 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
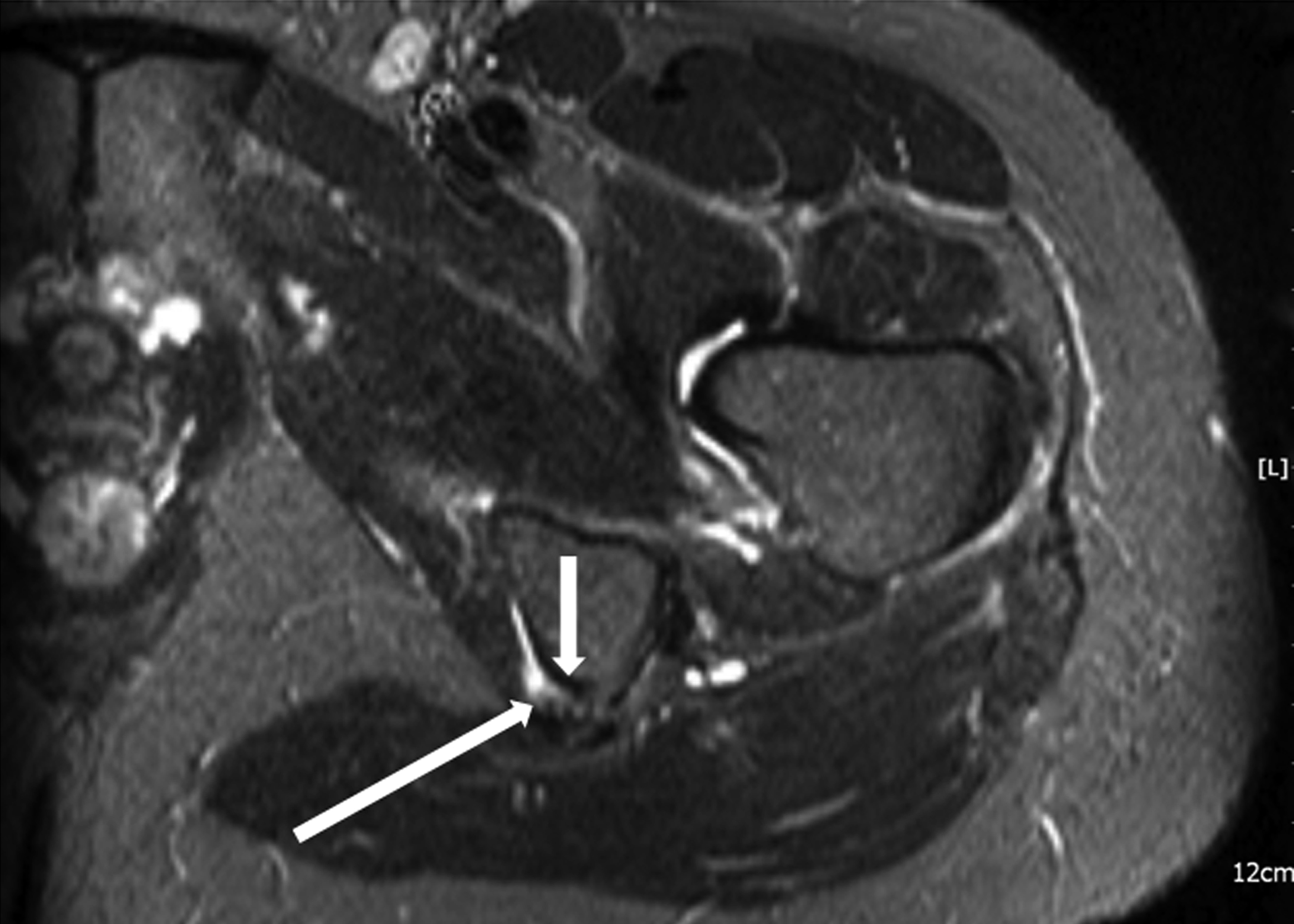
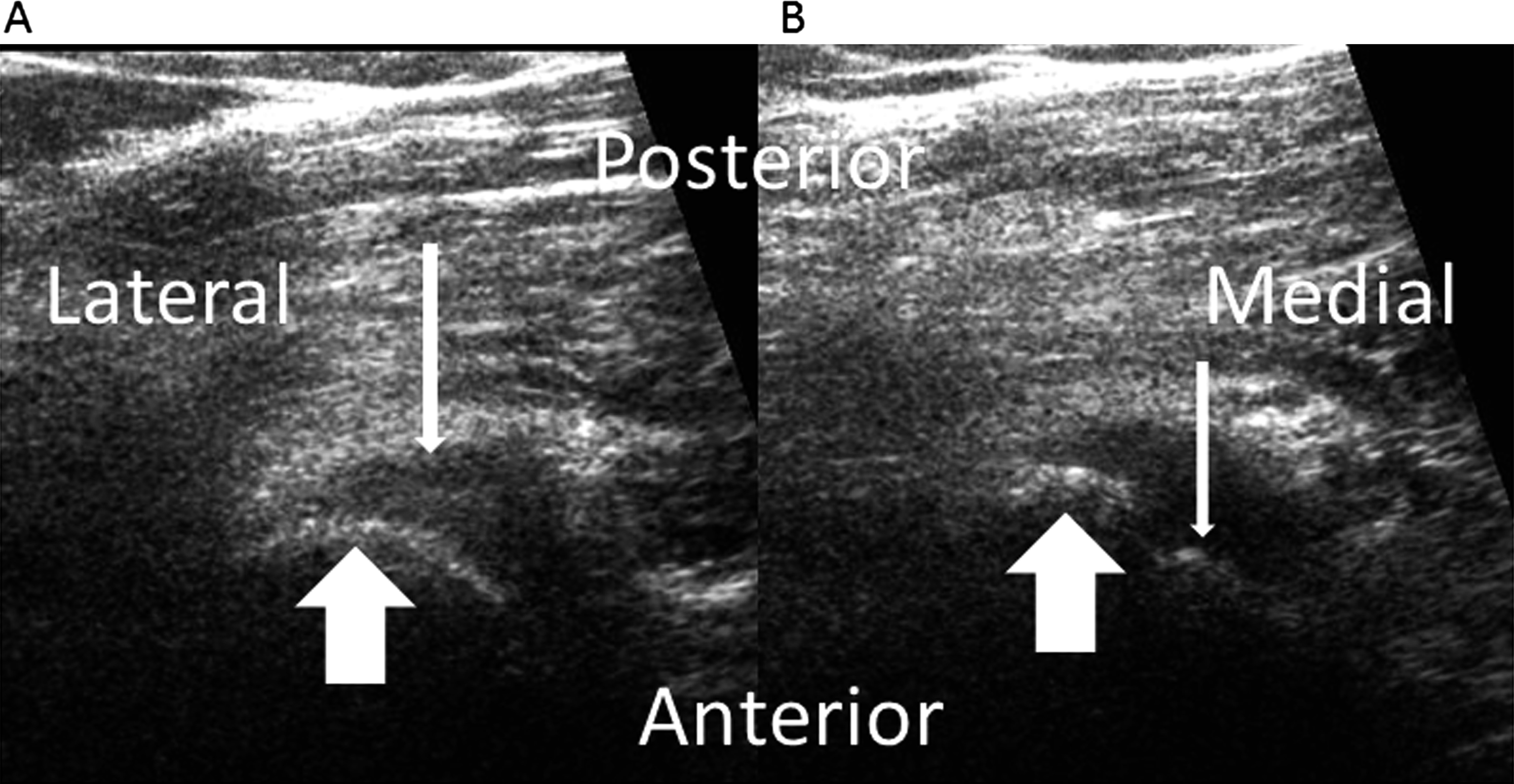
Fig. 3A fifty-five-year-old female recreational tennis player presented with a one-year history of left buttock pain as well as audible snapping in the buttock when she bent at the hips. The symptoms began approximately one month after she sustained a hamstring strain while playing tennis. Because of the pain, she had been unable to return to athletic activities. Physical examination revealed tenderness at the hamstring origin. Full motion of the hips, knees, and back was present with no contractures. The patient reproduced the snapping with hip flexion of approximately 90° while she was in the standing position. The snapping was palpable at the ischial tuberosity and was audible. Pelvic radiographs showed no abnormalities. Magnetic resonance imaging (MRI) demonstrated a partial tear of the proximal hamstring origin with surrounding edema (Fig. 1). While the patient performed the provocative maneuver, dynamic ultrasound with the probe on the ischial tuberosity demonstrated subluxation of a portion of the proximal hamstring origin over the tuberosity (Fig. 2). The patient underwent physical therapy for hamstring stretching and strengthening for six weeks, but the symptoms persisted. A cortisone injection was then administered over the area of maximal tenderness. The symptoms remained unchanged for several weeks after the injection. A second six-week course of physical therapy was prescribed, but, once again, the symptoms failed to improve. Without resolution of the painful snapping, the patient no longer desired to continue conservative treatment.
