A 76-Year-Old Woman with Hip Pain Following a Fall
June 2, 2021

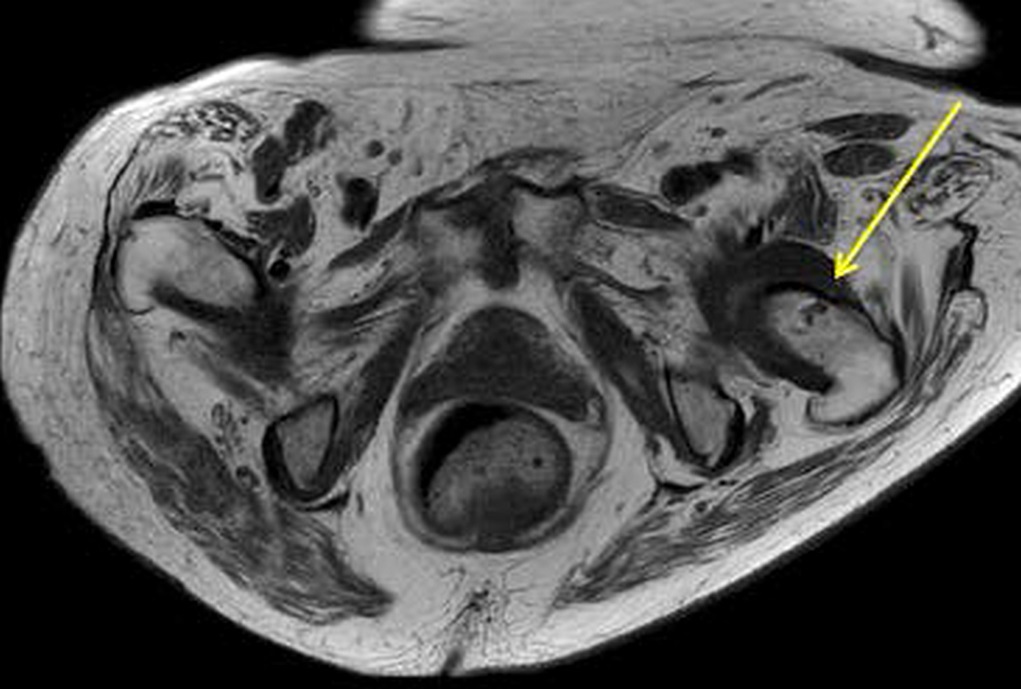
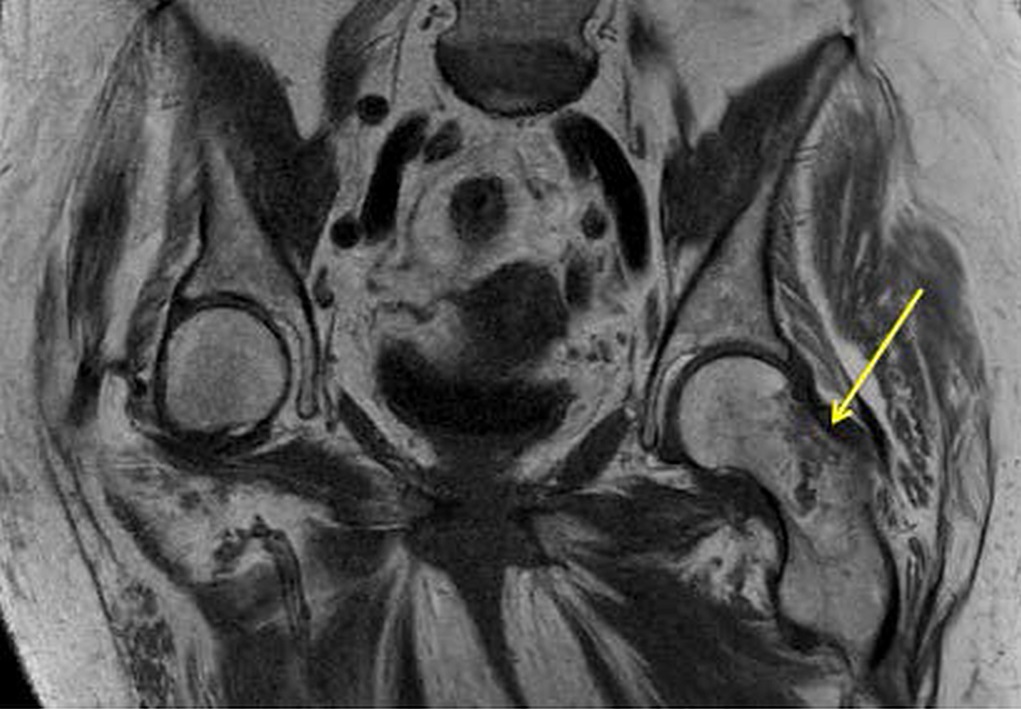
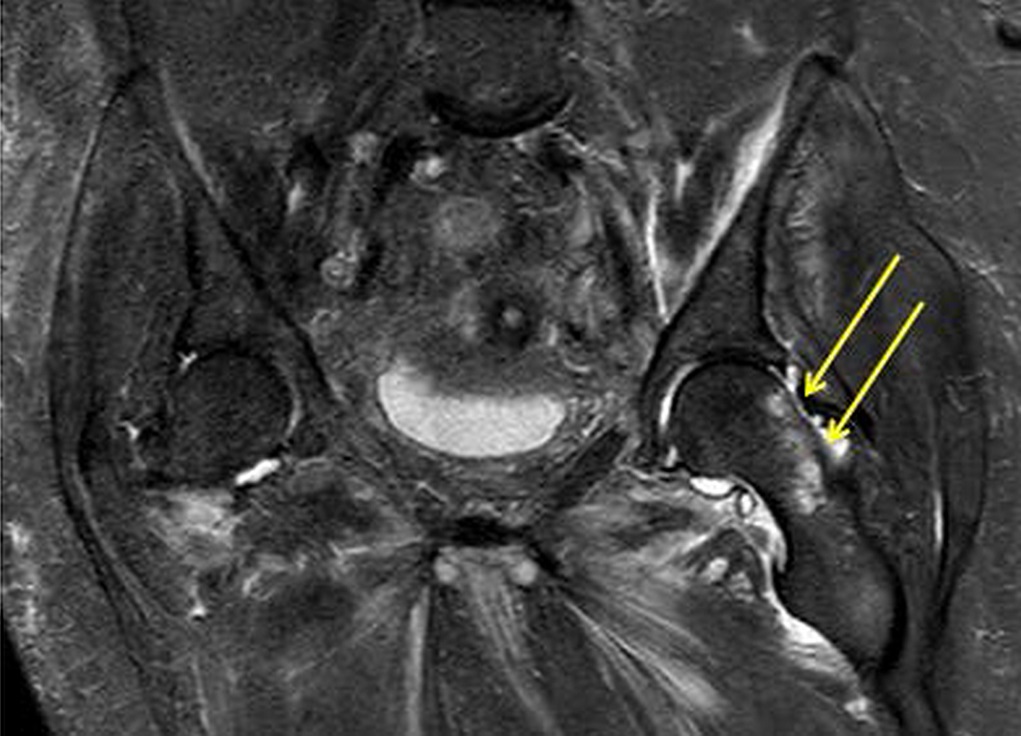
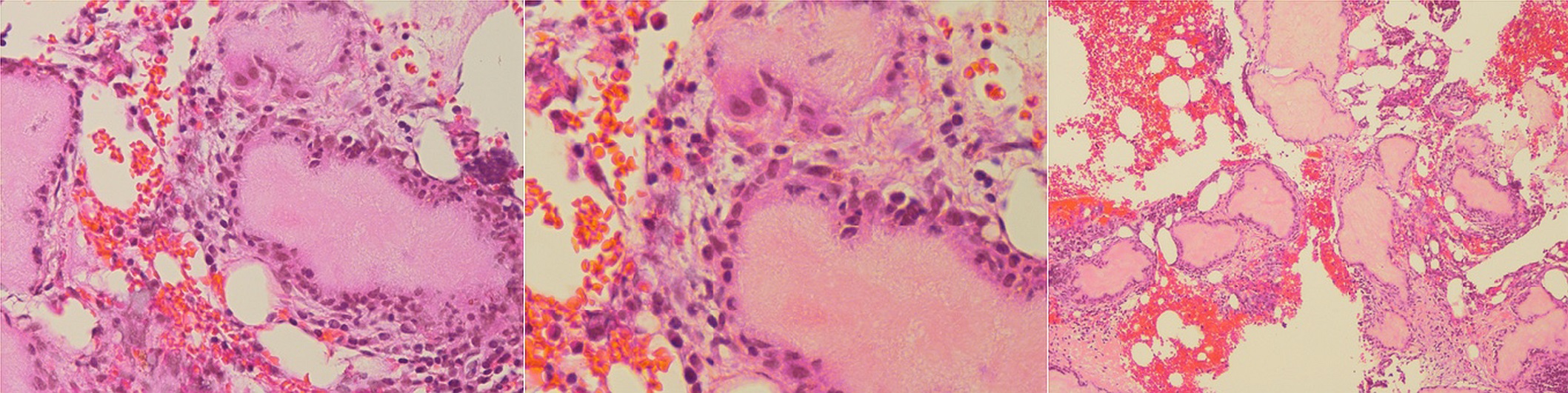
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 6
Fig. 6 Fig. 7
Fig. 7A 76-year-old woman presented to the emergency department reporting symptoms of left hip pain after a fall from her wheelchair.
