A 38-Year-Old Man with Long-Term Shoulder Pain
February 5, 2020
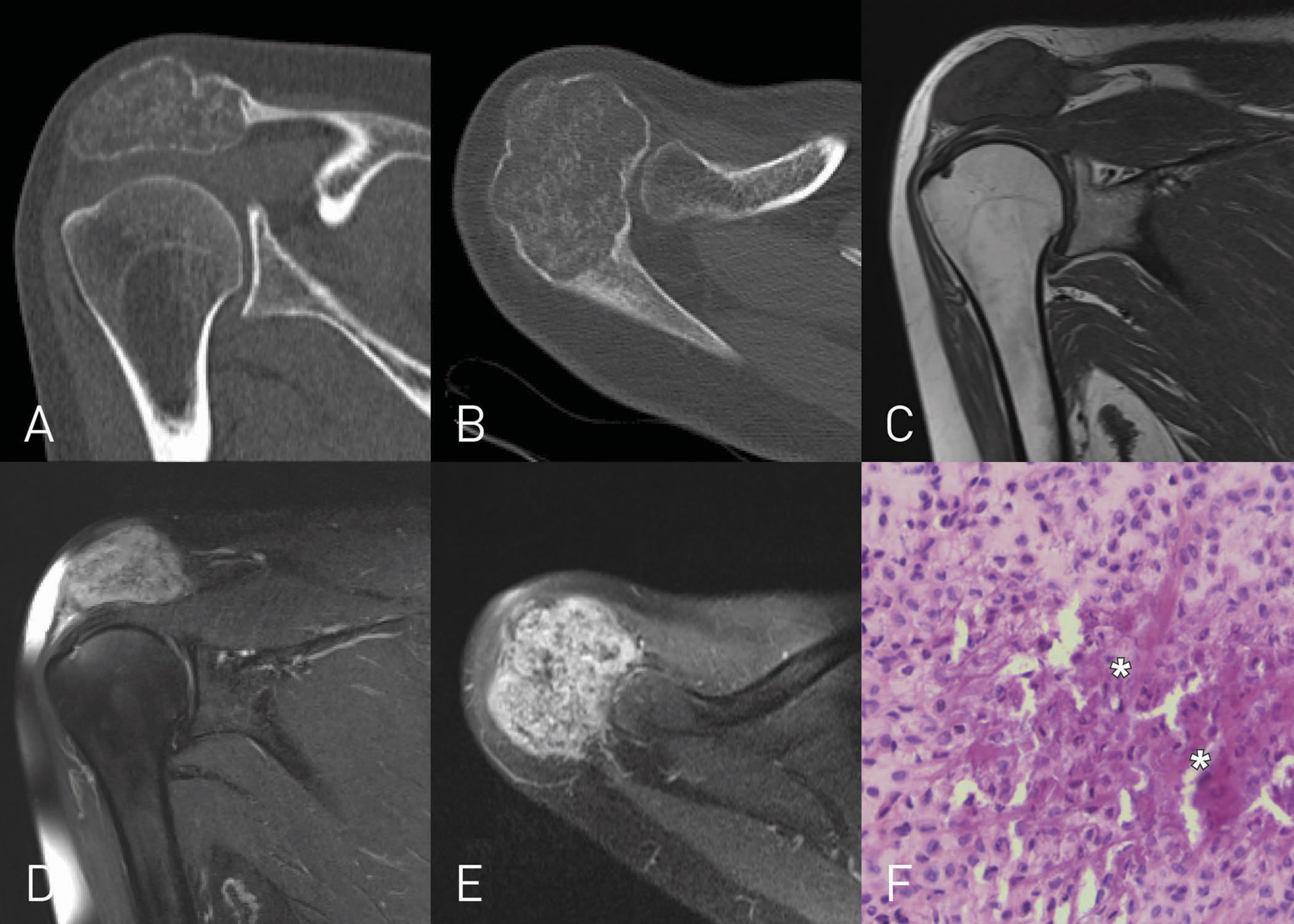
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3A 38-year-old man presented with pain in the right shoulder girdle with onset occurring approximately 1.5 years earlier.
