A 48-Year-Old Woman with Increasing Thigh Pain Following a Fall
January 16, 2019
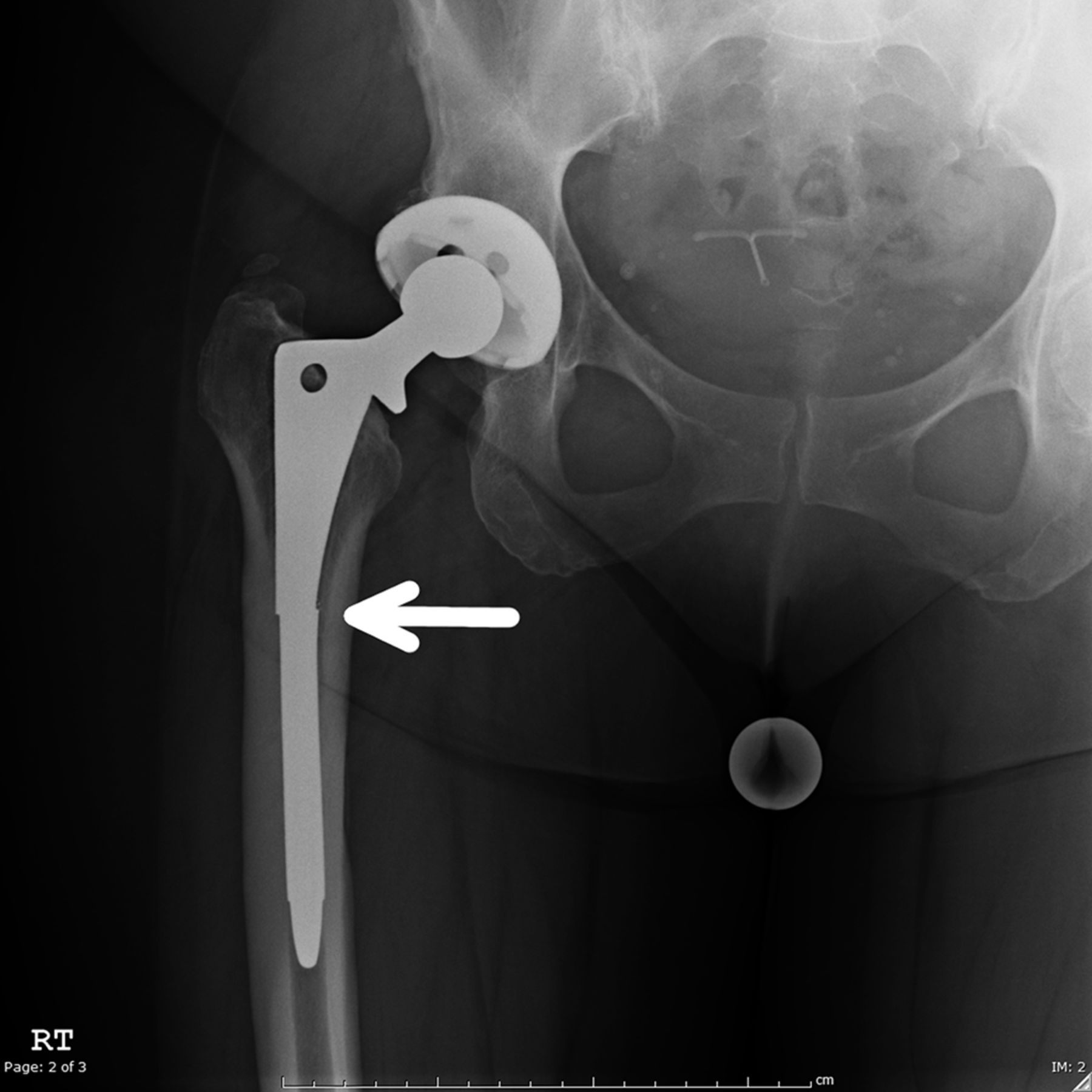


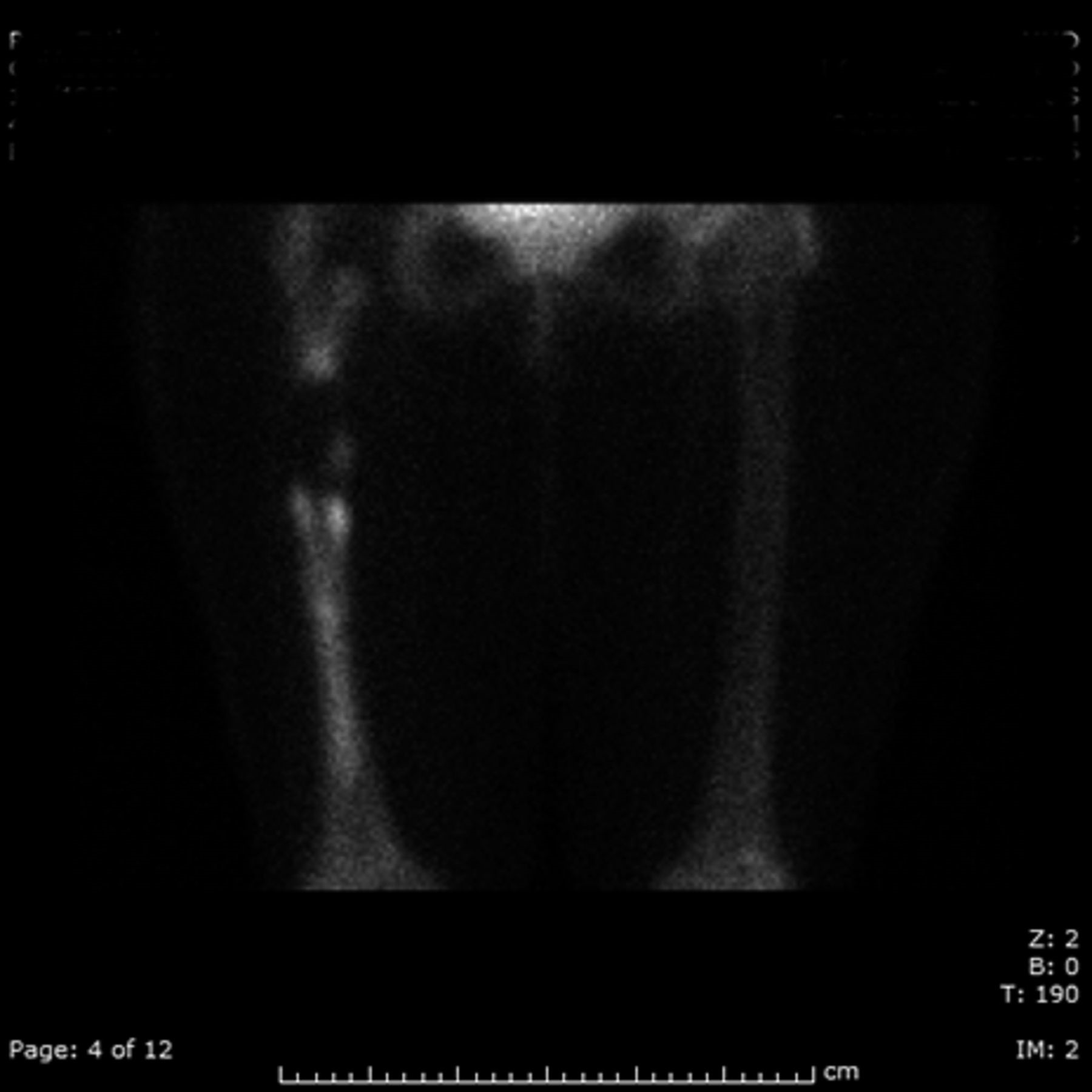


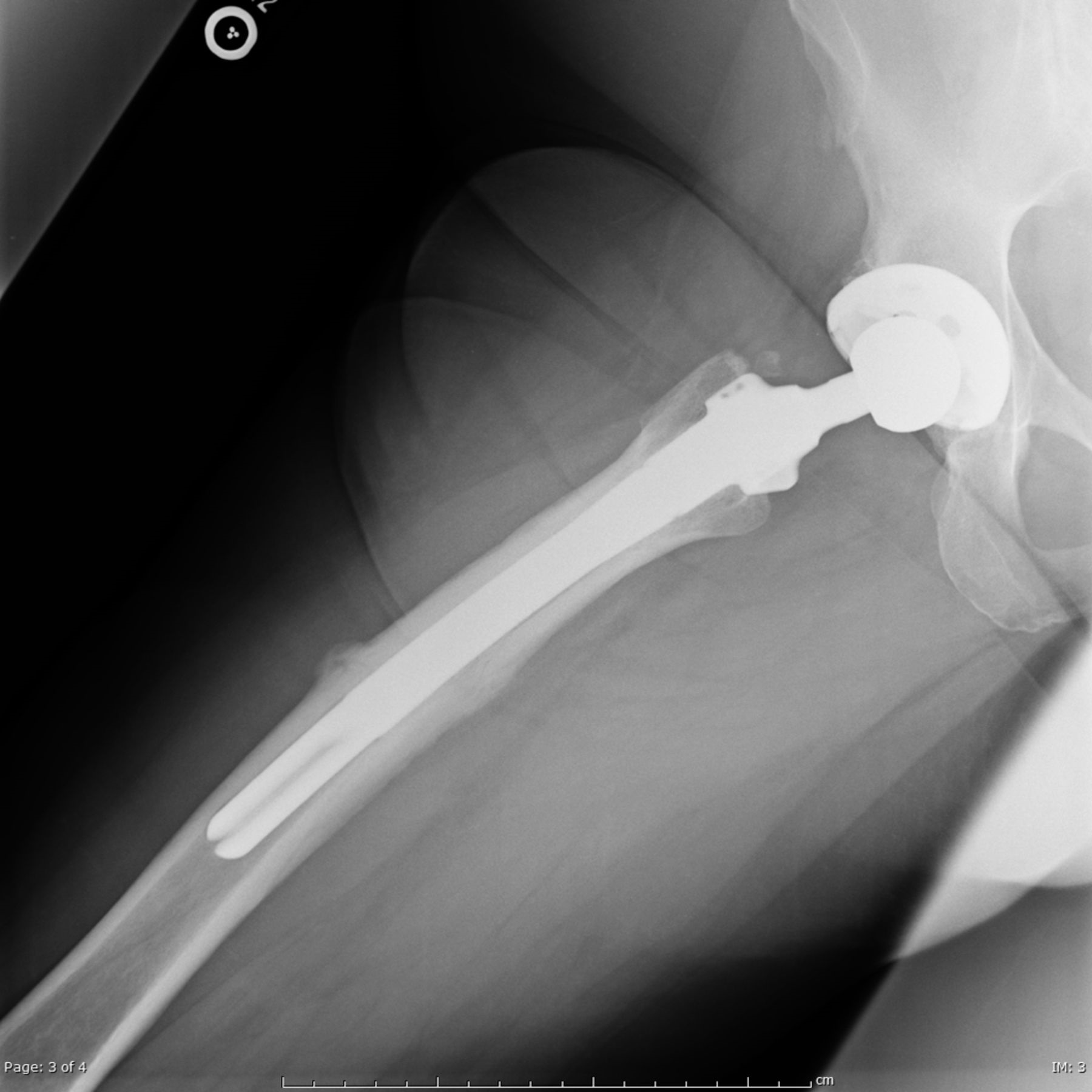
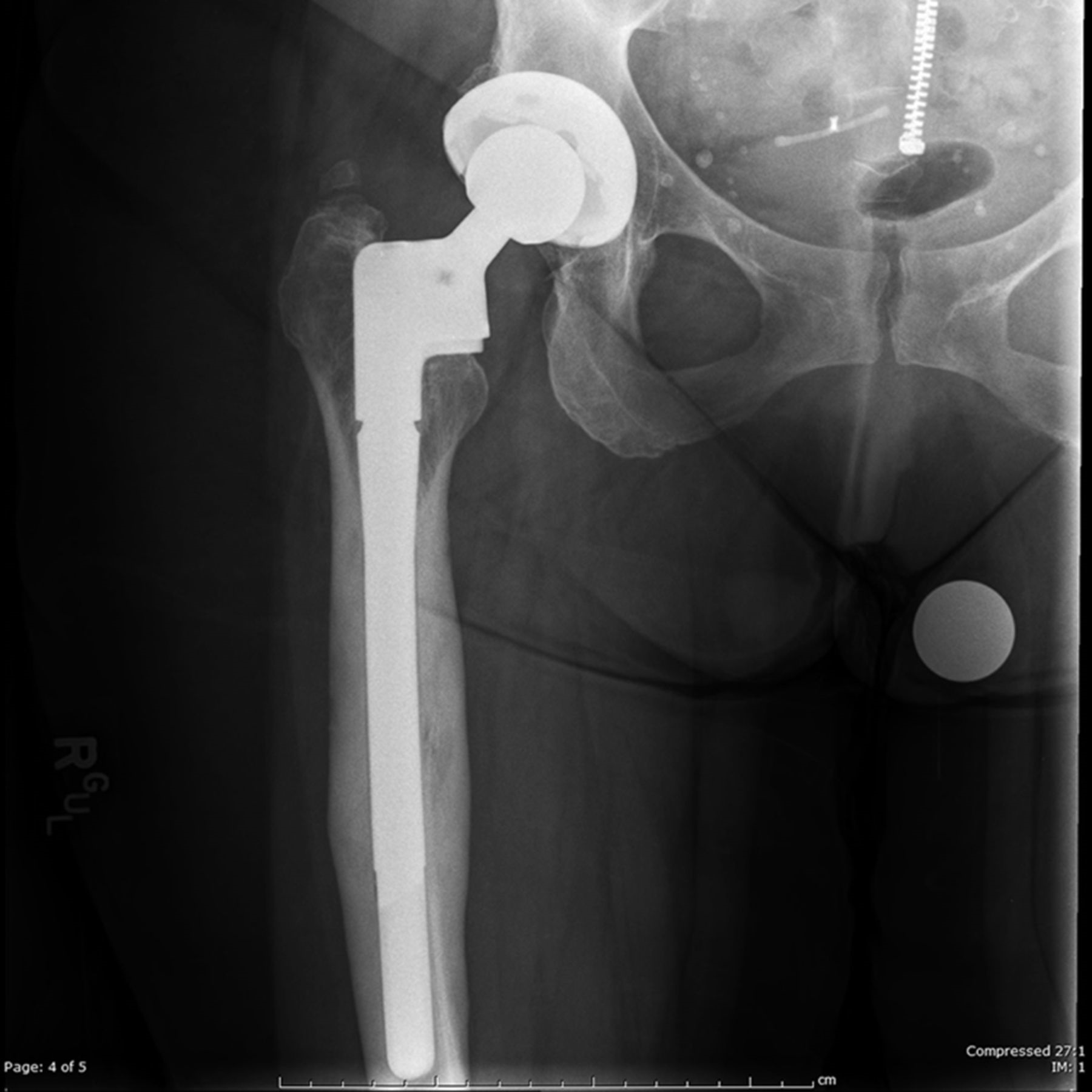

 Fig. 1
Fig. 1 Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 4-A
Fig. 4-A Fig. 4-B
Fig. 4-B Fig. 5-A
Fig. 5-A Fig. 5-B
Fig. 5-BA forty-eight-year-old woman with a body mass index of 36 kg/m2 underwent a primary total hip arthroplasty with a 10.5-mm fully porous-coated femoral component (AML; DePuy) for