At baseline, the patient required assistance with activities of daily living and used both a walker and a wheelchair for assistance. Her medical history was notable for atrial fibrillation, diastolic heart failure, pulmonary hypertension, type-2 diabetes, hyperlipidemia, and chronic kidney disease. She did not report substantial joint pain or swelling.
A screening dual x-ray absorptiometry (DXA) scan performed 3 days before her fall demonstrated a bone mass density (BMD) of the femoral neck as 0.631 g/cm2 (−2.0 T-score) and BMD of the left hip as 0.725 g/cm2 (−1.8 T-score). Based on these results, her 10-year risk for a major osteoporotic fracture was determined to be 13% and that for a hip fracture was determined to be 3.4%.
On examination, the patient was noted to have ecchymosis of the lateral soft tissues of the left hip and moderate tenderness to palpation over the greater trochanter and proximal part of the femur. Passive range of motion of the hip was limited, secondary to pain, but she maintained active knee flexion and extension.
A radiograph of the left hip and pelvis demonstrated coxa profunda and Tonnis-2 osteoarthritis without evidence of fracture (Fig. 1). A computed tomography (CT) scan revealed osteopenia without evidence of a displaced fracture. Due to the relatively benign imaging and the patient’s inability to bear weight, a magnetic resonance image (MRI) was pursued to investigate an occult fracture. The MRI scans demonstrated a nondisplaced fracture of the femoral neck with an associated joint effusion (Figs. 2, 3, and 4). Laboratory evaluation revealed an elevated C-reactive protein (CRP) of 26 mg/L (<5-mg/L range) and a serum uric acid of 13.4 mg/dL (2.5 to 8.3-mg/dL range). Given her examination and associated imaging, the decision was made to proceed with an open biopsy, followed by operative fracture stabilization via cephalomedullary nailing pending biopsy results.
A lateral approach was chosen for the biopsy and cephalomedullary nail. Because the fascia was incised, light chalky-tinged fluid was encountered. On evaluation of the left femoral neck, powdery tissue with a large osseous cyst was identified. Once removed, the specimen was white in color with a chalky consistency and was sent for frozen section along with crystal and microbiologic evaluation. There was no displacement or gross instability at the fracture site with no suspicion of infection or malignancy on frozen section, so we proceeded with cephaomedullary nail fixation as planned.
In total, 4 specimens were sent for analysis: 1 from the femoral reamings and 3 from the femoral neck. Of the 3 femoral neck specimens, 2 were fixed in formalin and 1 was fixed in ethanol. The first specimen in formalin was a gray-dark green tissue measuring 1.2 × 0.9 × 0.1 cm. The second specimen in formalin was a gray-tan brown tissue measuring 1.3 × 0.5 × 0.5 cm. The third specimen was fixed in 100% ethanol. Hematoxylin and eosin (H&E)-stained sections are shown in Figure 5.
