A 67-Year-Old Woman with Diabetes and Worsening Hip Pain
December 5, 2018
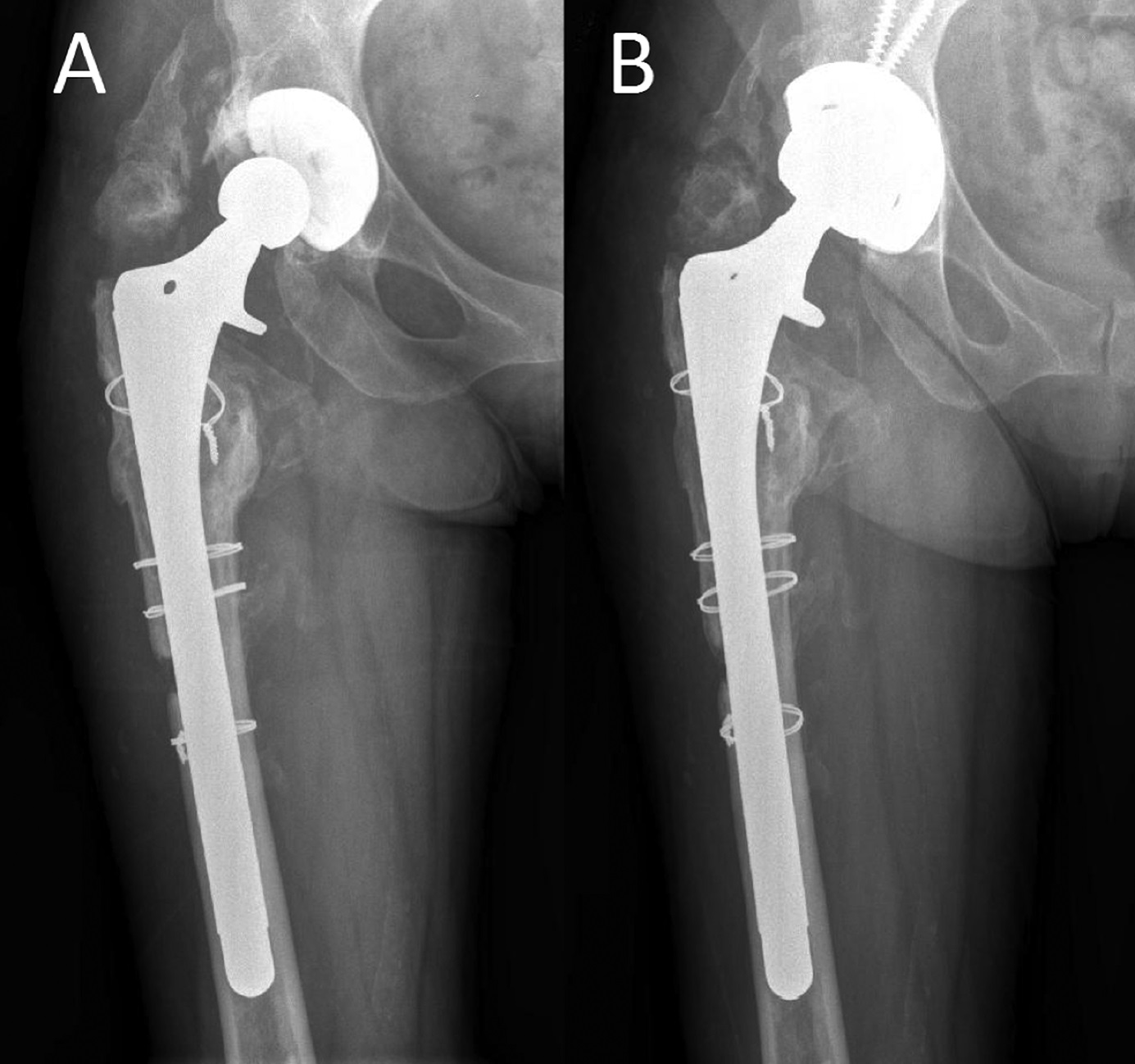
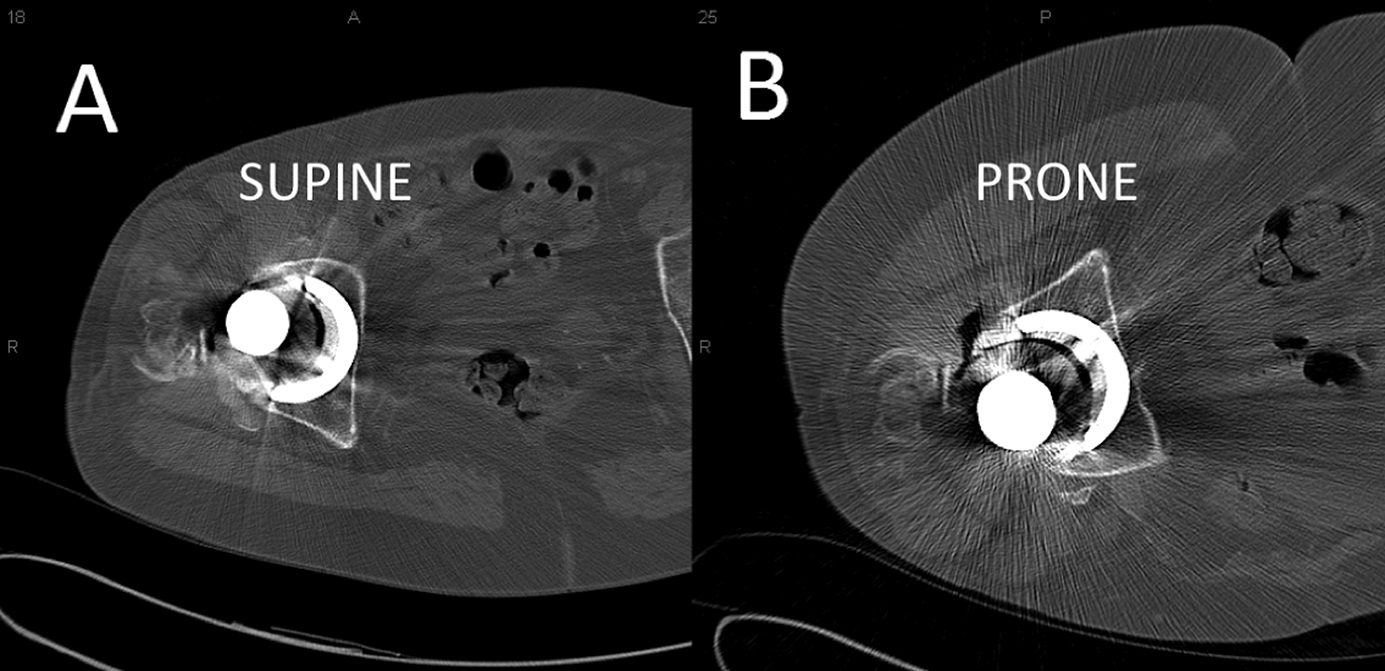
 Fig. 1
Fig. 1 Fig. 2
Fig. 2A 67-year-old woman first presented with a 6-month history of progressive right hip pain and limited ambulation. The medical history was noteworthy for insulin-dependent diabetes mellitus as well as systemic lupus erythematosus treated with prednisone. The patient had undergone multiple right hip operations. The primary total hip arthroplasty for osteonecrosis had been performed at an outside institution 12 years prior to presentation. The patient had experienced a difficult postoperative course, which included multiple dislocations of the primary total hip arthroplasty and a deep infection that required irrigation and debridement with a head and polyethylene liner exchange 3 years after the primary total hip arthroplasty. She did well for a few years, but developed progressive right hip pain and difficulty with ambulation. She was referred to our institution for additional management. The initial radiographs (not included in this report) revealed mature heterotopic ossification, substantial femoral osteolysis, loosening of the femoral component, and extensive eccentric wear of the polyethylene liner. Based on these clinical and radiographic findings, she underwent re-revision total hip arthroplasty.
