An 18-Year-Old Woman with an Enlarging Mass on the Hand
October 18, 2017


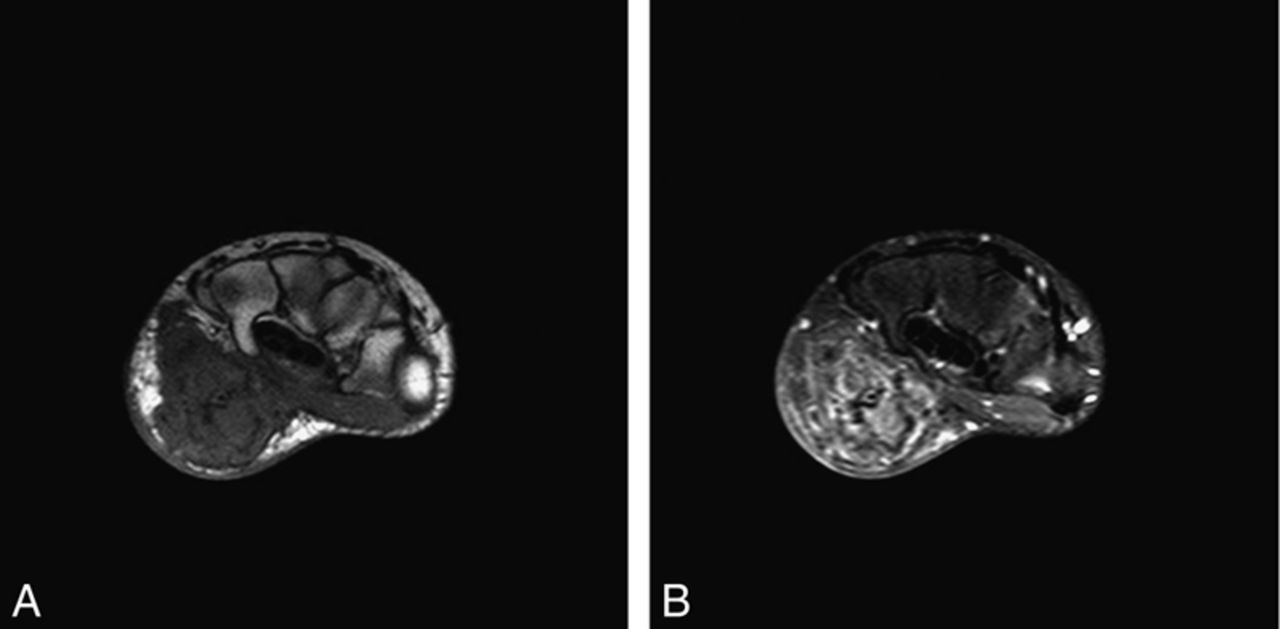
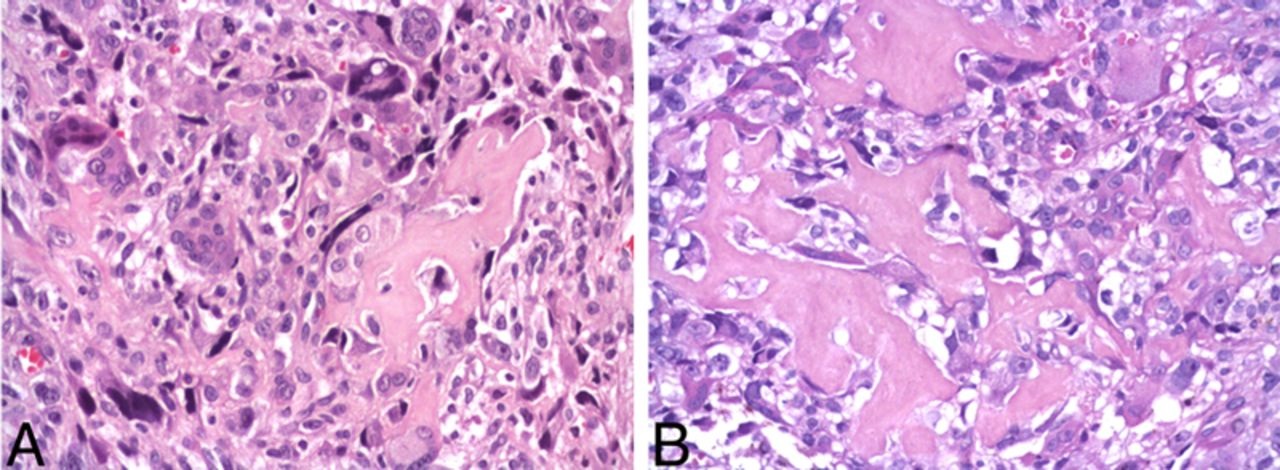
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 6
Fig. 6 Fig. 7
Fig. 7An eighteen-year-old woman presented with a rapidly enlarging, painless mass of the left hand. The patient had noticed the mass four months earlier. She reported no injury to the hand or prior history of radiation therapy. She denied any health problems and family history of cancer. No skeletal involvement was seen.
