

 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 6
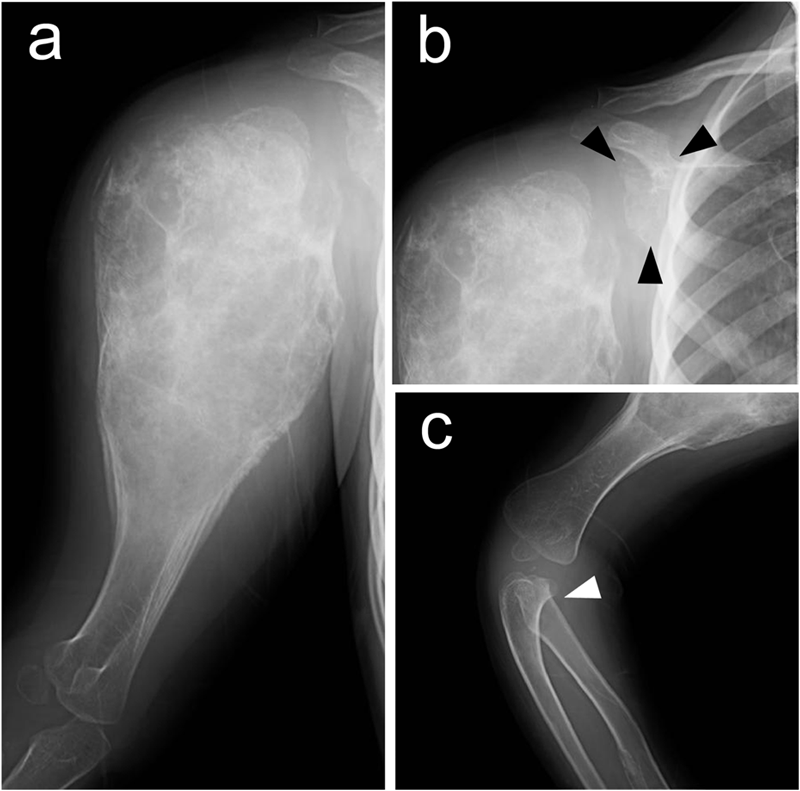
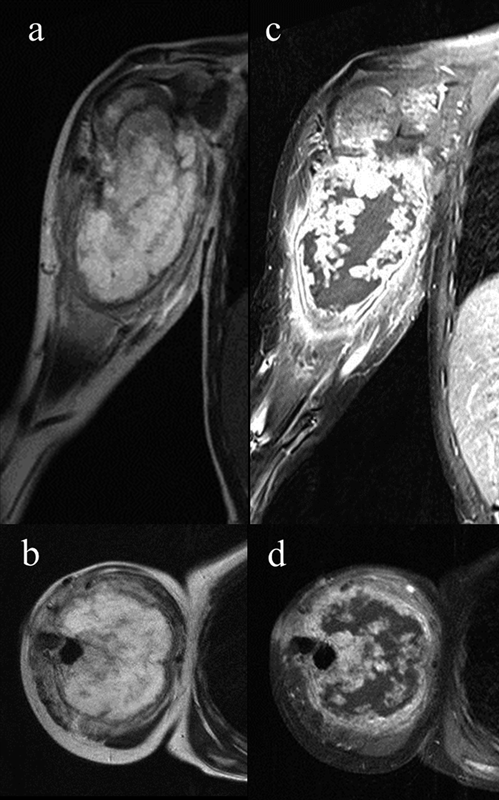
Fig. 6A four-year-old boy was brought to a local hospital with a one-week history of right shoulder pain. He had no contributory medical or family history. Radiographs revealed a geographic, mildly expansile, lytic lesion with mild cortical thinning and slight intratumoral calcification in the proximal part of the right humerus (Figs. 1-A and 1-B). Computed tomography (CT) demonstrated multiple additional bone lesions in locations other than the humerus, including the right scapula and radius, with a unilateral distribution. A sample obtained from the humeral lesion by needle biopsy via a transdeltoid approach was diagnosed as enchondroma at another hospital. Periodic medical examinations were performed; six months after the biopsy, the tumor started to show a rapid increase in size. The patient was referred for additional evaluation and management. On physical examination, an osseous hard mass was palpable over the entire circumference of the proximal part of the right humerus, and local tenderness was evident. Flexion and abduction of the right shoulder were minimally limited (160° and 150°, respectively). Radiographs showed an expansile lytic lesion in the proximal part of the right humerus with thinning of the cortex and intratumoral calcification (Fig. 2-A). Tumor growth, especially in the proximal portion, was evident on the radiographs that were taken six months after the needle biopsy. Areas of endosteal lysis were also found in the right scapula and radius (Figs. 2-B and 2-C). Magnetic resonance imaging (MRI) demonstrated a lobulated lesion of the proximal part of the right humerus, with intermediate signal intensity relative to skeletal muscle on T1-weighted images, and heterogeneous high signal intensity on T2-weighted images (Figs. 3-A and 3-B), consistent with chondroid matrix. No extraosseous extension was noted. The lesion showed intense septal and peripheral rimlike contrast enhancement after intravenous administration of contrast medium (gadolinium-diethylenetriamine pentaacetic acid) (Figs. 3-C and 3-D). A bone scan showed increased accumulation of the radioisotope in the humeral lesion (Fig. 4), but no remarkable accumulation was observed in the scapula or radius, as had been demonstrated on the radiographs (Figs. 2-B and 2-C). The increased size of the lesion and the appearance of a lytic area with cortical destruction that was associated with pain prompted us to perform an open biopsy. A transdeltoid approach through the anterior third of the muscle was used to minimize the resection of other muscles and contamination of the main neurovascular bundle of the upper extremity. Pathologic examination showed multinodular growth of hyaline cartilage separated by thin fibrous bands. The chondrocytes were atypical, varying in size and shape, and they contained enlarged hyperchromatic nuclei. There were several areas where the tumor closely intermixed with lamellar bone, suggestive of permeative growth.