The femoral component was removed through an extended trochanteric osteotomy. The acetabular liner demonstrated extensive wear and was removed, but the metal shell was manually tested and found to be well-fixed onto the pelvis. The femur was revised with a fully porous-coated stem that was 8 in (20.3 cm) long (VerSys; Zimmer). The hip was trialed and was found to be unstable secondary to the native position of the acetabular component. A decision was made to retain the acetabular component because of poor periacetabular bone quality and potential complications associated with removing the metal shell. The acetabulum was prepared by roughening of the acetabular component with a metal-cutting burr. Next, a 7-mm offset polyethylene liner (Longevity; Zimmer) with a diameter that was 4 mm smaller than the inner diameter of the cup was cemented into the acetabular component after roughing of the nonarticular surface. The lateral portion of the liner was supported by host bone. The cement was allowed to cure; the hip was re-trialed and was stable through the flexion-extension arc.
At 1 year postsurgery, radiographs revealed a healed osteotomy with bone ingrowth on the femoral side and no evidence of migration or radiolucencies around the acetabulum. The patient was able to walk without any aids.
At 14 months postsurgery, the patient sustained a fall. She was evaluated in the emergency room, and no fractures were reported. She returned to the clinic 8 weeks later and noted activity-related pain in the anterior aspect of the thigh. Radiographs failed to reveal any structural changes (Fig. 1-A), and overall, there were no apparent radiographic changes in comparison to the prior radiographs. She was treated nonoperatively but continued to have increasing pain and leg weakness with weight-bearing. The values for the infectious workup, which included white blood-cell count, erythrocyte sedimentation rate, and C-reactive protein level, were within normal limits. A technetium-99 bone scan did not demonstrate occult fracture or component loosening. At 4 months post-trauma, the patient continued to experience pain. A double-contrast computed tomographic (CT) arthrogram was performed under local anesthesia. Aspiration of joint fluid and injection of 2 cc of iodinated contrast agent confirmed the needle placement. A total of 15 cc of air then was injected into the joint. After injection, the patient underwent CT in the supine (Fig 2-A) and prone (Fig 2-B) positions.
There was a crescent-shaped air-fluid level between the liner and the cement (Fig. 2-A). There was air in the superior (anterior aspect of the hip) part of the interface, and the contrast iodine had settled inferiorly (posterior aspect of the hip). The double contrast of the air-fluid levels changed when the patient was repositioned from the supine to the prone position (Fig. 2-B). The air remained superiorly with the patient in the supine and prone positions, suggesting a continuous space between the liner and the cement, indicating debonding of the polyethylene liner from the cement mantle in the acetabular shell. Additionally, no radiolucencies or air levels were detected around the acetabular component.
The patient underwent another revision surgery of the acetabular component through the same anterolateral approach, at which time the liner was found to be completely loose. The metal shell was carefully removed and replaced with a 60-mm cementless metal-backed acetabular component (Trabecular Metal Cup; Zimmer), which was stabilized with screws. A 36-mm femoral head and the corresponding polyethylene liner were inserted. The hip was found to be stable intraoperatively. No additional complications were noted. At 3 years following this revision surgery, the patient was doing well and walking without aids (Fig. 1-B).
Proceed to Discussion >>Reference: Chauhan A, Fitzpatrick S, Sciulli RL, Sotereanos NG, Sewecke JJ. Using double-contrast CT arthrography to confirm suspected dissociation of a cemented polyethylene liner in the setting of revision total hip arthroplasty: a case report. JBJS Case Connect. 2017 Apr-Jun;7(2):e34.
Removal of a stable well-fixed acetabular component during revision surgery is often difficult and time-consuming. Increased rates of complications associated with bone loss and fracture of the acetabulum have been associated with this procedure.
In 1998, LaPorte et al. reported 8 cases of nonmodular metal-backed acetabular components in which cement was used to fix a new liner into the metal shell. Biomechanical studies reported that a cemented liner was more stable than some of the available locking mechanisms, and stable enough to withstand loads applied by a hip simulator. Therefore, the use of a liner with a diameter that is 4 mm smaller than the metal shell is recommended. Based on these findings, cementing a liner into a well-fixed acetabular component became popular when the locking mechanism was at fault, a matching liner was not available, or there was malpositioning of the cup noted intraoperatively.