degenerative joint disease secondary to a prior slipped capital femoral epiphysis. She initially did well, but presented five years postoperatively with thigh pain. The pain worsened after she stepped off a curb at six years postoperatively, and she required crutches with ambulation. A radiograph showed a fracture of the femoral component (Fig. 1). Revision of the fractured femoral component was recommended.
At the time of revision, a polyethylene liner exchange of the acetabular component was performed, and the metaphyseal portion of the stem that was loose was removed. The diaphyseal portion of the stem was well fixed. The proximal part of the diaphysis was reamed with a straight reamer above the retained distal segment to 12 mm (1.5 mm larger than the implanted stem). Next, since access was felt to be acceptable, trephines were used to remove the distal portion of the stem without performing an extended trochanteric osteotomy. Three trephines were utilized in conjunction with copious irrigation. The femoral canal was then prepared to accept the revision femoral component. Intraoperative radiographs showed an acceptable position of the revision implant without evidence of perforation or fracture.
Postoperatively, weight-bearing was limited to 30 lb (13.6 kg) for the first six weeks. Radiographs at that time showed an acceptable position of the revision component (Figs. 2-A and 2-B). The patient initially did well; however, at four months postoperatively, the pain in the thigh had worsened over time, requiring the use of a crutch with ambulation. Radiographs showed no interval change, and an evaluation for infection was negative.