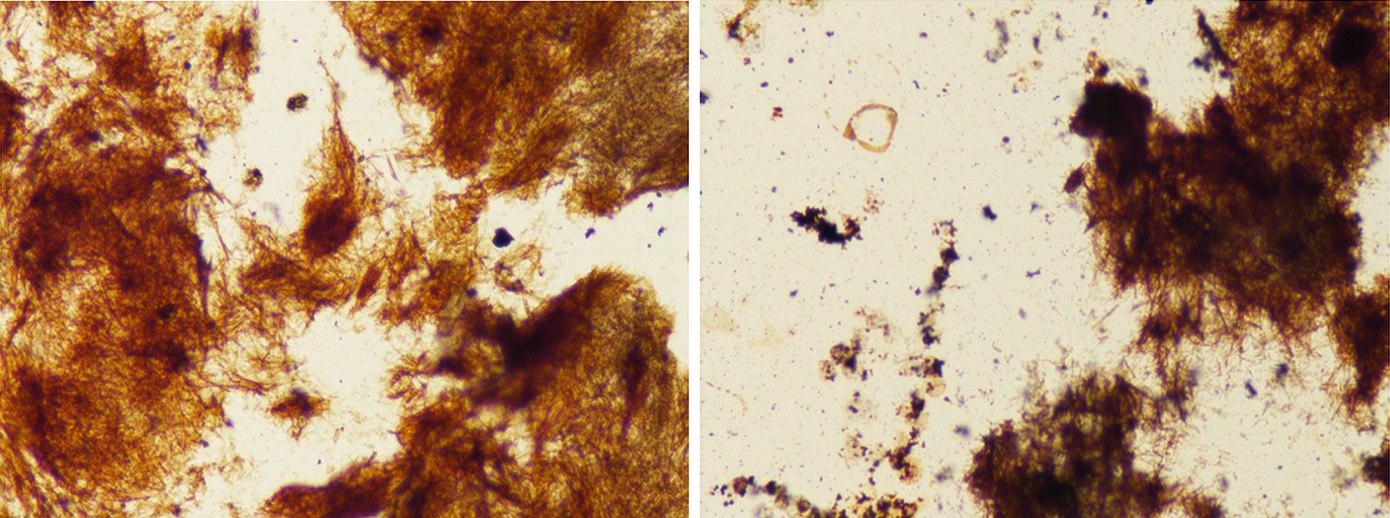
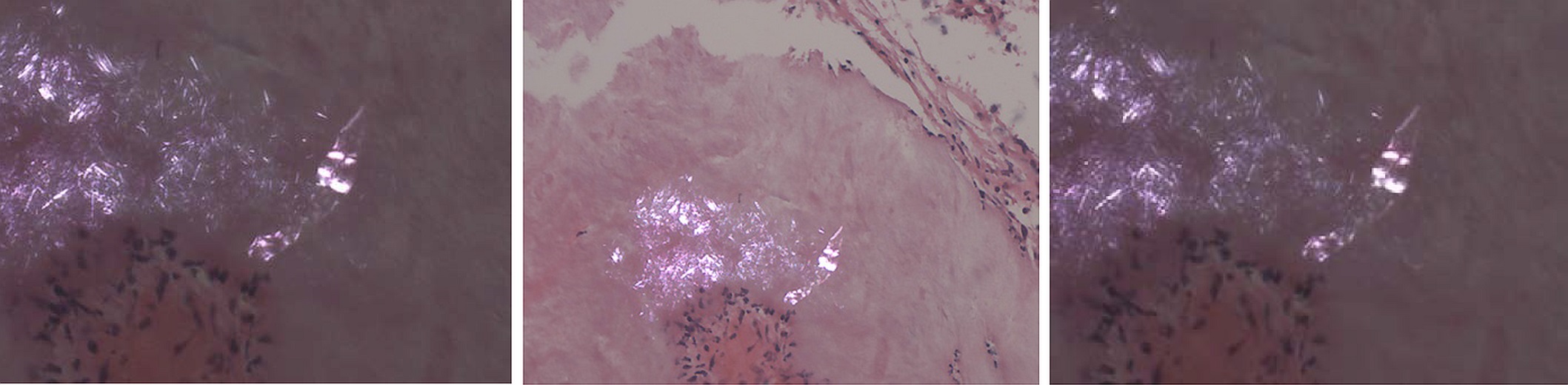
The combination of routine histology, a special stain, and the use of polarized light to demonstrate needle-shaped crystals is diagnostic of uric acid deposition (tophaceous gout).
