

 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4A 6-year-old Chinese girl presented with pain over the right knee and right shoulder; at the age of 2 years, she had been diagnosed as having neurofibromatosis based on the presence of café-au-lait spots. Radiographs showed lytic changes in the proximal part of the right humerus, the distal part of the right radius, and the distal part of the right femur. Curettage and bone-grafting were performed in the right humerus and right femur in a local hospital. The histological findings at that time are not known.
At the age of 10 years, the patient presented with symptoms of right shoulder and right thigh pain after a minor injury. A nondisplaced fracture of the proximal part of the humerus was suspected on the radiographs. A radiolucent lesion with an impending fracture was noted in the diaphysis of the right femur. Her birth and developmental histories were normal; the family history was negative for features of type-1 neurofibromatosis and bone lesions. On physical examination, height and weight were appropriate for the patient’s age. There was a 5 cm × 6 cm area of alopecia on the right side of the scalp. Corneal leukoma was found in the right eye; no Lisch nodules were present. There were no signs of neurofibromas, optic glioma, hypogonadism, or cardiovascular malformations. Multiple large café-au-lait spots were present over the right side of the face and neck, right limbs, and right torso without axillary freckles. Only the right side was involved, and the spots did not cross the midline. The café-au-lait spots were “coast of Maine” type with ragged and irregular outlines. Hyperkeratosis was noted on some of the spots (Fig. 1). There was no evidence of scoliosis. Neurological examination was normal. The patient did not have mental retardation.
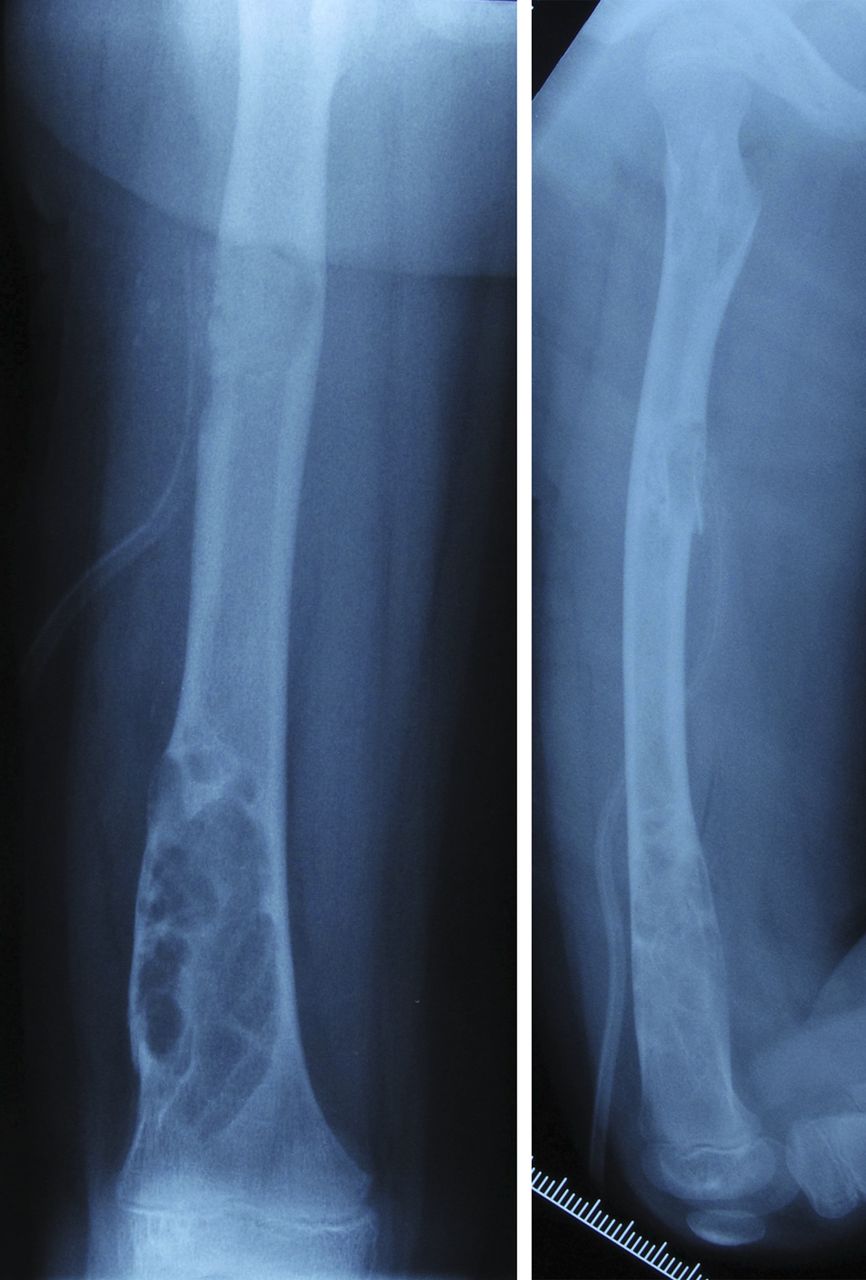
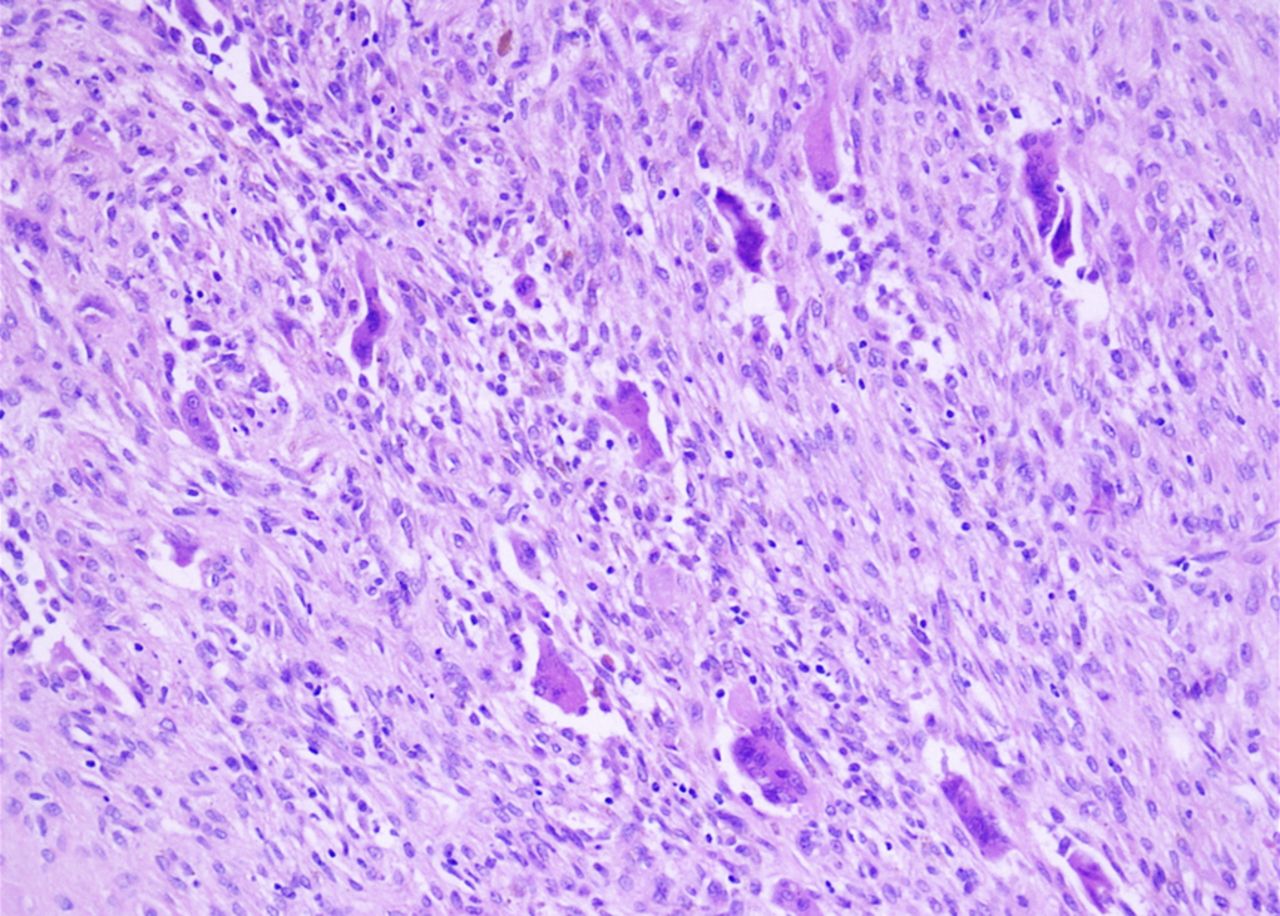
Radiographs showed demarcated osteolytic lesions in the metadiaphyseal regions of the proximal part of the right humerus, the distal part of the right radius, and the distal part of the right femur and femoral shaft (Fig. 2). Magnetic resonance imaging (MRI) of the brain and spine showed no abnormal findings. The right arm was placed in a sling, and the pain was relieved after 2 weeks. Biopsy and bone-grafting were performed for the right femoral diaphyseal lesion to prevent fracture, and full weight-bearing was permitted 2 months after surgery (Fig. 3). Histological examination of tissue from the right femur is shown in Figure 4.