Although early clinical results with this technique were favorable, failures at the cement-liner interface have been reported, and appear to be related to the cementing of constrained liners or to liners with a diameter larger than the diameter of the retained cup. To our knowledge, a total of 4 failures at the cement-liner interface have been reported. We were unable to find any reported cases of failure of the cement-cup interface to date. Herein, we describe a failure in 1 patient in whom a 7-mm offset polyethylene liner had been used. Although the onset of the symptoms was trauma-related, the fact that a considerable part of the liner was not supported by the shell might have played a role in the fate of the construct. Dissociations of the liner in modular acetabular systems also have been previously reported and have been linked with inadequate locking mechanisms of specific designs.
Acute onset of groin pain, limited motion, and instability are the most common symptoms associated with dissociation of polyethylene liners. Most patients also report clicking of the joint with walking. Dislocation of the hip joint may occur. Our patient described pain, weakness, and limited motion initiated by trauma. The symptoms did not alter over a period of 4 months, and she had difficulty performing daily activities.
In cases where the liner has been displaced inferiorly, asymmetric placement of the femoral head into the acetabular component is apparent on plain radiographs. According to a recent review of 9 cases of dissociation of modular cups, a crescent-shaped radiolucency medial to the femoral head always was present in the anteroposterior radiograph of the pelvis, in addition to the eccentric placement of the head. The authors refer to this finding as the “crescent sign.” Similar radiographic findings have been reported by others.
According to some reports, radiographs are not always adequate to diagnose polyethylene liner dissociation. Dynamic testing under fluoroscopic control, arthrography and postarthrography CT, and metal artifact reduction sequence magnetic resonance imaging (MARS MRI) have been proposed in such cases. CT arthrography has been used in the presence of artificial joints to confirm loosening of components. Air-contrast CT arthrography has been used to detect labral lesions in the shoulder and disorders of the temporomandibular joint. MARS MRI has been used to diagnose periprosthetic fractures, bone resorption and osteolysis, postoperative hematoma, disruption of the pseudocapsule, synovitis caused by polyethylene wear and adverse local tissue reactions, periprosthetic masses and neoplasms, bursitis, tendinopathy and tendon tears, and neurovascular compromise. To our knowledge, this is the first report of the use of positional double-contrast CT arthrography to detect pathology in a total hip arthroplasty.
In our patient, multiple radiographs failed to reveal any abnormality. An old fracture of the greater trochanter and heterotopic ossification could have accounted for the pain; correlation with interpretation of radiographs is difficult. Also, no crescent sign and no head asymmetry were detected on radiographs. It should be noted that the patient did sustain a fall, which could have contributed to the dissociation. However, radiographs obtained after the fall did not demonstrate any changes in the prosthesis orientation from previously obtained postoperative radiographs. The possibility that the cement never had adhered to the polyethylene liner cannot be excluded.
In this patient, air in the interface between the polyethylene liner and the cement mantle suggested dissociation of the liner. In order to ensure that the liner was completely detached from the cement, double-contrast CT arthrography was performed in both the supine and prone positions. Propagation of air through the interface was documented because the air in both positions remained on the most superior part of the gap, and the radiolucency was deemed to be circumferential. Asymmetry of the head in relation to the metal shell was apparent only in the CT reconstruction image after the distension of the capsule with air. Although rare, dissociation of a polyethylene liner cemented into a previously implanted metal shell may occur, and its diagnosis may be uncertain. In such instances, double-contrast CT arthrography could be a valuable confirmatory tool.
Reference: Chauhan A, Fitzpatrick S, Sciulli RL, Sotereanos NG, Sewecke JJ. Using double-contrast CT arthrography to confirm suspected dissociation of a cemented polyethylene liner in the setting of revision total hip arthroplasty: a case report. JBJS Case Connect. 2017 Apr-Jun;7(2):e34.
What is the diagnosis?
Pseudotumor likely related to corrosion products
Dissociation of a dual-mobility polyethylene liner
Dissociation of the modular femoral head from the trunnion of the femoral component
Debonding of the polyethylene liner from the cement mantle in the acetabular shell
Loosening and migration of the metal acetabular shell