Physical examination revealed shoulder asymmetry with a palpable mass in the acromial region. The patient experienced pain on palpation of the acromion. Also, active range of motion was moderately restricted because of pain. The patient presented active forward elevation of 150° and abduction of 160°, active external rotation of 50° with the arm at the side, and active internal rotation with the thumb reaching the spinous process L2. Because of pain and loss of strength, the patient was severely restricted during activities of daily living, was unable to work as a mechanic, and was unable to perform overhead activities.
Computed tomography (CT) showed an expansile osteolytic mass in the right acromion with intralesional calcifications (Figs. 1-A and 1-B). Magnetic resonance imaging (MRI) confirmed the presence of a lobulated mass (Figs. 1-C, 1-D and 1-E).
The histology of a biopsy is shown in Figure 1-F.
The biopsy showed uniform round to polygonal chondroid cells within an eosinophil matrix and characteristic “chicken wire” calcification (Fig. 1-F), diagnostic of a chondroblastoma. The patient underwent intralesional curettage and allogenic bone-grafting.
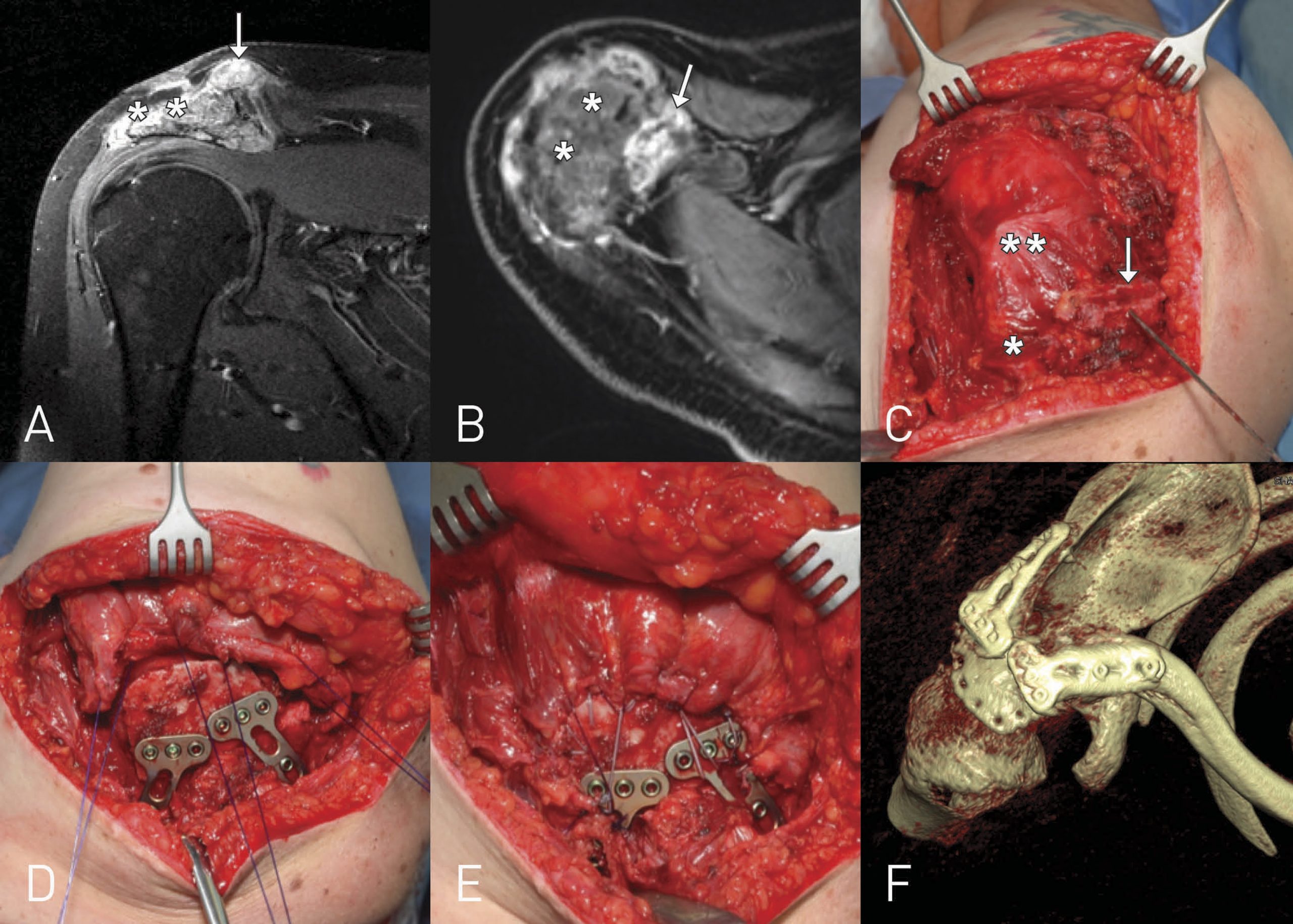
During regular follow-up visits, a local tumor recurrence was observed approximately 11 months after the first operation. At that time, the patient presented an active forward elevation of 150° and abduction of 140°, external rotation of 50° with the arm at the side, and active internal rotation with the thumb reaching the third lumbar vertebra. MRI presented tumoral lesions at the origin of the deltoid muscle and adjacent to the acromioclavicular joint (Figs. 2-A and 2-B), which was not accessible for a further curettage because of the large size of the lesion and the small residual acromion. CT of the thorax showed no evidence of metastases.
