 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
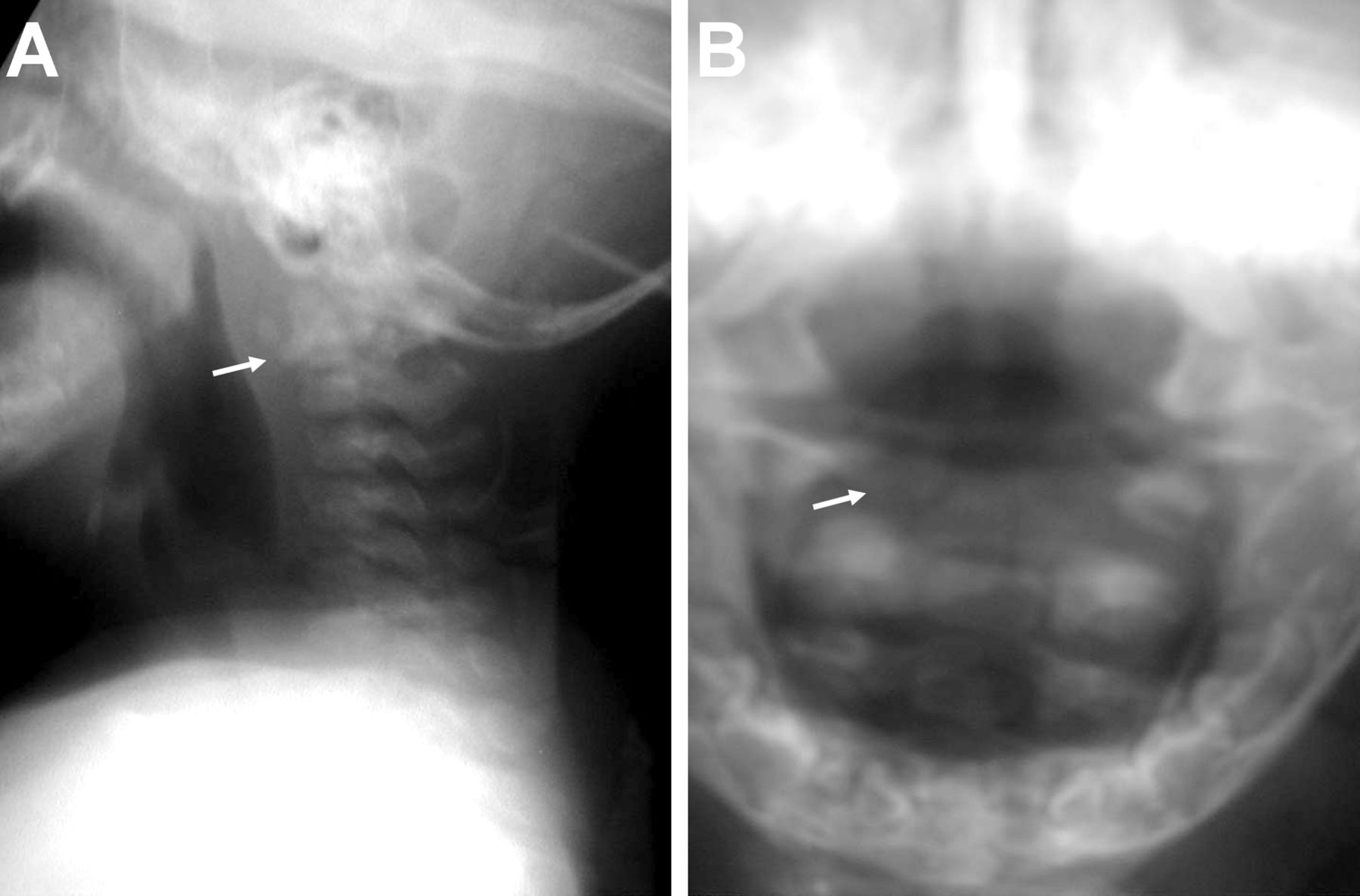
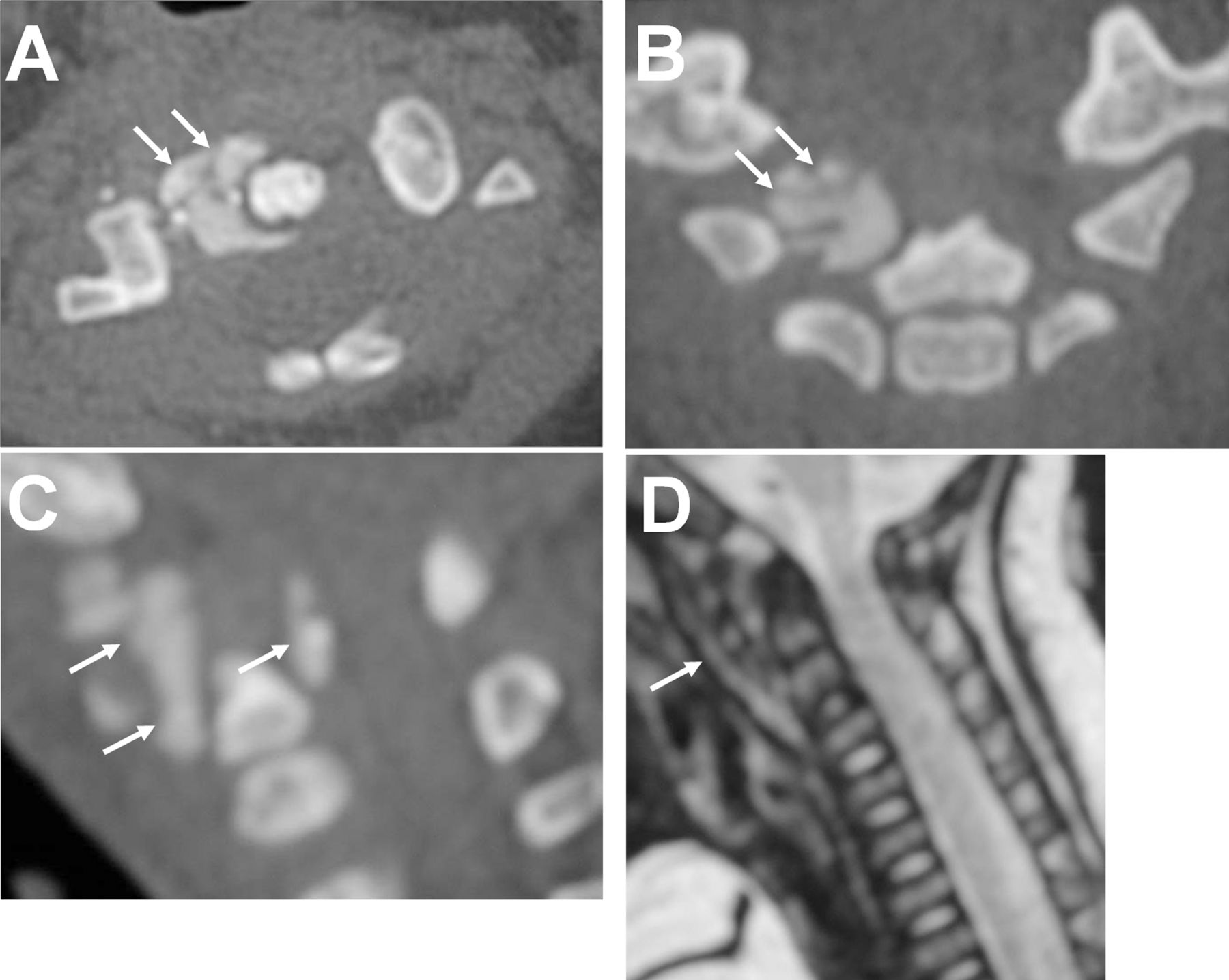
Fig. 3A previously healthy five-month-old girl was referred to our institution four days after the onset of acute, intense neck pain. The patient was unable to support her head, though she had begun to support it at the age of three months. One week prior to the onset of symptoms, she had fallen from a height of approximately 50 cm and hit her head with the neck extended. The patient did not have a fever upon presentation to us. Physical examination revealed a limited, painful neck motion in flexion, extension, and rotation. However, there was no evidence of neurological abnormality. There were no palpable masses or swelling around the neck, and there were no external signs of injury. No skeletal anomalies were observed. The results of laboratory tests, including complete blood-cell