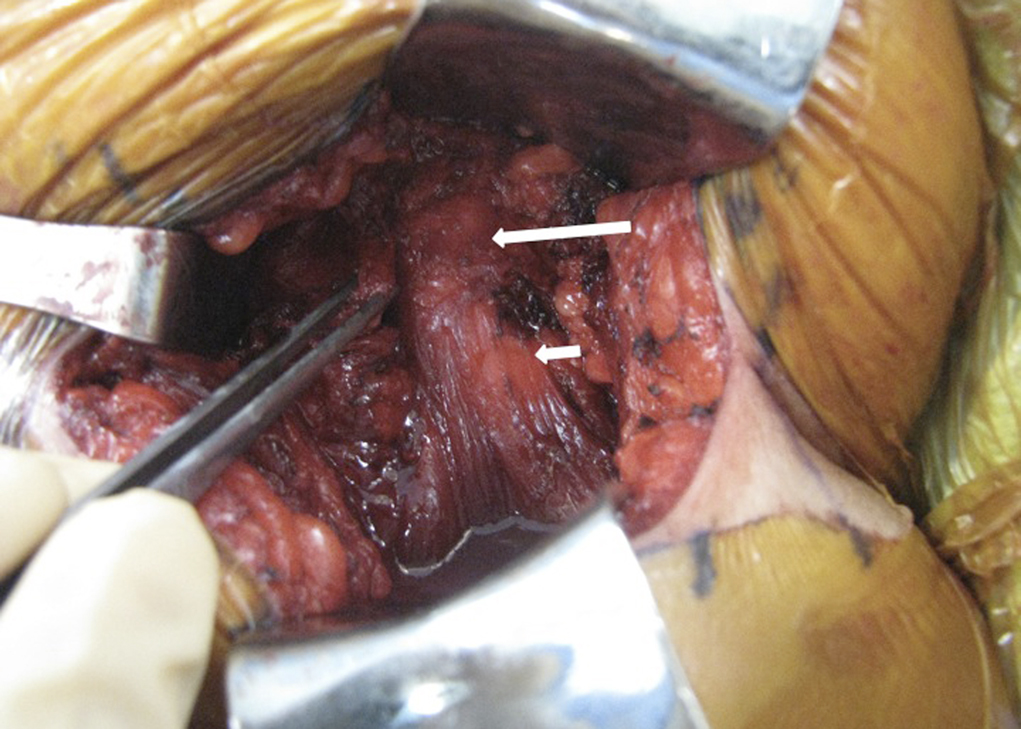
A limited tenotomy of the lateral portion of the proximal semimembranosus origin was performed. The patient was placed in the prone position, with the entire left lower extremity draped free and with the surgical table flexed at the hip to allow reproduction of the provocative position. The limited tenotomy was performed through a transverse incision in the gluteal fold centered over the ischial tuberosity. The gluteal fascia was incised transversely, and the gluteus maximus muscle was split bluntly. The sciatic nerve was identified and was protected with a retractor throughout the procedure. The hamstring fascial sheath was identified and split longitudinally; an elongated partial tear, comprising 25% of the semimembranosus muscle origin, was noted. Snapping of this elongated tendon tear over the ischial tuberosity was recreated intraoperatively with hip flexion (Fig. 3). A tenotomy was performed on the elongated, partially torn tendon. This tendon was released directly from the ischial tuberosity, and the remainder of the origin of the hamstrings was spared. Postoperatively, the patient was permitted weight-bearing as tolerated. Passive and active hip motion was started immediately after surgery without any limitation. Strengthening was started three weeks postoperatively. The patient was free of painful snapping after the tenotomy. She returned to athletic activity three months postoperatively without appreciable hamstring pain or weakness. Nine months after surgery, the patient remained pain-free and no longer experienced hip snapping; she played tennis without limitation.