Physical examination confirmed a firm, immobile, painless mass, approximately 3.5 × 2.5 × 1.5 cm in size, situated superficially in the hypothenar region of the left hand (Fig. 1).
Radiographs of the hand demonstrated a soft-tissue mass with an irregular ossified matrix contained within the hypothenar eminence. The mass did not appear to be attached to the underlying skeleton, although it seemed to distort the carpal bone relationship (Fig. 2).
Magnetic resonance imaging showed a large soft-tissue mass with heterogeneous signal intensity within the hypothenar muscles (Figs. 3-A and 3-B).
A biopsy was obtained and showed histologic features similar to those seen in Figure 4.
The biopsy was interpreted as a high-grade extraskeletal osteosarcoma (ESOS).
After completing two cycles of neoadjuvant chemotherapy with doxorubicin and ifosfamide, the patient underwent wide local excision of the primary tumor via partial amputation of the hand.
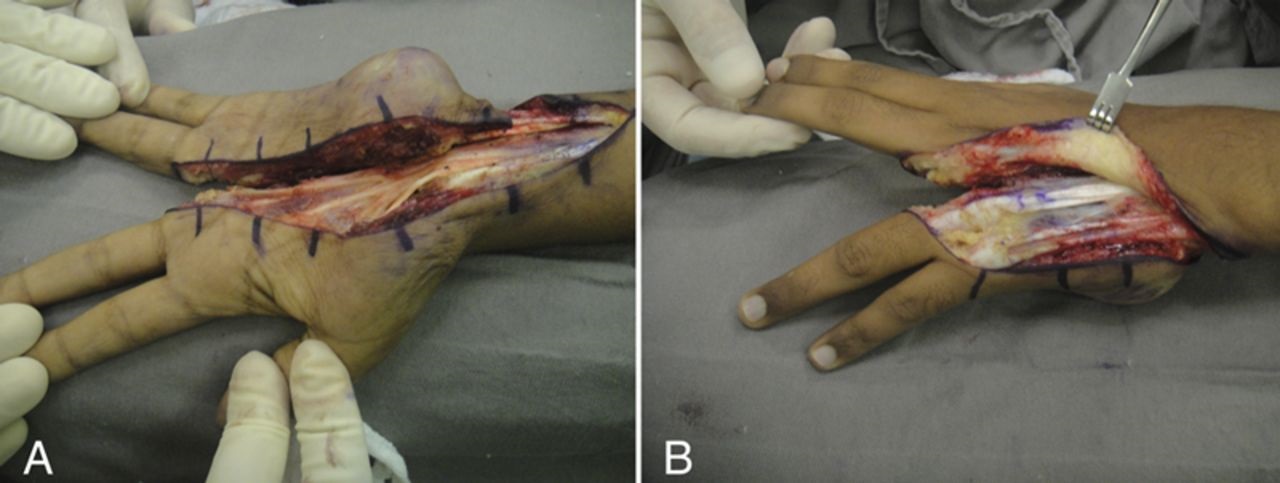
The fourth and fifth distal rays were resected along with the hamate, pisiform, and triquetrum bones, as well as the ulnar head and surrounding soft tissue (Fig. 5). The carpal tunnel was not compromised, and its radial structures, including the median nerve, were preserved.