count, erythrocyte sedimentation rate, and C-reactive protein, were within normal ranges. There was no history of sore throat or upper respiratory infection before the trauma. There was no record of child abuse before the trauma or during the follow-up period. A lateral cervical spine radiograph demonstrated an abnormal calcified mass at the anterior aspects of the C1-C2 vertebrae (Fig. 1-A). Although the mass was poorly delineated on an open-mouth anteroposterior radiograph (Fig. 1-B), it was well defined by computed tomography (CT). Axial CT images confirmed the presence of a massive periodontoid calcification between the odontoid process and the right lateral aspect of C1 (Fig. 2-A). Coronal and sagittal CT images demonstrated that the calcification extended from the occipital region to C2 and from the anterior aspect of the odontoid to the retro-odontoid area (Figs. 2-B and 2-C). Magnetic resonance imaging (MRI) showed a mass around the odontoid process but no evidence of spinal cord compression (Fig. 2-D). There were no abnormal findings on the radiographs in the toes or other regions in the upper and lower extremities.
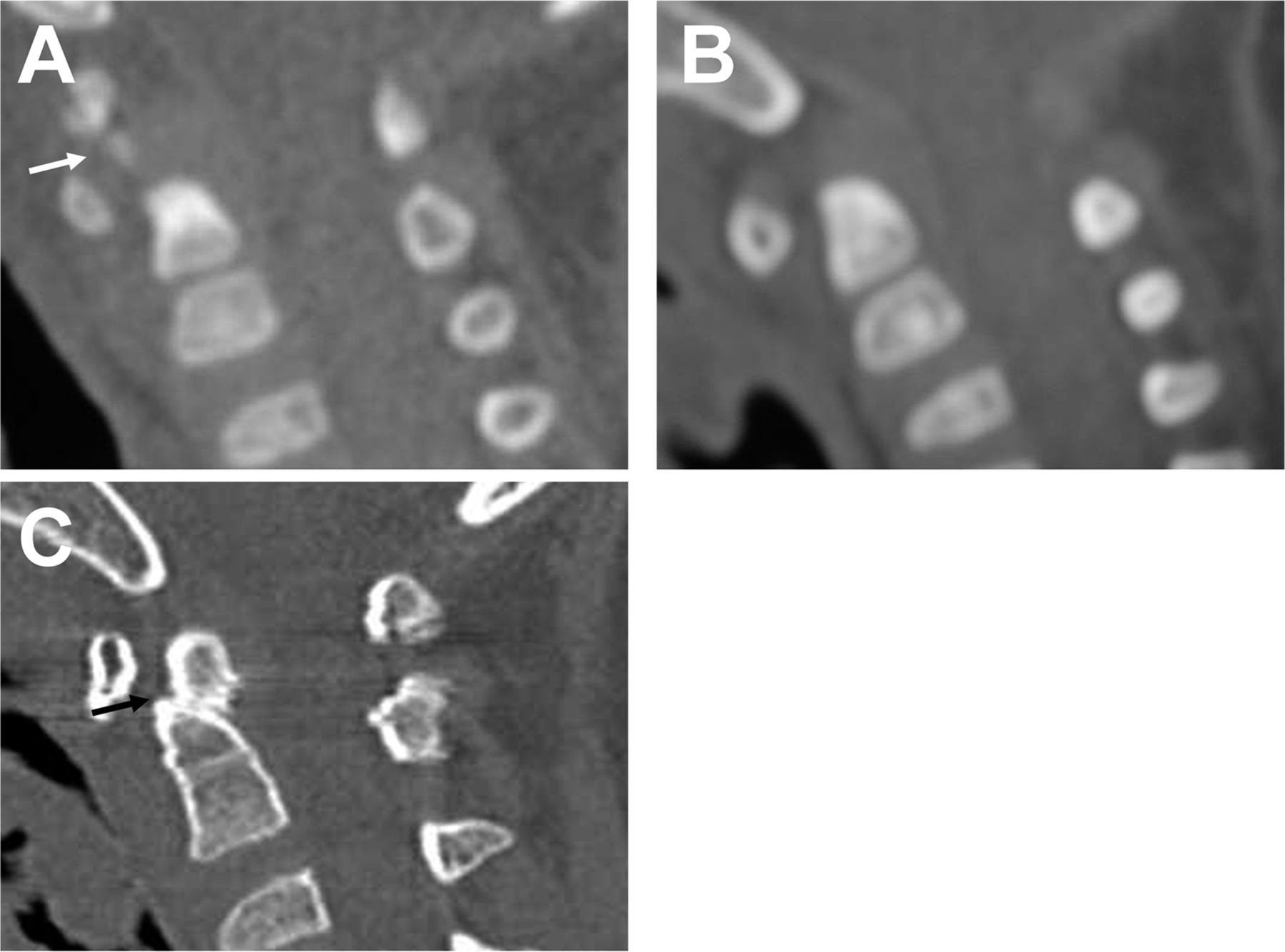
The patient was treated conservatively with use of a custom-made cervical orthosis prepared with fiberglass casting tapes and under-casting pads. The neck pain and restriction of neck movement appeared to resolve within two weeks of the onset of symptoms, and she regained the ability to support the neck. Because a CT scan revealed that the size of the calcified mass had decreased dramatically one month after the onset of symptoms (Fig. 3-A), we concluded that this was not a soft-tissue neoplasm. We diagnosed myositis ossificans traumatica (MOT), and the patient was discharged from the hospital. A CT scan performed three months after the onset of the symptoms indicated resorption of the calcification (Fig. 3-B). Although the patient did not experience any trauma after discharge, a CT scan was performed at the five-year follow-up to evaluate for potential growth problems in the upper cervical spine. In a CT image along the sagittal plane, deformity of the odontoid process was observed. Although an odontoid fracture had not been apparent on the initial radiographic examination, the CT scan five years later showed that the tip of the dens was displaced posteriorly and was malunited to the body of the odontoid process (Fig. 3-C), suggesting that a missed fracture of the odontoid possibly existed at the time of the initial trauma.
Proceed to Discussion >>Reference: Yoshii T, Nakai O, Hirai T, Sotome S, Shinomiya K, Okawa A. Myositis ossificans traumatica secondary to fracture of the odontoid in a five-month-old infant. A case report. JBJS Case Connect. 2012 Feb 22;2(1):e7.