The individual urate crystals cannot be seen on the H&E stain because they are often dissolved in the process. Therefore, the De Galantha stain, a silver stain performed on alcohol-based tissue, was used to reveal long, needle-shaped urate crystals (Fig. 6). In addition, polarized light was used to demonstrate needle-shaped, negatively birefringent crystals consistent with gout (Fig. 7).
The left femoral neck tissue and femoral canal reamings did not demonstrate signs of malignant neoplasm and were negative for acid-fast bacilli, aerobic bacteria, anaerobic bacteria, and fungus. A peripheral blood sample tested negative for bacterial growth, and urine culture obtained from the catheter yielded no growth.
At the 2-week follow-up, radiographs demonstrated anatomic alignment without loosening or evidence of periprosthetic fracture. However, the patient was noted to be experiencing a decline in mental status since the surgical procedure. A head CT scan was obtained, which did not reveal acute findings. A urinalysis was obtained, which tested positive for Candida albicans (10,000 to 50,000 per mL), Citrobacter freundii complex (50,000 to 100,000 per mL), and Escherichia coli extended spectrum beta-lactamase (>100,000 per mL). Based on these results, an infectious disease consultation was obtained. In the following weeks, the patient developed elevated serum glucose, blood urea nitrogen (BUN), and creatinine and died 48 days after the surgical procedure.
Proceed to Discussion >>Reference: Parisien RL, Ment A, Shin M, Anand N, Martin EA. Pathologic hip fracture by virtue of a rare osseous manifestation of gout: a case report. JBJS Case Connect. 2020 Jul-Sep;10(3):e20.00231.
This report describes a rare case of a pathologic fracture of the femoral neck secondary to a tophaceous gouty lesion. Instances of pathologic fractures secondary to intraosseous gout are uncommon, with most reports describing cases involving the patella. To our knowledge, there have only been 2 previous reports of tophaceous gout-mediated femoral fractures in the literature involving patients with a known history of chronic gouty arthritis. This report differs in the respect that our patient did not have a known personal or family history of gout. However, her medical history was notable for hypertension, chronic kidney disease, and diabetes, all of which are known risk factors for gout. In addition, her fracture risk assessment (FRAX) score indicated a relatively low 10-year risk for hip fracture at 3.4%. These are salient points because they highlight the importance of maintaining an appropriate level of clinical suspicion of osseous gouty tophi-induced hip pain in patients with negative radiographs, low FRAX scores, and a comorbid profile placing them at risk for gout.
Given our patient’s symptoms, negative radiographs, and atypical findings on advanced imaging, the decision was made to biopsy the region during surgical intervention. Although surgical intervention is seldom required for the management of tophaceous gout, operative indications include osseous lesions associated with severe pain, joint destruction, and mechanical instability with particular vigilance required with identification of lesions in critical weight-bearing areas such as the hip and proximal part of the femur. In conjunction with hip fracture fixation, comprehensive medical management should focus on reducing uric acid levels and the mitigation of modifiable risk factors. After acute management with nonsteroidal anti-inflammatory drugs, allopurinol and febuxostat (xanthine oxidase inhibitors) are used to effectively reduce long-term concentrations of uric acid. As such, our patient was prescribed allopurinol for chronic management of the gout. However, her postoperative protocol followed that typically prescribed for cephalomedullary nailing of hip fractures as the gouty lesion was not anticipated to adversely affect the stability of fixation.
In conclusion, this report describes a pathologic hip fracture secondary to a rare osseous manifestation of the tophaceous gout in a patient with no known history of gout. We emphasize the importance of including this potential etiology in the differential diagnosis of elderly patients presenting with hip pain, with or without a known history of gout.
Reference: Parisien RL, Ment A, Shin M, Anand N, Martin EA. Pathologic hip fracture by virtue of a rare osseous manifestation of gout: a case report. JBJS Case Connect. 2020 Jul-Sep;10(3):e20.00231.
What is the diagnosis?
Tophaceous gout
Ochronosis (alkaptonuria)
Granulomatous inflammation suggestive of mycobacterial infection
Calcium pyrophosphate deposition
Findings consistent with previous tetracycline administration