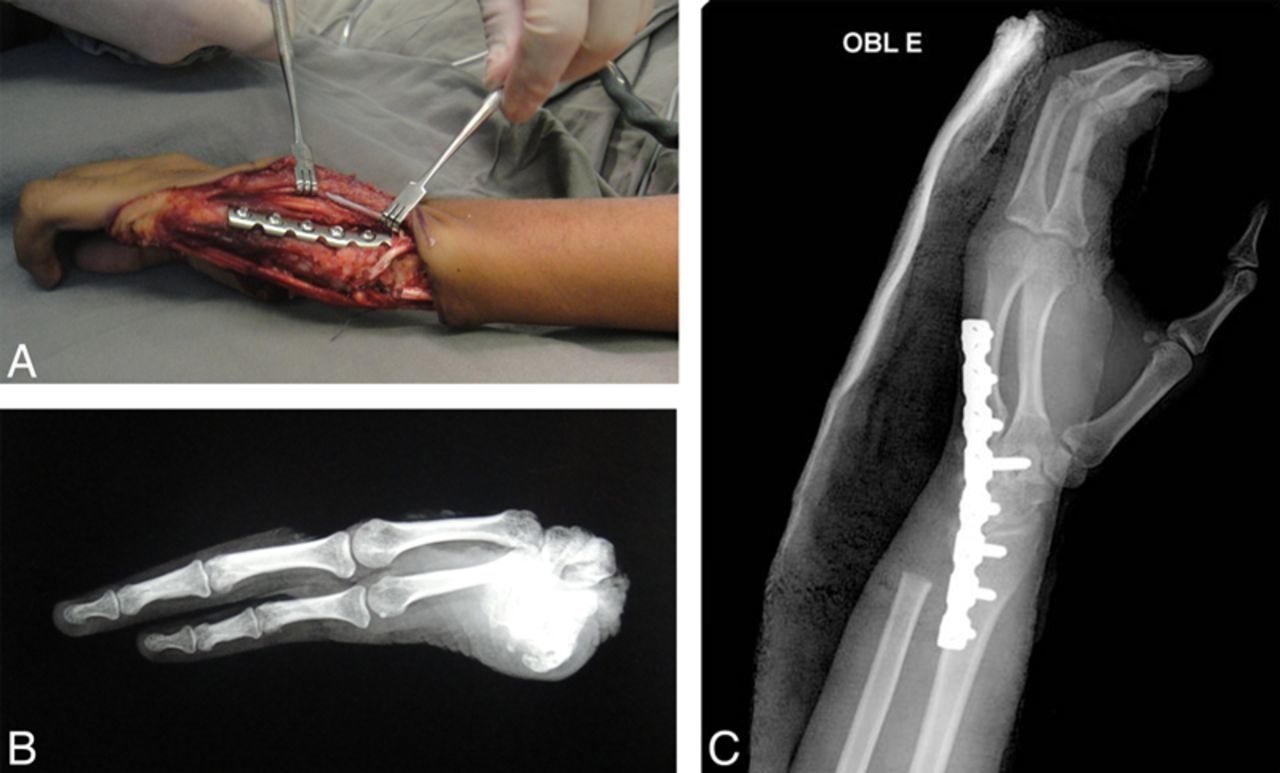
Arthrodesis of the wrist was performed to improve stability (Figs. 6-A, 6-B, and 6-C). The gross pathological findings confirmed an osteosarcoma mass that measured 3.0 × 2.5 × 2.0 cm. The tumor was infiltrating the adjacent wrist bones, and 100% of the tumor cells were viable (Huvos grade I). The margins of the specimen were disease-free (Figs. 5-A and 5-B).
After surgery, the patient received two additional cycles of adjuvant doxorubicin and ifosfamide. She then received a regimen of cisplatin and high-dose methotrexate combined with doxorubicin for three cycles. The doxorubicin was omitted in the fourth cycle since she had reached the cumulative dose of 375 mg/m. She was subsequently maintained on an oral regimen of cyclophosphamide and methotrexate for an additional sixteen months, according to the Brazilian Osteosarcoma Treatment Group Protocol.
Two months after the resection, the patient had full recovery of function and sensitivity of the median nerve, and she was able to perform opposition with the first and second fingers. Six months after the resection, she had no evidence of local recurrence and was tolerating oral adjuvant chemotherapy. At that time, she underwent a tenolysis of the middle finger extensor tendon to improve grip function (Figs. 7-A through 7-D). At the twenty-three-month follow-up, the patient was no longer receiving any treatment, had no signs of local or systemic recurrence, and continued to have satisfactory motor-sensory function.
