A 14-Year-Old-Girl with Wrist Pain and Swelling
September 21, 2016
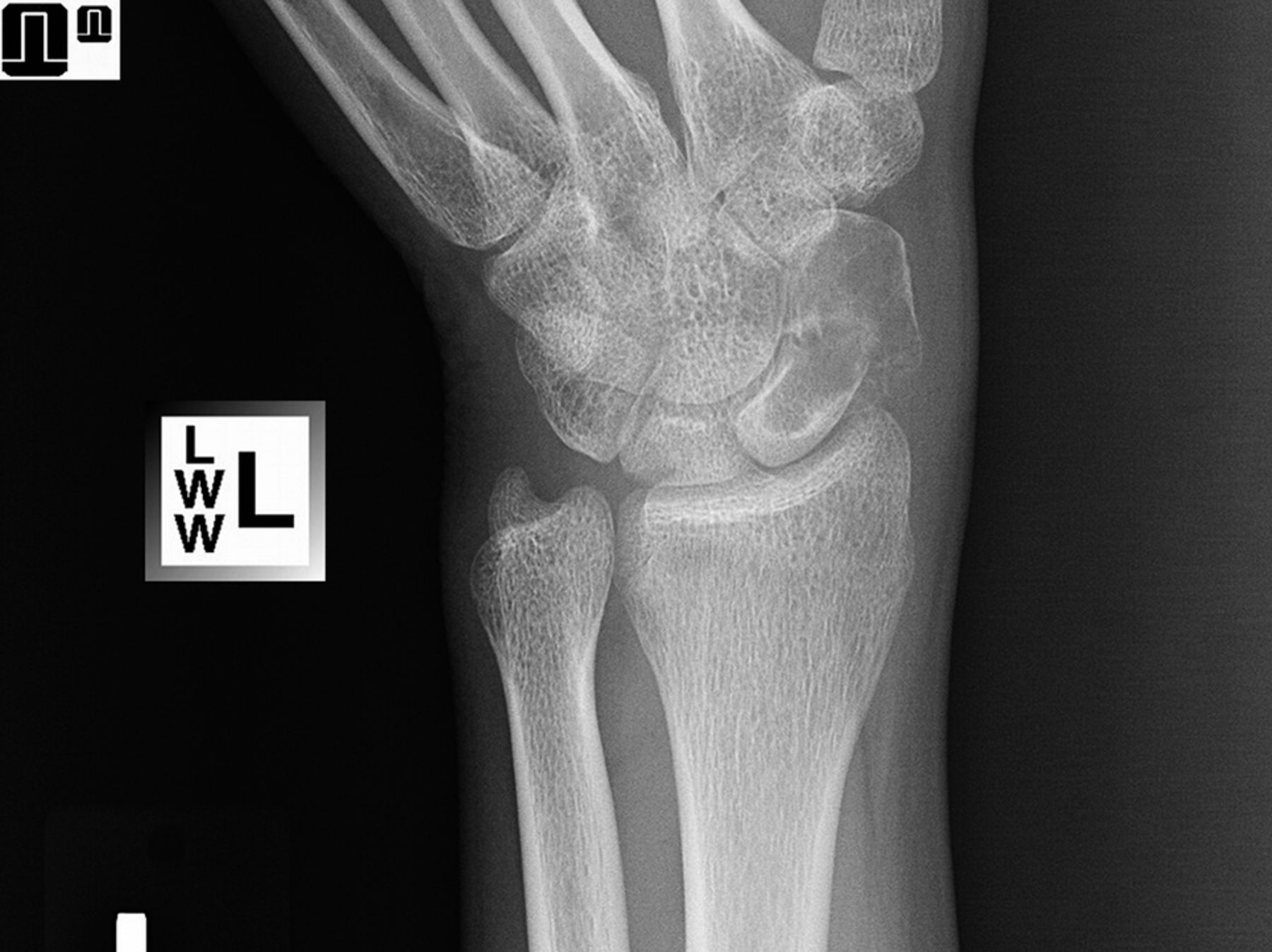
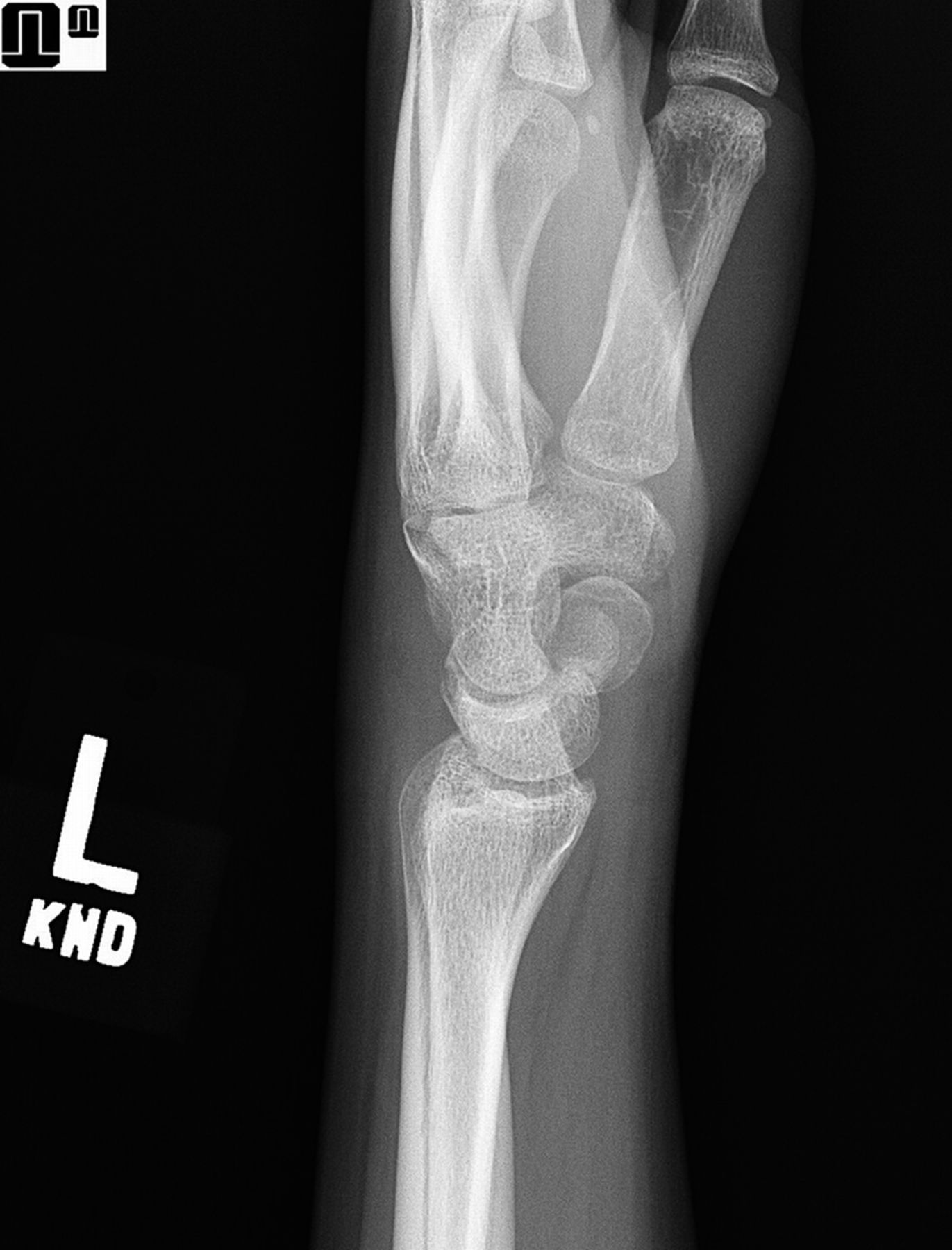
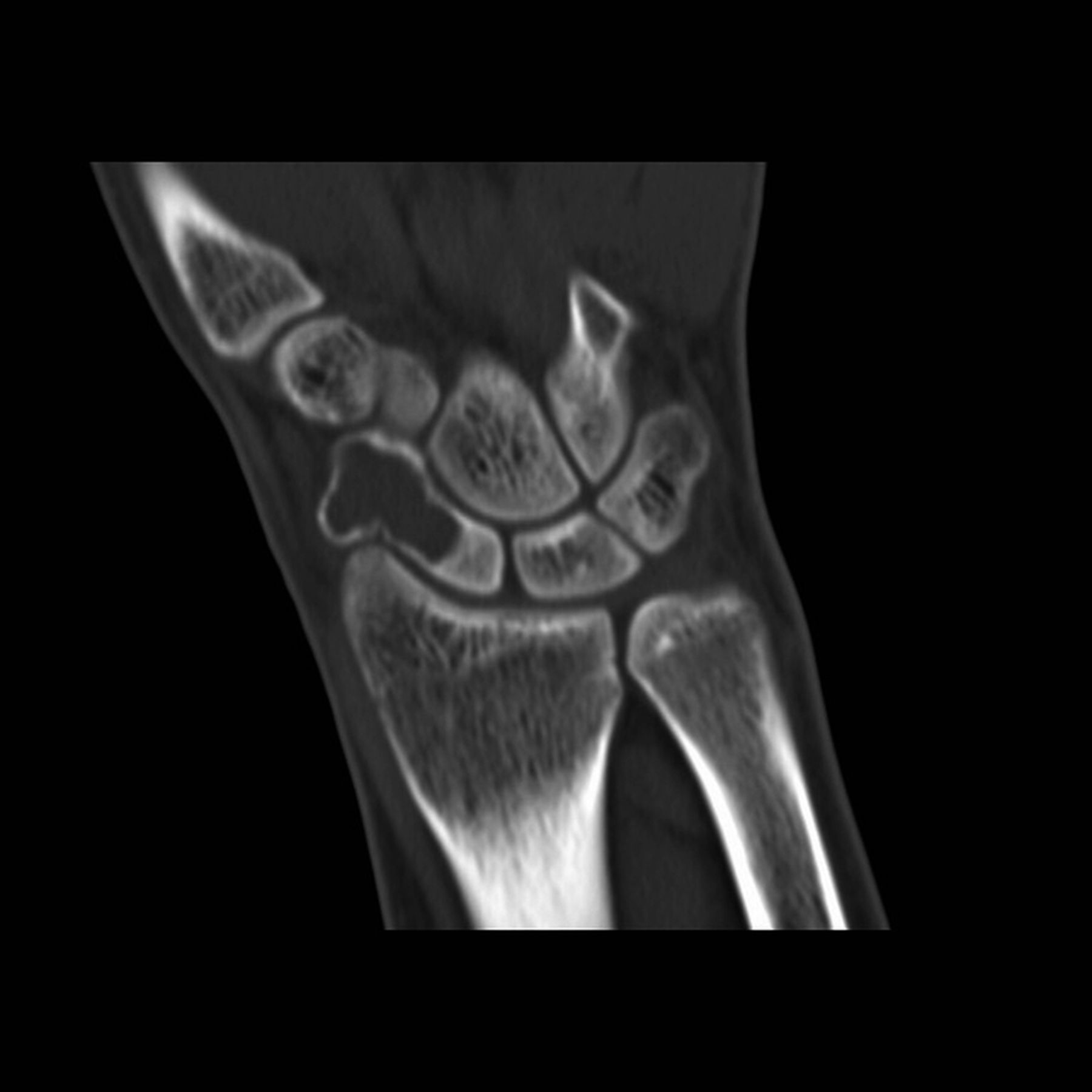

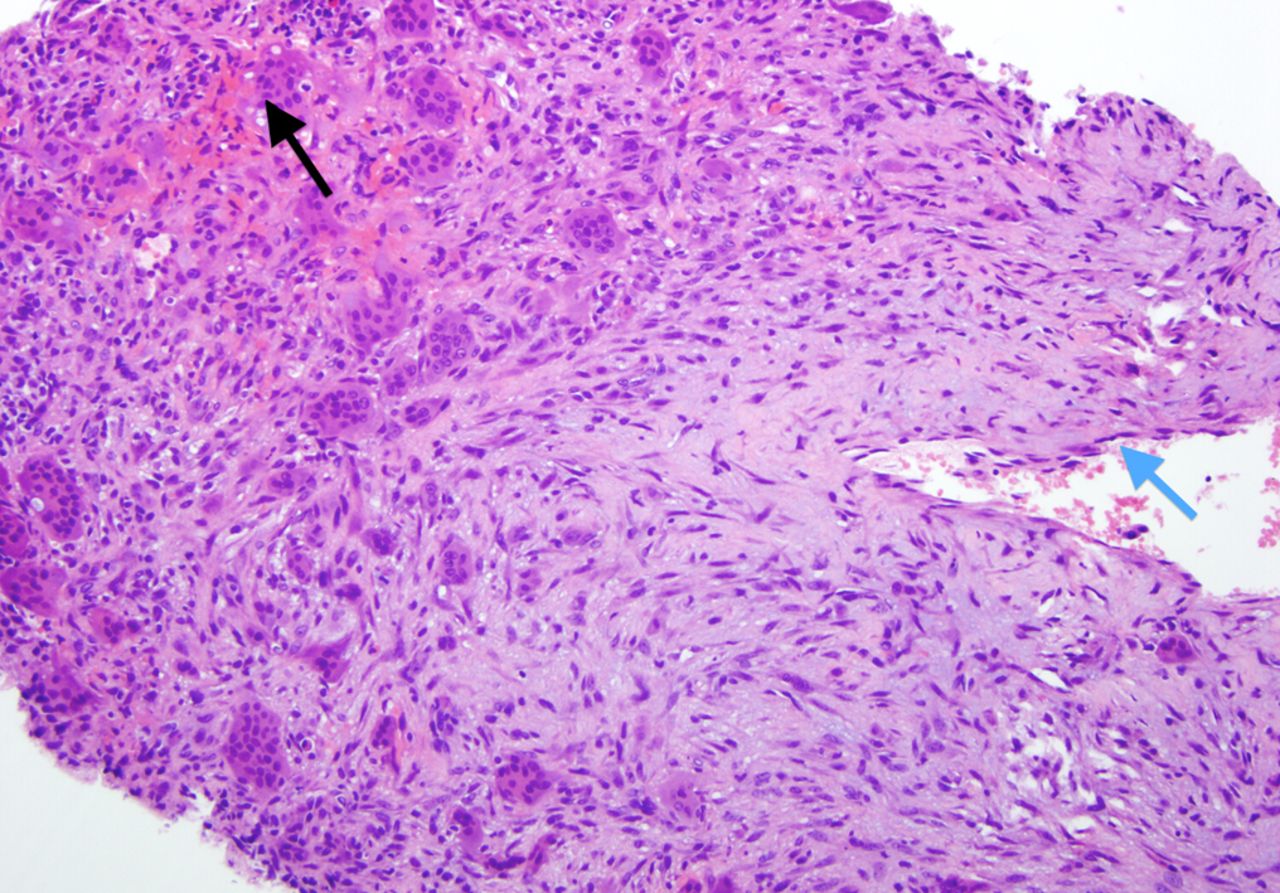