To preserve a functionally intact shoulder girdle, anatomical reconstruction of the acromion was performed as follows. Surgery took place in the left lateral position on a flat top table. A utilitarian S-shaped approach from the deltopectoral groove to the spine of the scapula with excision of the former incision exposed the acromion. After resection of the coracoacromial ligament at the coracoid process, the deltoid muscle was detached from the acromion. The osteotomy of the clavicle was performed 1 cm medial to the acromioclavicular joint, and the acromion was separated dorsally at the transition to spine of the scapula (Fig. 2-C). A tricortical, trapezoid-shaped graft was harvested from the middle portion of the iliac bone. Size and shape were estimated based on preoperative 3-dimensional CT analysis of the healthy contralateral side. It was prepared to a bicortical graft with cancellous bone edges to promote bone fusion and reinsertion of the deltoid muscle. The inner surface constituted the new undersurface of the acromion, and the thin central part was used for transosseous deltoid reinsertion. Two T-shaped angular stable plates (3.5-mm T-LCP; DePuy Synthes) were used to fix the graft at the spine of the scapula and the clavicle. The deltoid muscle was reattached with FiberWire sutures (Arthrex) through drilled holes at the anterior, lateral, and posterior borders of the graft, and sutures direct to the plates neutralized tension forces (Figs. 2-D through 2-F). Additional polydioxanone sutures (Ethicon) were used for soft-tissue adjustment and closure of the deltopectoral groove.
An inflatable shoulder abduction cushion (medi SAK; medi) was applied directly in the operating room with the shoulder flexed and abducted at 60°. Passive motion from 60° to 120° was allowed for 3 months. Thereafter, a 15° shoulder abduction splint (medi SAS 15; medi) was applied for another 6 weeks. Free passive motion and active-assisted exercises were allowed with transition to active exercises after 3 weeks.