Proceed to Discussion >>Reference: Scillia A, Choo A, Milman E, McInerney V, Festa A. Snapping of the proximal hamstring origin: a rare cause of coxa saltans. A case report. J Bone Joint Surg Am. 2011;93:e125. doi:10.2106/JBJS.J.01622
While the "snapping hip" is a commonly recognized entity, rarely is subluxation of the proximal origin of the hamstrings over the ischial tuberosity considered in the differential diagnosis. A snapping hip is suspected to be due to subluxation of the proximal hamstring origin over the ischial tuberosity when there is a history of audible snapping and pain in the area of the buttock rather than in the anterior aspect of the groin or the lateral portion of the hip. During physical examination, the subluxation of the tendon can be palpated as the patient fully flexes the abducted hip in the standing position. The hamstring tendons originate on the ischial tuberosity with a common tendon for the biceps femoris and semitendinosus muscles. This common tendon has an oval-shaped insertion, averaging 2.7 × 1.8 cm3, medial to the semimembranosus muscle. The insertion of the semimembranosus muscle is lateral to the common origin of the biceps femoris and semitendinosus muscles. It is crescent-shaped and has an average size of 2.1 × 1.1 cm3. During the operative treatment of our patient, the pathology was located on the lateral portion of the origin, and the fibers were contributions from the semimembranosus muscle. However, at this level, the subluxating fibers could not be tracked definitively to a single muscle belly. Radiographs did not show any pathology in our patient. MRI demonstrated nonspecific changes at the ischial tuberosity consistent with tendinopathy and a partial tear of the lateral portion of the hamstring origin. The utility of MRI is restricted with this diagnosis because of limitations with patient positioning in the MRI scanner. The provocative position is not feasible within the MRI machine, nor is dynamic imaging available with this modality. We believe that dynamic ultrasound is the optimal study for the "snapping hip" caused by subluxation of the proximal hamstring origin at the ischial tuberosity. To our knowledge, there are no data on the treatment of the "snapping hip" due to subluxation of the proximal hamstring origin except in one case report. Conservative treatment of this condition is the same as the treatment of a high hamstring strain, and includes rest, ice, nonsteroidal anti-inflammatory drugs (NSAIDs), and physical therapy. If pain and snapping resolve with these conservative methods, a progressive return to sports with adjuvant low-intensity jogging and cycling can be considered. Cohen and Bradley stated that athletes are able to return to sports after a single hamstring tendon avulsion with retraction up to 2 cm. The indications for operative treatment of this condition are not established. Our rationale for the operative procedure that we performed was based on the integrity of the tendon origin on the ischial tuberosity. While clear indications for repair of tears of the hamstring origin are debatable, we utilized those set forth by Cohen and Bradley, in which repair is indicated for a proximal hamstring avulsion involving two or more tendons with >2 cm of retraction in a patient who is less than fifty years of age and who desires to continue athletic participation. Based on the nature of this condition, we suspect that it would be improbable to have a completely torn and retracted tendon and, therefore, repair is unlikely to be indicated. It is more plausible that the "snapping hip" resulting from subluxation of the proximal hamstring origin would be caused by tendinopathy or an elongated or partially torn tendon, similar to what was noted in our patient. Surgical options include partial tenotomy or partial tenotomy with transfer. Athletes with proximal hamstring tendinopathy have been treated with tenotomy of the semimembranosus muscle with suture repair to the biceps femoris muscle with good functional outcomes. We did not choose this procedure because our patient was fifty-five years old, was not a high-level athlete, and had only a small tear of the lateral portion of the hamstring origin that was responsible for the painful snapping. As demonstrated in this case report, partial release of the subluxating semimembranosus tendon from the ischial tuberosity resulted in resolution of the pain and the snapping.
Reference: Scillia A, Choo A, Milman E, McInerney V, Festa A. Snapping of the proximal hamstring origin: a rare cause of coxa saltans. A case report. J Bone Joint Surg Am. 2011;93:e125. doi:10.2106/JBJS.J.01622
Tenotomy of the semimembranosus tendon
Resection of the lateral portion of the ischial tuberosity
Open repair of the semimembranosus tear
Transfer of semimembranosus origin laterally on the ischial tuberosity