Proceed to Discussion >>Reference: Bellan DG, Jesus-Garcia R, Teresa de Seixas Alves M, de Toledo M, Petrilli AS, Korukian M, Carai Maia V, Schoedl MF, Senerchia AA. Extraskeletal osteosarcoma of the hand in an adolescent: a case report. JBJS Case Connect. 2013 Jan-Mar;3(1):e6.
Conventional osteosarcoma arises in osseous structures, progresses to destroy the bone cortex, and invades the surrounding soft tissue. ESOS arises in soft tissue and may progress to infiltrate the adjacent bones. ESOS is extremely rare and usually develops during the fifth or sixth decade of life, although there are reports of its occurrence in the first through ninth decades. The most common presentation is a mass in the soft tissue without skeletal or periosteal attachment.
ESOS presents most frequently in the lower extremity, most often involving the soft tissues of the thigh. The prevalence of ESOS in the upper extremity ranges between 15% and 23%; 7% of these cases have occurred in the hand. Locations such as the pelvic and shoulder areas can also be involved. Up to 10% of cases have been reported in association with previous trauma or irradiation, but the etiological correlation of mechanical injury is difficult to assess.
Generally, ESOS has a poor prognosis. Almost all reported cases are high-grade tumors, with a five-year survival rate ranging from 24% to 50%. Local recurrence occurs in approximately 50% of the patients, and half of these sustain multiple recurrences following re-resection. The most frequent site of metastases is the lungs. Improved survival is observed with wide or radical resection as the initial surgery, but no survival advantage has been demonstrated comparing these two surgical techniques. When motor and sensory function of the distal end of the limb can be preserved, limb salvage is an optimal choice for surgical intervention. Most reports suggest that the only factor associated with extended disease-free survival is a tumor size smaller than 5.0 cm.
Because the role of adjuvant chemotherapy remains unproven, there is no standard chemotherapy protocol for ESOS. Two meta-analyses published in 1997 and 2008, respectively, have shown that doxorubicin-based chemotherapy serves to improve local control and progression-free survival. However, while there was a trend toward an overall survival benefit, it was not significant. The most recent report, however, demonstrated a significant overall survival advantage with the addition of ifosfamide to a doxorubicin regimen. While Ahmad et al. have suggested that such doxorubicin-based chemotherapy with the addition of ifosfamide and cisplatin is not active against ESOS, Goldstein-Jackson et al. reported that ESOS is more effectively treated with an aggressive multiagent chemotherapy regimen combined with appropriate surgery. The latter conclusion is also supported by the study by Torigoe et al. that demonstrated an overall five-year survival rate of 66% after use of multiagent chemotherapy.
This is a case of ESOS arising from the hypothenar muscles of the left hand in an eighteen-year-old woman, which was successfully treated with a multiagent chemotherapy regimen (doxorubicin, ifosfamide, cisplatin, and methotrexate) followed by surgery. Wide resection and partial limb salvage was the best option for our patient because of the intracompartmental location of the tumor. Although resection of this tumor required amputation of the fourth and fifth rays as well as the ulnar carpal bones to achieve margins free of tumor, the approach preserved the thumb and the index and middle fingers, allowing adequate motor sensory function (Figs. 7-A through 7-D). A below-the-elbow amputation would have fulfilled the oncological needs but would have caused substantial loss of function. Despite median nerve manipulation during the procedure, neurological function returned by eight weeks postoperatively. After a specific rehabilitation program with physiotherapy and a second surgical procedure for tendon release, the patient was able to perform bimanual activities of daily living.
Reference: Bellan DG, Jesus-Garcia R, Teresa de Seixas Alves M, de Toledo M, Petrilli AS, Korukian M, Carai Maia V, Schoedl MF, Senerchia AA. Extraskeletal osteosarcoma of the hand in an adolescent: a case report. JBJS Case Connect. 2013 Jan-Mar;3(1):e6.

What is the diagnosis?
Synovial chondromatosis
Osteochondroma
Extraskeletal osteosarcoma
Nora lesion (bizarre parosteal osteochondromatous proliferation [BPOP])
Tenosynovial giant cell tumor (giant cell tumor of tendon sheath, localized tenosynovitis)