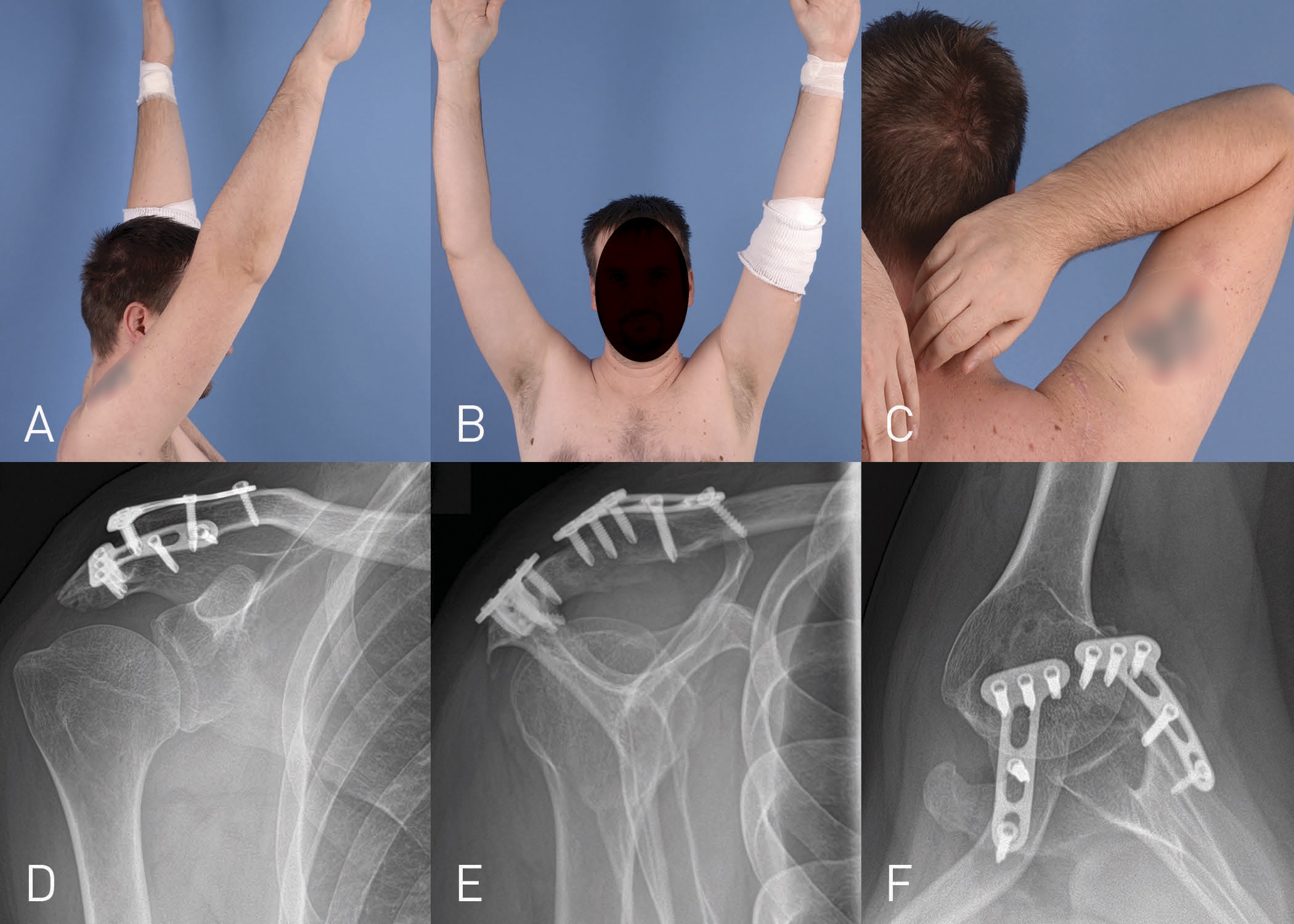
The patient exhibited steady improvement of active range of motion, and at the latest follow-up (17 months after surgery), he had forward flexion to 155° and abduction to 160°. External rotation was 50°, and internal rotation was to spinous process L3 (left shoulder: forward flexion 170°, abduction 170°, external rotation 60°, and internal rotation L1) (Figs. 3-A through 3-C). The Constant score was 77, demonstrating a good functional outcome. The evolution of the integration process was documented through follow-up visits with repeated MRI and CT scans and radiographs every 3 to 4 months, resulting in a radiologically healed graft after 7 months. There was no evidence of local recurrence at the latest follow-up of 17 months.
