Continuing Elbow Pain in a Twelve-Year-Old Boy Following Impact of a Helmet to the Hyperflexed Elbow During a Football Game
October 6, 2010


 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3
Fig. 3A twelve-year-old, right-hand dominant, otherwise healthy boy was referred to our center for consultation after having pain in the left elbow for approximately five weeks. The patient had no history of elbow problems and had experienced no musculoskeletal problems prior to the onset of pain. The birth history was normal and all developmental milestones had been achieved within the normal age ranges. Five weeks prior to our evaluation, the patient had sustained a direct impact injury to the hyperflexed left elbow during a football game. His elbow struck the helmet of an opponent, after which the patient immediately experienced pain in the elbow. He sat out for several plays and then returned to the game without appreciable discomfort, although he lacked full motion in the elbow. The patient continued to compete and continued to have elbow problems for the remainder of the football season. Occasionally, he would describe a sensation of locking to his parents, who noticed that he intermittently favored his left elbow in daily activities. These problems prompted a visit to a local orthopaedic surgeon, who obtained radiographs and a magnetic resonance imaging scan, after which the patient was referred to our center for definitive treatment. On physical examination and comparison of both elbows at our center, the left elbow was noted to have minimal soft-tissue swelling and a small, palpable joint effusion. There was full pronation and supination of the forearm bilaterally, but the left elbow lacked 5° of extension and had 135° of flexion in comparison with the right elbow, which exhibited 5° of hyperextension and 150° of flexion. There was tenderness to palpation over the posterolateral gutter of the left elbow. During both active and passive elbow motion, a catching and grinding sensation was appreciated through the flexion-extension arc. Plain radiographs revealed a congruent elbow joint that had open growth plates and appropriate ossification for the age of the patient and had no obvious loose bodies. Magnetic resonance imaging is presented in Figure 1-A and 1-B.
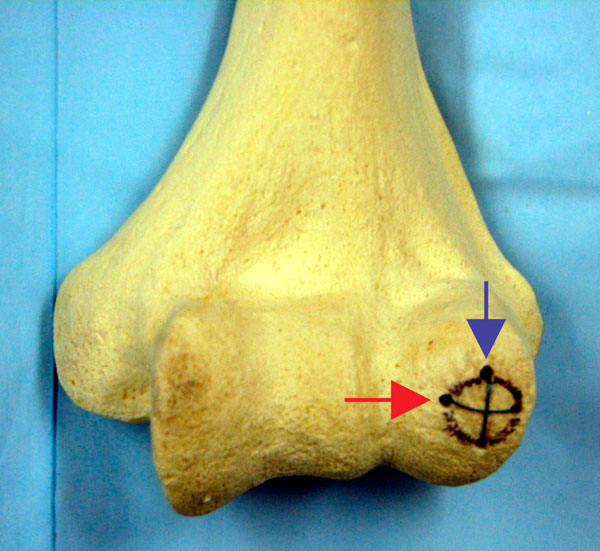
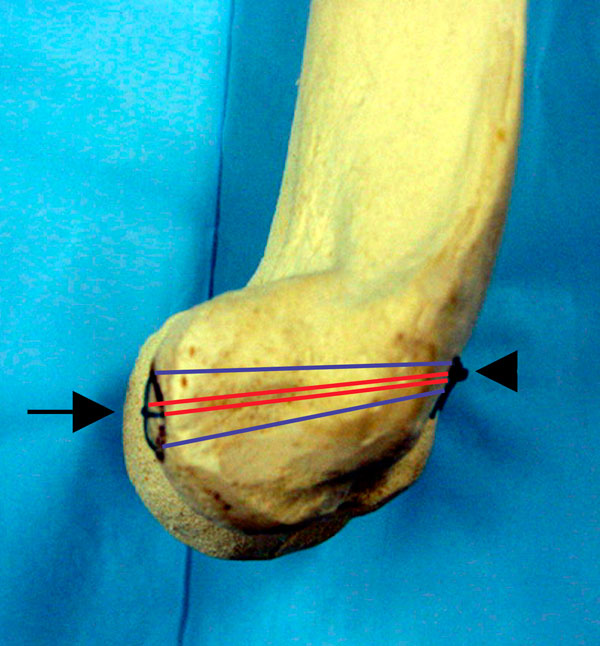
The magnetic resonance scan showed a small effusion as well as a coronal shear fracture of the capitellum, with the fracture fragment lying in the posterolateral gutter of the elbow (Figs. 1-A and 1-B). The capitellar defect measured 8 mm by 9 mm and was concave in shape. Surgical Technique The patient underwent arthroscopy of the left elbow, which revealed diffuse synovitis and a large osteochondral defect in the articular surface of the capitellum. The cartilaginous capitellar fragment was visible in the posterolateral gutter, and it was determined that an anatomic repair could only be accomplished through an open arthrotomy. A posterolateral approach was made through the Kocher interval, with care taken to remain anterior to the lateral ulnar collateral ligament and to preserve the posterolateral soft-tissue sleeve. The osteochondral fragment was removed from the joint, and a thin rim of subchondral bone and calcified cartilage was seen on its deep surface. The fracture fragment was then reshaped to match the capitellar defect, and the capitellar bed was débrided of fibrous tissue back to bleeding subchondral bone. The loose fragment was attached to the capitellum with chondral darts (Arthrex, Naples, Florida), resulting in only partial stability of the fragment with rotation and flexion-extension across the radiocapitellar articulation. This fixation was deemed unsatisfactory, and the darts were removed. Two horizontal mattress sutures (1-0 Vicryl; Ethicon, Somerville, New Jersey) were then placed across the fracture fragment in an "x" configuration with use of a smooth Keith needle (Figs. 2-A and 2-B). This suture technique achieved both stable fixation and compression