A Fifty-seven-Year-Old Man with Acute Pain Following Hip Arthroplasty
October 16, 2013
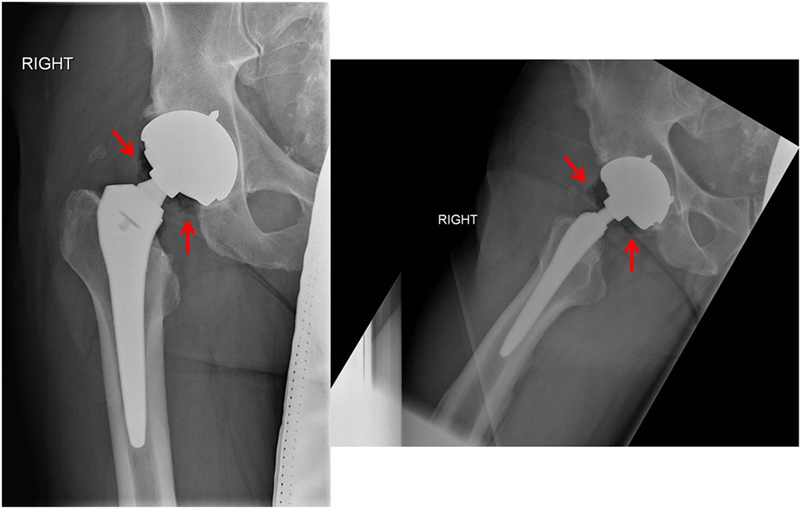
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5An otherwise healthy fifty-seven year-old man with a body mass index (BMI) of 31 kg/m2 underwent index right total hip arthroplasty for end-stage hip arthrosis. Through an anterolateral approach, he received a size-5 PROFEMUR Z femoral stem, a 58-mm CONSERVE nonmodular acetabular component, a plus-0 short varus neck, and a 52-mm cobalt-chromium head (all components from Wright Medical Technology, Arlington, Tennessee). This component combination includes a metal-on-metal articulation and an oval-tapered modular neck distally, which allows insertion into the femoral stem at a fixed angle. The femoral stem and modular neck are both manufactured from a titanium alloy (Ti-6Al-4V). The alignment of the prosthesis was confirmed immediately postoperatively and at each subsequent clinic visit. The postoperative course was unremarkable, and the patient was walking without pain within ninety days. At twenty-eight months following the index procedure, the patient, over the course of dinner, began to develop groin and buttock pain. Unable to stand or bear weight on the affected side, he immediately presented to our emergency department. The hip examination was limited secondary to pain; however, any movement caused irritability. Radiographs demonstrated well-aligned components, with no overt hardware failure; there was a distinct collection of gas within the hip joint (Fig. 1). Laboratory values did not suggest infection: the erythrocyte sedimentation rate (ESR) was 6 mm/h (normal, 0 to 9 mm/h) and the C-reactive protein (CRP) level was 1.1 mg/dL (normal, 0 to 1 mg/dL).
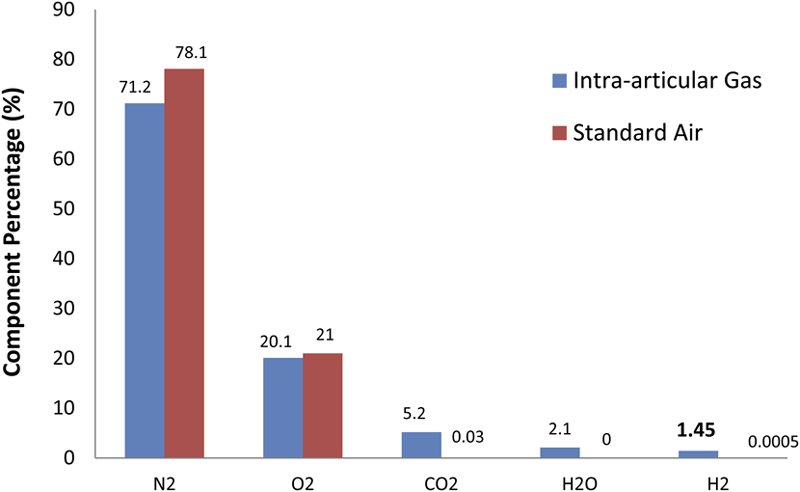
Under fluoroscopic guidance, two distinct samples (one of intra-articular gas and a second of joint fluid) were aspirated from the right hip joint. Upon penetration of the joint capsule with the spinal needle, the patient experienced a tremendous pang of pain, which quickly resolved and steadily progressed to almost complete pain resolution within minutes of removal of the gas sample. Synovial fluid was not suggestive of infection based on cell count (5000 red blood cells per mm3, 3000 white blood cells per mm3 marked as inaccurate secondary to white blood-cell lysis), cell differential (96% histiocytes, 2% neutrophils, 2% lymphocytes), and negative culture results; lack of infection was confirmed via a negative polymerase chain reaction assay for bacterial DNA. The intra-articular gas sample was analyzed with use of a custom-built mass spectrometer (HPR-20; Hiden Analytical, Warrington, United Kingdom). Time-dependent intensities for each gas species were plotted, and it was noted that their peaks integrated to derive a species-specific concentration. The concentration of each gas species was recorded and compared with a sample of standard air (Fig. 2). The patient returned to clinic two weeks later with marked improvements in the ability to bear weight and walk. However, because the serum titanium level was elevated at 61 ng/mL, the modular neck was revised three weeks following the initial presentation. An anterolateral approach and the modular neck extraction device were used. The freeing blow of the slap hammer resulted in a loud explosion and a cloud of pungent smoke. Visual inspection of the femoral neck demonstrated hallmark signs of corrosion, including debris and pitting (Fig. 3). Microscopic inspection of the adjacent capsular tissue revealed dense fibroadipose and vascular tissue with chronic inflammation; the aseptic lymphocytic vasculitis-associated lesions score was 7. Twenty months after revision surgery, the titanium level had decreased to 37 ng/mL and the patient was doing well clinically.