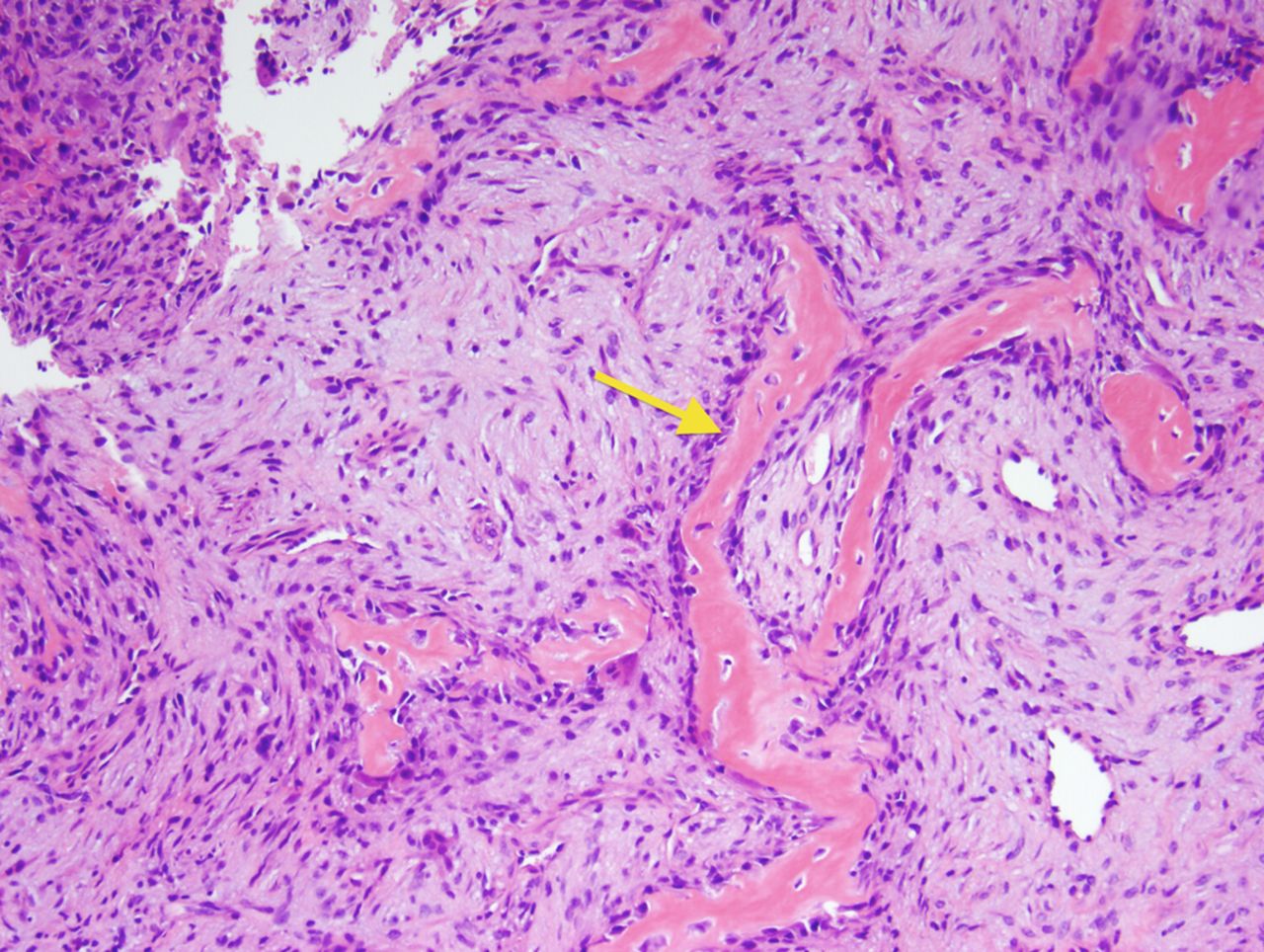
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 6
Fig. 6 Fig. 7
Fig. 7 Fig. 8
Fig. 8 Fig. 9
Fig. 9A 14-year-old, otherwise healthy girl was referred for left wrist pain and swelling, which she had had for more than 1 year without a history of trauma. Her symptoms began gradually and intermittently but progressed to a constant ache. She had pain and swelling over the dorsal and radial aspects of the wrist, which were exacerbated by motion. The examination was notable for swelling and mild tenderness over the dorsal-radial aspect of the left wrist in proximity to the anatomic snuffbox. Range of motion of the left wrist was limited compared with the contralateral wrist.