of the fracture fragment. The wound was closed in the usual fashion and the elbow was placed in a soft dressing with a sling for comfort, and the patient was allowed to begin immediate elbow motion. At the time of the three-month follow-up, the patient had no symptoms of mechanical problems in the left elbow. There was no pain and no tenderness to palpation over the capitellum or the posterolateral gutter. Range of motion of the left elbow had improved to 0° of extension and 145° of flexion, with full forearm pronation and supination. The patient had returned to sports and had no elbow discomfort or limitations. A repeat magnetic resonance imaging scan revealed restoration of the contour of the capitellar articular surface with healing of the Kocher-Lorenz fragment (Fig. 3). At the time of the fourteen-month follow-up, the patient was continuing to do well and had no pain, swelling, or mechanical symptoms. The anatomic carrying angle of the left elbow was maintained, and there was full pronation and supination of the elbow with a flexion-extension arc of 0° to 150°. The patient continued to participate in sports, including football and wrestling, without symptoms, and he stated that the elbow felt normal.
Proceed to Discussion >>Reference: Sodl JF, Ricchetti ET, Huffman GR. Acute osteochondral shear fracture of the capitellum in a twelve-year-old patient. A case report. J Bone Joint Surg Am. 2008;90:629-33.
Kocher-Lorenz fractures of the capitellum are rare in children. It is important to remember that these pure capitellar injuries may be missed on radiographs due to a lack of subchondral bone attached to the articular cartilage fragment. As a result, some authors have recommended routine arthrography if this injury is suspected clinically. We recommend magnetic resonance imaging as the study of choice for diagnosis and to determine the precise size and location of the articular fragment and associated soft-tissue injuries. Traditionally, treatment of Kocher-Lorenz fractures has often been by fragment excision because stable internal fixation is not easily achieved due to the small size of the fracture fragment. If fixation is attempted, Kirschner wires or screws have been utilized, but there is frequently not enough bone present to engage the wires or screw threads. We present a surgical method for treating these difficult fractures with use of a horizontal mattress suture cross-stitch technique. This method provides compression across the fracture site and achieves fracture stability, which allows immediate postoperative motion, obviates the need for implant removal, and facilitates the acquisition of high-quality magnetic resonance images postoperatively to assess healing. Following fixation, it is important that the elbow be moved through a full range of motion in the operating room to ensure that appropriate suture tensioning and fracture fragment stability are present. In patients with open physes, care must also be taken to leave the posterolateral soft-tissue sleeve of the elbow intact during the surgical approach to avoid compromising the vascular supply to the lateral column of the distal part of the humerus. To date, our patient has shown no signs of premature distal humeral physeal closure on either follow-up imaging or physical examination. This surgical technique is not likely to pose a serious risk of growth arrest because smooth Keith needles that are passed across the physis rarely cause injury to the physeal cartilage. Recent studies have shown no evidence of growth arrest with use of similar methods. In conclusion, the described suture technique can achieve stable fixation of a Kocher-Lorenz fracture of the capitellum with a low risk for growth arrest and should be considered as a surgical treatment option for this challenging fracture.
Reference: Sodl JF, Ricchetti ET, Huffman GR. Acute osteochondral shear fracture of the capitellum in a twelve-year-old patient. A case report. J Bone Joint Surg Am. 2008;90:629-33.



Radial head fracture
Lateral epicondyle fracture
Capitellar shear fracture