The lesions of MOT are predominantly localized to the most common sites of injury in the thighs, hips, and elbows, but can occur at any other anatomical location in the body, including the spine. MOT is observed in adolescents and young adults but is rare in children. It has been reported that less than 1% of MOT cases occur in children under ten years of age. To our knowledge, there have been no reports in children under the age of one year. In patients with MOT, radiographs at the time of the initial event are often negative. Calcification of the osteoid tissue begins a few weeks later. The calcific-dense areas gradually enlarge, and the ossification pattern usually appears in six to eight weeks. The peripheral rim has increasing ossification in a zonal pattern. Complete maturation of the ossification usually takes five to six months; the lesion then regresses in size, and the ossified mass sometimes resolves spontaneously. MOT sometimes will present with atypical clinical and radiographic findings. In our case, the initial CT images did not indicate a typical zonal pattern: they showed a well-circumscribed, homogeneous mass with calcification. Because the radiographic findings can vary depending on the maturation of the mass, the zonal pattern may not be clear in some cases. Our patient followed a more rapid clinical course than is typical. Severe neck pain resolved within two weeks after the onset of symptoms. The calcified mass decreased in size as early as one month after the onset of symptoms and was resorbed at three months. Previously, Kim and Choi reported an atypical case in which the calcified mass was resorbed in a few months. The rapidity in the resolution can vary depending on the site or maturity of the calcified mass. Although the typical clinical course of MOT in an infant is still unknown, we speculate that it could be rapid because of the active potential for bone formation and resorption. Given the broad spectrum of presentation, the diagnosis of MOT in the cervical spine is sometimes difficult, especially in young children. Differential diagnosis should rule out other conditions, such as fibrodysplasia ossificans progressiva (FOP), infection, and soft-tissue neoplasms. FOP is an autosomal-dominant disorder that leads to heterotopic ossification in soft-tissue locations and progressively develops at multiple periarticular sites. In our case, FOP was ruled out because of the patient’s normal great toes and also by the radiographs taken from other sites in the body. Infection was eliminated because of the absence of fever and the negative results from the laboratory studies. In addition, we distinguished this case from neoplasms and FOP because of the history of trauma prior to the onset of symptoms and the evidence of spontaneous regression of the abnormal calcified mass. When the diagnosis of MOT is confirmed, patients are primarily managed with conservative treatment, such as immobilization of the neck to control hemorrhage and to avoid reinjuring the site. In our case, conservative treatment with use of a cervical orthosis was successful. The neck pain and restriction of neck movement resolved within two weeks with the decreasing size of the calcified mass, and the patient regained the ability to support the neck. Injuries of the upper cervical spine are uncommon in children; however, they may not be as rare as previously thought. It is reported that there is often a delay in diagnosis of a fracture of the dens in children, and some fractures remain undetected until complications develop at a later time. A fracture of the dens in young children usually involves disruption of the synchondrosis (the basal portion of the odontoid process) because of its mechanical weakness. However, in these children, a fracture can also involve the odontoid tip. In our case, a deformity of the odontoid tip was found at the five-year follow-up even though there were no additional injuries after the discharge. Although the initial radiograph did not clearly indicate an odontoid fracture, the tip of the dens was displaced posteriorly and was malunited to the body of the odontoid process. This finding suggested that an unrecognized fracture at the odontoid tip existed at the time of the initial trauma and that this injury caused the formation of a periodontoid calcification. Previous reports have demonstrated that an injury of the odontoid process during childhood can cause the development of os odontoideum. Whether the etiology of os odontoideum is congenital or posttraumatic has been a subject of debate. In the posttraumatic theory, traumatic injuries of the odontoid process, such as an unrecognized fracture, a dislocation of the odontoid tip, a ligamentous injury, or a cartilaginous injury, can lead to the formation of os odontoideum. In our case, an unrecognized fracture of the odontoid process could have caused the development of a deformity in the odontoid process. The odontoid tip was united to the body of the odontoid process in this patient. However, this type of injury could result in the development of os odontoideum. In summary, we present an unusual case of a five-month-old infant who developed a massive calcification around the odontoid process following minor trauma. When a calcification of soft tissue is found in young children, the differential diagnosis should include myositis ossificans as well as neoplasm. In addition, the existence of other underlying injuries associated with the calcification, which can cause problems with vertebral development, should always be considered.
Reference: Yoshii T, Nakai O, Hirai T, Sotome S, Shinomiya K, Okawa A. Myositis ossificans traumatica secondary to fracture of the odontoid in a five-month-old infant. A case report. JBJS Case Connect. 2012 Feb 22;2(1):e7.
Tumoral calcinosis
Myositis ossificans traumatica
Plasmacytoma of C2
Aneurysmal bone cyst at C2
Retropharyngeal lymphoma