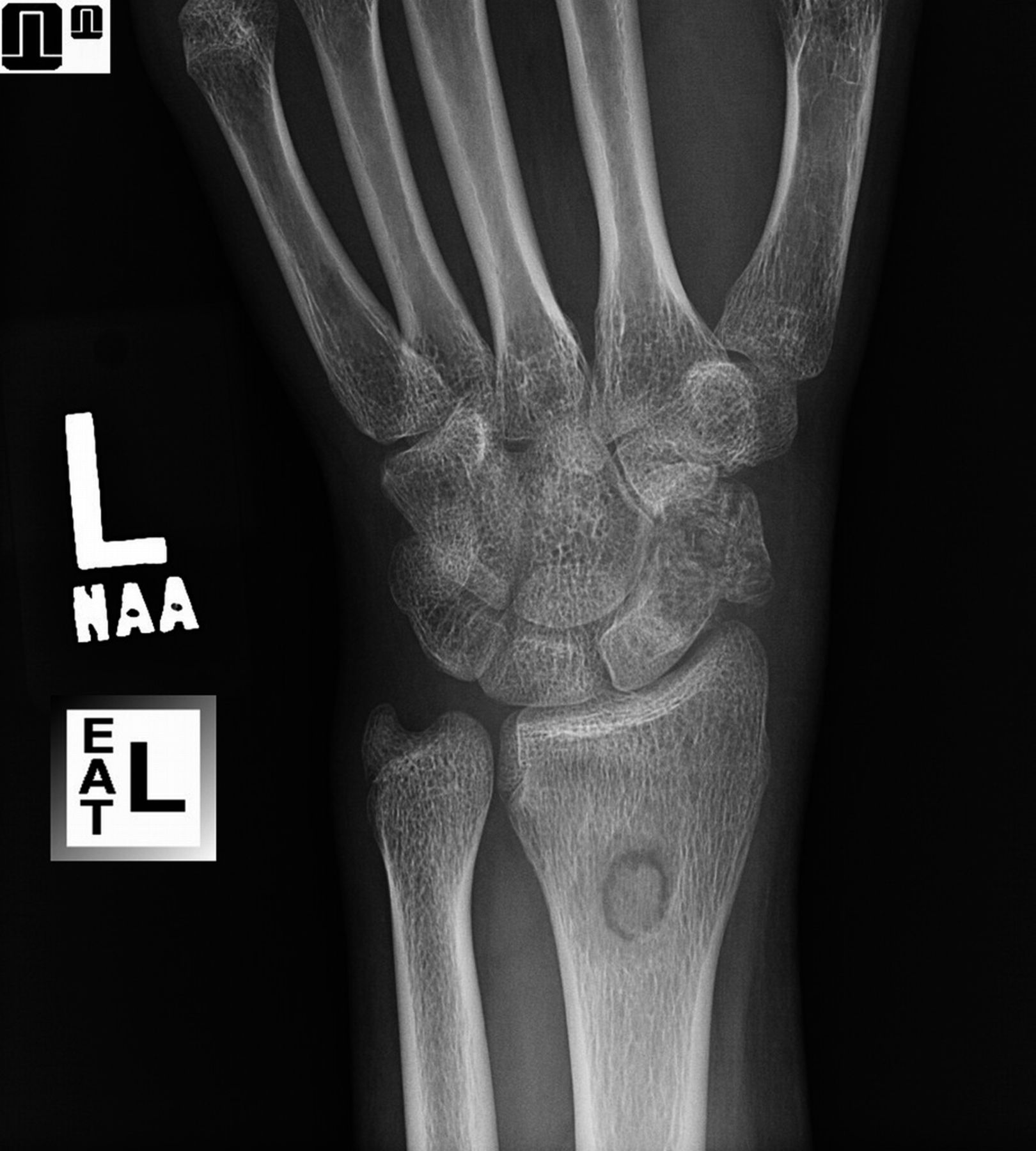
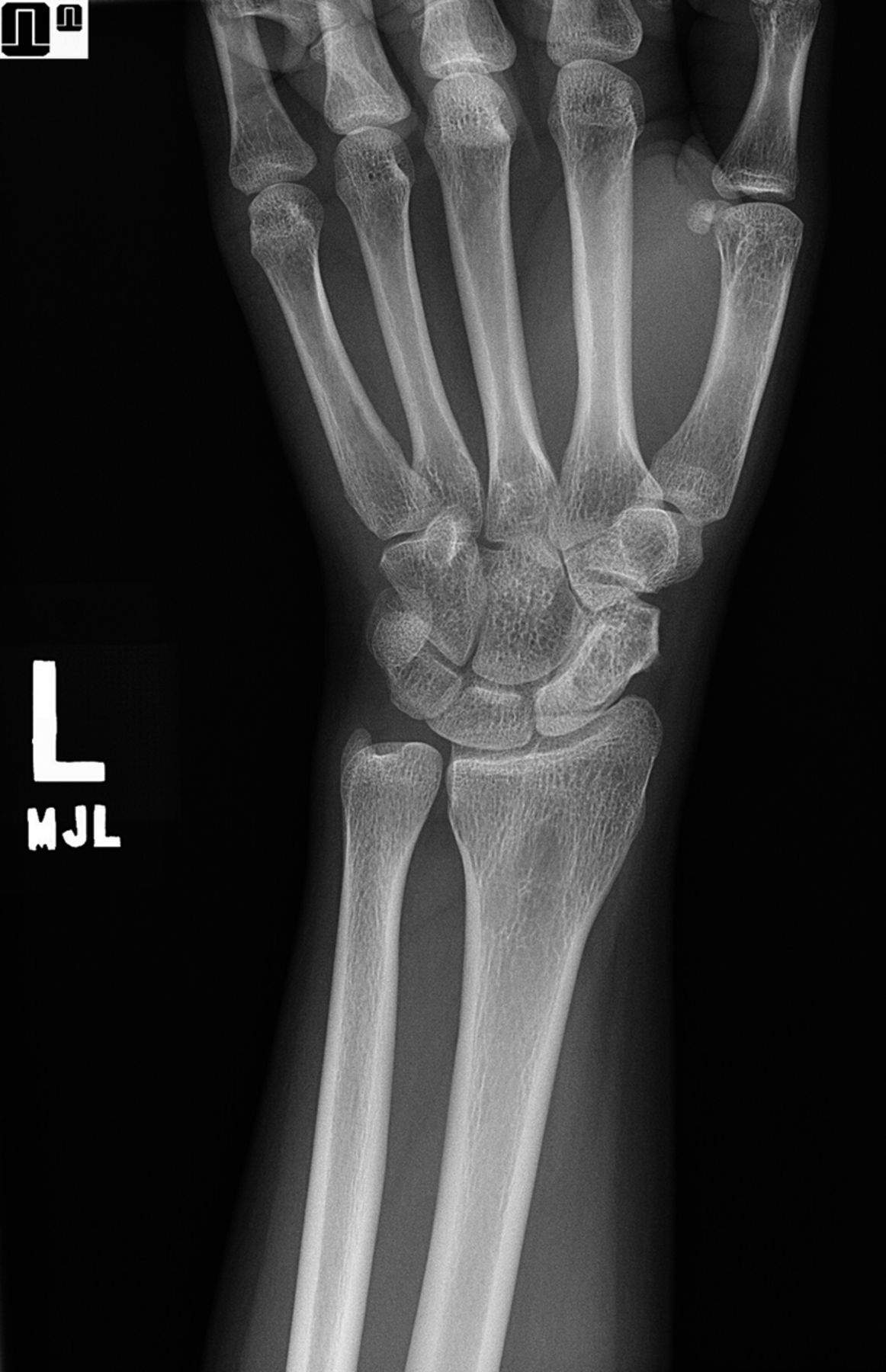
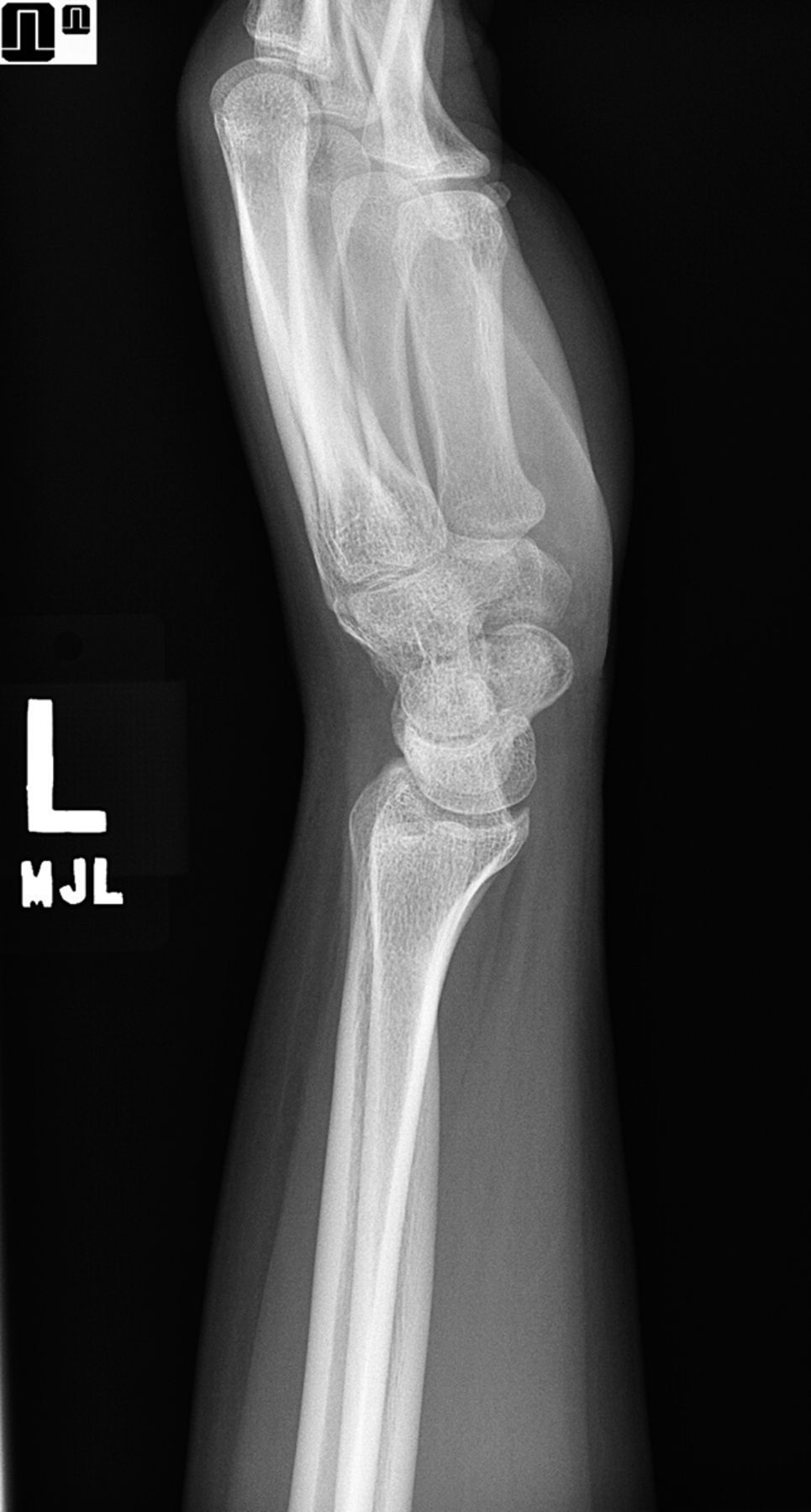
Radiographs demonstrated a lesion encompassing nearly the entirety of the middle and distal aspects of the scaphoid with an associated pathologic fracture (Figs. 1 and 2). Computed tomography (CT) also demonstrated the minimally displaced pathologic fracture as well as substantial cortical thinning surrounding the lytic lesion (Fig. 3). Magnetic resonance imaging (MRI) showed an expansile lesion with septal and rim enhancement on post-contrast sequences (Fig. 4).
In part because of the unusual location, the decision was made to conduct an open biopsy of the lesion to establish a histologic diagnosis prior to definitive treatment. Under regional anesthesia, the lesion was biopsied from a dorsal approach using the 3,4 interval between the extensor pollicis longus and extensor digitorum communis. A small cortical window was created in the dorsal aspect of the scaphoid. Representative photomicrographs are displayed in Figures 5 and 6.