Three months after surgery, the patient reported relief of pain and normal function in both the upper and lower right limbs.
The histology of the bone lesion indicated a non-ossifying fibroma. The patient was diagnosed with Jaffe-Campanacci syndrome.
Proceed to Discussion >>Reference: Yang C, Gong Y, Li C, Gu G, Liu J, Qi X. Jaffe-Campanacci syndrome: a case report and review of literature. JBJS Case Connect. 2012 Mar 14;2(1):e10.
Multiple café-au-lait spots and multiple nonossifying fibromas are 2 prominent features of the Jaffe-Campanacci syndrome. In our case, both skin and bone lesions were limited to the right side of the body. No café-au-lait spots crossed the midline. Kotzot et al. also reported a case of both skin and bone lesions restricted to only 1 side of the body. However, other reported cases had bilateral involvement. It was suggested that somatic mosaicism in early embryonic development was possibly responsible for the lateralization of the lesions.
To identify any possible nonossifying lesions, Colby and Saul suggested radiographs of the knee for patients suspected to have Jaffe-Campanacci syndrome. Nonossifying fibromas are likely to be located at the distal part of the femur or the proximal part of the tibia, but they can also be found in the upper limbs (as in our patient and some of the cases reported in the series by Campanacci et al.). Therefore, a skeletal survey is likely indicated to localize all of the lesions. Moreover, the lesions are not limited to the metaphysis of the tubular bones: they usually extend extensively into the diaphysis in Jaffe-Campanacci cases. We also found a skip lesion with an impending fracture of the femoral diaphysis in our patient. Hau et al. reported the case of a 15-year-old patient with Jaffe-Campanacci syndrome. In this patient, both of the lesions in the distal part of the femur were treated with intralesional excision, curettage, allograft strut-grafting, and plate fixation; healing was achieved 6 months after the operation. We performed a similar intralesional excision and allograft grafting, but, instead of rigid fixation, we suggested restricted weight-bearing for 3 weeks. Bone union was achieved after 6 months. These findings suggest that healing at the sites of the bone lesions was not impaired.
Jaffe-Campanacci syndrome has been most commonly reported in whites, but this case shows that it can also occur in the Asian population.
Although non-ossifying fibromas can be seen in neurofibromatosis type 1, multiple nonossifying fibromas accompanied by cutaneous café-au-lait spots indicate Jaffe-Campanacci syndrome. Mafucci syndrome is characterized by soft-tissue vascular lesions (hemangiomas or vascular malformations) along with multiple enchondromas. Cystic skeletal angiomatosis can be unilateral, but the lesions are vascular (not non-ossifying fibromas) and the syndrome lacks café-au-lait spots.
Reference: Yang C, Gong Y, Li C, Gu G, Liu J, Qi X. Jaffe-Campanacci syndrome: a case report and review of literature. JBJS Case Connect. 2012 Mar 14;2(1):e10.
What is the diagnosis?
Neurofibromatosis type 1
Neurofibromatosis type 2
Maffucci syndrome
Cystic skeletal angiomatosis
Jaffe-Campanacci syndrome