Proceed to Discussion >>Reference: Herget GW, Maier D, Südkamp NP, Uhl M, Füllgraf H, Dovi-Akue D. Anatomical reconstruction of the acromion using an autologous iliac crest graft for treatment of recurrent chondroblastoma. A case report. JBJS Case Connect. 2019 Jul-Sep;9(3):e0086.
Chondroblastoma is a rare, cartilage-producing bone tumor. It is characterized histologically by the proliferation of immature chondrocytes (chondroblasts) along with other secondary elements, such as mature cartilage, giant cells, calcification, and, occasionally, aneurysmal bone cyst formation. Most tumors are diagnosed in the second and third decades of life with a male predominance (2 to 1).
Chondroblastoma tends to be a solitary lesion. However, recently, a metachronous bilateral chondroblastoma of the proximal part of the femur was described. In young people, it preferentially occurs in the epiphysis of long tubular bones, with the most common sites being the proximal part of the tibia or femur, distal part of the femur, and proximal part of the humerus. In older individuals, the location is more variable, and tumors may involve nontubular bones such as the craniofacial skeleton or bones of the hands and feet. It is highly exceptional for the acromion to be involved, as in our case. It very rarely metastasizes—a benign metastasizing chondroblastoma—but does not transform into a high-grade tumor.
Clinical presentation typically consists of gradually increasing pain and local tenderness, followed by swelling and reduced range of motion of the adjacent joint. In our case, pain was the major symptom, the patient had a palpable mass on the acromion, and range of motion was restricted.
Surgery is the treatment of choice. The accepted method is curettage and filling of the bone defect with a bone graft, which generally results in satisfactory outcomes. Another treatment option represents the en bloc resection. Chemical (phenol) and electric cauterization or cryosurgery can be used as complementary therapy. However, the local tumor recurrence rate is relatively high, on the order of 14% to 18%, depending somewhat on the initial location.
The initial operation consisted of curettage and bone-grafting. Unfortunately, the chondroblastoma recurred, requiring a revision surgery.
In general, after resection of the acromion, the reattachment of the deltoid muscle is crucial to preserve a functional shoulder joint. Using an autologous iliac crest graft, we achieved an anatomical reconstruction of the acromion with transosseous reinsertion of the deltoid muscle, and the patient regained normal shoulder function without relevant deficits during activities of daily living. There was no evidence of recurrence at a follow-up of 17 months. Furthermore, radiographs demonstrated complete bony fusion of the iliac graft (Figs. 3-D through 3-F).
To the best of our knowledge, this is the first description of a functional and anatomical reconstruction of the acromion using an autologous iliac crest craft fixed with T-shaped angular stable plates. This surgical procedure is very beneficial for advanced tumors requiring resection of the acromion to restore and preserve a functionally intact shoulder girdle, particularly in young and functionally demanding patients. In contrast, conventional alternative methods such as acromial resection or shoulder arthrodesis are functionally debilitating and should be avoided whenever possible.
In conclusion, the initial tumor in the acromion was large, and achieving adequate curettage was likely difficult, making local recurrence not unanticipated. Resection followed by autologous iliac bone-graft fixation demonstrated a good clinical outcome, without evidence of local recurrence at 17 months after secondary surgery.
Therefore, this surgical procedure could be considered for large, expansile lesions in this location for which adequate curettage would leave little remaining bone that might compromise function.
Reference: Herget GW, Maier D, Südkamp NP, Uhl M, Füllgraf H, Dovi-Akue D. Anatomical reconstruction of the acromion using an autologous iliac crest graft for treatment of recurrent chondroblastoma. A case report. JBJS Case Connect. 2019 Jul-Sep;9(3):e0086.
What is the diagnosis?
Amyloidoma
Langerhans cell granuloma (eosinophilic granuloma)
Osteosarcoma
Chondroblastoma
Osteomyelitis