Proceed to Discussion >>Reference: Weber AE, Skendzel JG, Waxman DL, Blaha JD. Symptomatic aseptic hydrogen pneumarthrosis as a sign of crevice corrosion following total hip arthroplasty with a modular neck: a case report. JBJS Case Connector. 2013 Jul 24;3(3):e76.
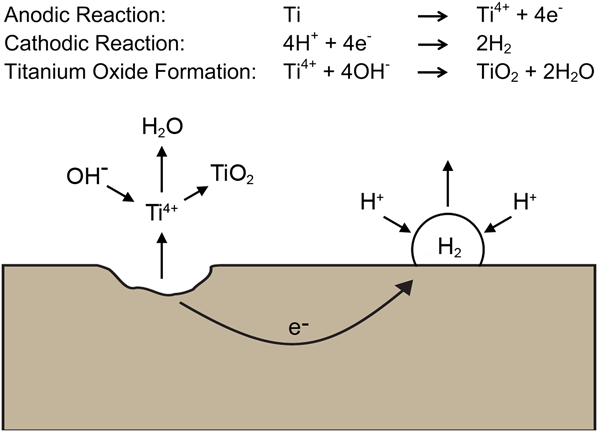
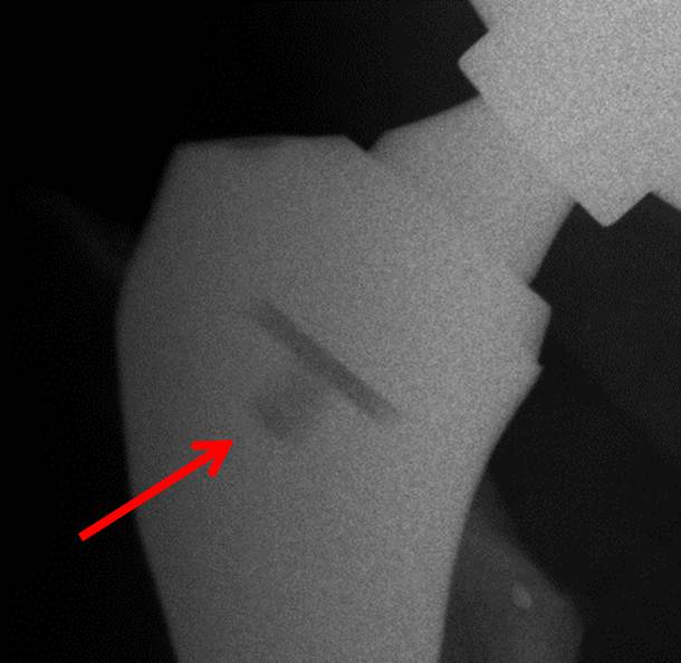
Modularity of the femoral neck in total hip arthroplasty affords the surgeon options for augmenting version and offset once the femoral stem has been implanted. These options become advantageous in difficult primary arthroplasty and in revision when the stem is not in an ideal position. These advantages may be negated by the increasing number of clinical reports of modular neck complications or failure; numerous in vitro and retrieval studies assist in understanding the underlying mechanisms that lead to clinical failure. Some studies have identified asymmetric mechanical loading of the modular neck as a cause of increased stress and ultimate failure. Other studies, focused on the biochemical environment of the Ti/Ti neck-stem interface, have demonstrated that this interface undergoes crevice corrosion in the presence of micromotion. The process of corrosion starts with the combination of micromotion abrading the stable external oxide layer on the implant while, simultaneously, joint fluid occupies the defect created by the micromotion. Once the stable oxide layer is removed, the freshly exposed titanium alloy reacts with the joint fluid (mainly the water component) to form an oxide and then release hydrogen ions into solution (Fig. 4). With successive loading cycles, the process repeats itself, leading to the propagation of corrosion and the sequelae thereof, including pitting, cracking, and ultimately implant failure. This sequential process may be initiated or exacerbated in the presence of contamination during the assembly of components or because of inadequate impaction of the components. We contend that this process of crevice corrosion may have occurred at the modular neck-stem interface in our six patients. One by-product of crevice corrosion is diatomic hydrogen gas (Fig. 4), which likely accumulates in the small reservoir found in the distal aspect of the neck-stem interface (Fig. 5) until a path is created for its release, either by continued micromotion or crevice corrosion. Once the gas is released, the joint capsule is suddenly subjected to an increase in pressure, resulting in the acute onset of pain. This process would also explain the radiographic evidence of pneumarthrosis in the absence of infection with a gas-producing organism. The loud explosions heard at the time of the removal of the neck from the stem in two of our patients were likely caused by acute depressurization of the hydrogen gas.
Reference: Weber AE, Skendzel JG, Waxman DL, Blaha JD. Symptomatic aseptic hydrogen pneumarthrosis as a sign of crevice corrosion following total hip arthroplasty with a modular neck: a case report. JBJS Case Connector. 2013 Jul 24;3(3):e76.

Clostridium infection in hip
Intra-articular fretting corrosion
Titanium metallosis
Aseptic hydrogen pneumarthrosis