The biopsy contained predominantly fibrous tissue with admixed multinucleated osteoclast-like giant cells often centered on areas of stromal hemorrhage. Foci consistent with the cyst walls that line blood-filled cavities were also noted. A small amount of reactive woven bone was also present. These findings confirm the diagnosis of aneurysmal bone cyst (ABC). Following diagnosis, the patient underwent a second surgical procedure under regional anesthesia for definitive treatment with curettage, phenol adjuvant therapy, and distal radial autografting as well as allografting with demineralized bone matrix and cancellous chips (Fig. 7). The postoperative course required prolonged immobilization followed by ultrasound-mediated bone stimulation; however, 23 months following surgery, the left scaphoid demonstrated radiographic union and she had no pain and minimal limitation of range of motion clinically (Figs. 8 and 9).
Proceed to Discussion >>Reference: Lebus GF, Cates JM, Lee DH. Aneurysmal bone cyst of the scaphoid: A case report. JBJS Case Connect. 2016 Jun 22;6(2):e49.
First described by Jaffe and Lichtenstein in 1942, ABCs are rare, benign skeletal tumors that affect patients early in life, usually in the first 2 decades. Although they may arise in any portion of the skeleton, the majority affect the femur, tibia, humerus, fibula, skull, and posterior elements of the spine. Most patients with ABC present with localized pain and soft-tissue swelling and occasionally a palpable, expansile mass. The classic appearance on radiographs is that of an expansile lesion with thinned cortices and often osseous septations. MRI reveals contrast-enhancing septa as well as fluid-fluid levels, which represent the layering of solid blood components within the cavity of the lesion. The pathophysiology of ABCs remains controversial. Some cases may represent a primary bone neoplasm, while others may be sequelae of traumatic injury; a vascular anomaly; or cystic degeneration of a precursor lesion, such as giant cell tumor of bone, osteoblastoma, osteosarcoma, chondroblastoma, nonossifying fibroma, or fibrous dysplasia, among other bone tumors. Although ABCs have a signature appearance radiographically and histologically, other lesions can have many of these characteristics as well. Fracture through a simple cyst, giant cell tumor, and telangiectatic osteosarcoma should remain in the differential diagnosis when assessing these lesions. In the case of our patient, the histopathologic diagnosis was made by virtue of the facts that the stroma is more fibrous in an aneurysmal bone cyst than in a giant cell tumor and that aneurysmal bone cysts lack the overt cytologic atypia and atypical mitotic activity seen in osteosarcoma.
The ideal treatment for aneurysmal bone cysts is also a matter of controversy because of a lack of prospective randomized controlled trials; however, the most common method consists of curettage with or without adjuvant therapy and bone-grafting. Excision has the lowest rate of recurrence but is often not practical given the anatomic location of the lesion. For lesions that are extensive and periarticular, resection and reconstruction or arthrodesis may be required. Treatment is not always straightforward, as the rate of local recurrence has been reported to be as high as 20% and malignant transformation, although rare, has been documented. Phenol adjuvant therapy, which was used in this case, has historically been believed to lead to decreased recurrence rates because of its necrotizing effect on residual tumor cells, although recent reports suggest that adequate intralesional curettage may be more predictive of decreased recurrence rates than use of any adjuvant therapy. Additionally, phenol and other adjuvant treatments may damage surrounding normal tissues and should be employed with discretion.
There are few reports documenting the existence of ABCs in the carpal bones, particularly the scaphoid. To our knowledge, there is only one prior study, in the French literature, of a similar occurrence in the scaphoid bone specifically. Platt and Klugman described a similar account of an ABC of the capitate in 1995 as well as documented a review of 32 previously reported cases of ABC of the hand. In that study, the majority (52%) of ABCs involved the metacarpals, followed by the phalanges (36%) and then the carpal bones (12%). Mankin et al. and Moussallem et al. documented 2 separate cases of ABC of the lunate. Whereas Mankin et al. performed an excision of the lunate and a scaphocapitate arthrodesis, Moussallem et al. treated their case by curettage and bone-grafting without excision or arthrodesis. Both methods achieved good clinical outcomes. Sakamoto et al. similarly successfully treated an ABC of the capitate without arthrodesis and obtained a good clinical outcome without recurrence.
In summary, this case report documents an uncommon but treatable cause of wrist pain in an otherwise healthy adolescent. Similar to other cases in the literature, our patient experienced resolution of the ABC of the scaphoid with curettage, phenol adjuvant therapy, and local autografting along with supplemental allograft. She did have a prolonged postoperative course in terms of osseous healing of the scaphoid, but nearly 2 years after treatment, she had no sign of recurrence and was clinically asymptomatic.
Reference: Lebus GF, Cates JM, Lee DH. Aneurysmal bone cyst of the scaphoid: A case report. JBJS Case Connect. 2016 Jun 22;6(2):e49.
What is the diagnosis?
Tenosynovial giant cell tumor (giant cell tumor of tendon sheath)
Intraosseous ganglion cyst
Giant cell tumor of the bone
Brown tumor of hyperparathyroidism
Aneurysmal bone cyst