep;8(3):e51.

What is the diagnosis?
Fibrous dysplasia
Osteofibrous dysplasia with rhabdoid cells
Epithelioid osteoblastoma
Granulomatous inflammation suggestive of mycobacterial infection
Camurati-Engelmann disease (progressive diaphyseal dysplasia)