At one year postoperatively, a technetium-99m bone scan showed a 4 to 5-cm area of decreased uptake at the junction of the middle and distal thirds of the femoral shaft (Figs. 3-A and 3-B). The patient was instructed to use two crutches with ambulation; two months later, the pain had improved. Radiographs showed changes in the cortex (Figs. 4-A and 4-B). At six years postoperatively, she had no pain, and the implants were stable (Figs. 5-A and 5-B).
Radiographic changes at 1 year after revision were interpreted as showing diaphyseal osteonecrosis, likely caused by heat from the reaming that was required to remove the broken femoral component. Subsequent changes suggested a stress fracture, followed by healing with a hypertrophic callus.
Proceed to Discussion >>Reference: Conrad DN, Dennis DA. Trephine use during revision total hip arthroplasty resulting in diaphyseal osteonecrosis and stress fracture: a case report. JBJS Case Connect. 2015 Apr 8;5(2):e31.
We report a case of thermal osteonecrosis and stress fracture of the femoral diaphysis associated with use of trephines to remove a broken fully porous-coated femoral component. In a review of the literature, we found that Austin et al. reported an intraoperative femoral fracture secondary to trephine reamer breakage at the distal end. The physiologic effects of intramedullary reaming, including the thermal induction of osteonecrosis, have been well established. Numerous cases of segmental thermal osteonecrosis have been reported in the orthopaedic trauma literature. Many of these cases involve small intramedullary canals where the reamer was intimately in contact with the endosteal cortical bone, causing heat generation. Notably, irrigation and aspiration of room temperature normal saline solution while reaming the intramedullary canal have been shown to drastically decrease the peak cortical temperatures. Additionally, the condition of the reamers can dramatically affect the peak cortical temperature; higher temperatures are seen with dull reamers.
Kancherla et al. reviewed thirty-six cases of revision total hip arthroplasty in which trephines were used for removal of a broken femoral stem. They observed two cases of periprosthetic fracture that occurred at a similar time interval as with our patient (postoperatively at three and four months, respectively). Thermal necrosis was suspected in both of these cases.
With our patient, copious irrigation was utilized during the trephining process to cool the reamers. Additionally, three different trephine reamers were utilized to avoid the use of a dull reamer. Despite these measures, the femoral segment adjacent to the trephining process became osteonecrotic and subsequently lost its mechanical integrity. The revision femoral stem used for the reconstruction gained diaphyseal fixation distal to the site of the thermal osteonecrosis, imparting stability to the surrounding compromised bone and stress fracture. Once the osteonecrosis had been identified, the patient was successfully treated nonoperatively with limited weight-bearing, ambulatory aids, activity modification, and close clinical follow-up. Diagnosis had been delayed, primarily because the effects of thermal osteonecrosis were not initially evident. Earlier diagnosis may be possible if a high index of suspicion is present in cases in which trephines have been used and persistent thigh pain exists.
In retrospect, the patient’s obesity and relatively small primary femoral component diameter likely contributed to the femoral component fracture. Additionally, the narrow intramedullary canal and femoral bow may have led to excessive thinning of the medial cortex, further disposing this area to thermal osteonecrosis and subsequent stress fracture. If an extended trochanteric osteotomy had been performed, trephine reaming may have been more central, and less heat would have been produced; an extended trochanteric osteotomy should have been considered to lessen heat generation during the trephining process. With these types of cases, it is imperative to anticipate the problems that can arise with the use of such a valuable and powerful instrument. Copious irrigation and employing numerous reamers may decrease the peak cortical temperature; however, avoidance of thermal osteonecrosis and stress fracture is not ensured. Based on this experience, we typically now exhibit more patience during the trephining procedure and avoid extended seconds of continuous reaming in hopes of generating less thermal injury.
Reference: Conrad DN, Dennis DA. Trephine use during revision total hip arthroplasty resulting in diaphyseal osteonecrosis and stress fracture: a case report. JBJS Case Connect. 2015 Apr 8;5(2):e31.
What is the diagnosis?
New-onset Paget disease
Melorheostosis
Thermal-induced osteonecrosis, stress fracture, and fracture callus
Osteopathia striata (Voorhoeve disease)
Erdheim-Chester disease