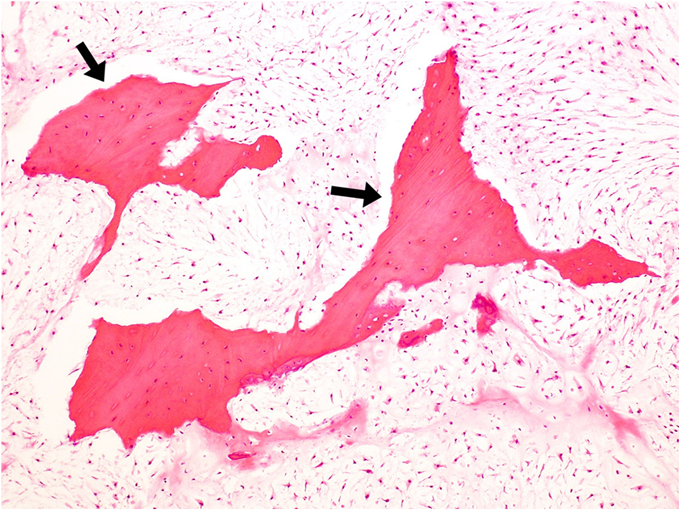
The overall findings, together with radiographic and clinical data, suggested a likely diagnosis of secondary chondrosarcoma. On the basis of the histological interpretation, we performed a wide resection of the tumor and reconstruction with use of a free vascularized fibular graft as a functional spacer, as well as a sling procedure to preserve scapulohumeral passive movement. The distal end of the fibula was fixed to the proximal stump of the humerus with screws, and the head of the fibula was inserted slinglike through the acromion with the tendons of the biceps femoris muscle (Fig. 5-A). The peroneal artery and vein were anastomosed to the deep brachial artery and vein, respectively. Histological examination of the resected specimen revealed features similar to those of the open biopsy, but in addition, substantial myxoid change and unequivocal permeative growth with entrapment of the preexisting lamellar bone were evident (Fig. 6). Thus, the diagnosis of low-grade secondary chondrosarcoma arising in a patient with Ollier disease was confirmed. The resection margin was free of tumor. The postoperative course was uneventful, and no local recurrence or metastasis was evident five years postoperatively. The bone graft was well incorporated, and there was no dislocation of the fibular head (Figs. 5-B and 5-C). Although there was limitation of lifting ability and range of motion, the patient had no pain and he was able to participate in recreational swimming. The International Society of Limb Salvage/Musculoskeletal Tumor Society score was 73%.
Proceed to Discussion >>Reference: Ogura K, Takeda K, Fujiwara T, Yoshida A, Chuman H, Kawai A. Secondary chondrosarcoma of the proximal part of the humerus arising in a four-year-old boy with Ollier disease: a case report. JBJS Case Connector. 2013 Dec 24;3(4):e131 1-6.
Secondary chondrosarcoma is a distinctive type of chondrosarcoma that originates from a preexisting benign chondroid lesion. It has a male predilection (male-female ratio of 2:1); the most common sites of involvement are the pelvis and the proximal part of the femur, followed by the scapula and the proximal part of the humerus. Secondary chondrosarcomas are most commonly associated with solitary or multiple osteochondromas, which constitute 88% of secondary chondrosarcomas. Only a fraction of cases arise from other conditions, including solitary enchondroma, synovial chondromatosis, Ollier disease, or Maffucci syndrome. Although malignant transformation in patients with Ollier disease is well recognized, little information regarding the true incidence of secondary chondrosarcomas in Ollier disease is available because of the rarity of the condition. Previous reports have suggested that the rate of malignant transformation is ten to fifteenfold higher in patients with Ollier disease or Maffucci syndrome compared with solitary enchondroma or osteochondroma. In the largest reported series of enchondromatosis, four of thirty-seven patients (mean age at diagnosis, three years; range at diagnosis, infancy to fourteen years) with Ollier disease developed chondrosarcoma at a mean age of twenty-eight years (range, eighteen to forty-three years); four of seven patients (mean age at diagnosis, three years; range at diagnosis, one to five years) with Maffucci syndrome developed chondrosarcoma at a mean age of thirty-five years (range, sixteen to fifty-eight years). In these reports, the mean age at diagnosis of malignant transformation was thirty-four years, which is younger than the age of patients with primary chondrosarcoma. In a series from the Mayo Clinic, approximately 60% of patients with secondary chondrosarcoma were in their third or fourth decade of life, while only 4.8% were in their second decade. No patients with secondary chondrosarcoma were in their first decade of life. Additionally, in a series by the Armed Forces Institute of Pathology, no patients with secondary chondrosarcoma were less than ten years of age. Histological differentiation between enchondroma and low-grade chondrosarcoma is sometimes difficult because malignant features may be present only in limited areas of the tumor. Furthermore, in cases of secondary chondrosarcoma arising through transformation from enchondroma, including Ollier disease, lack of unequivocal biopsy evidence may be a problem. Although good quality imaging is useful for demonstrating suspicious features such as endosteal erosion and cortical buttressing, biopsy is often needed to demonstrate tumor permeation through preexisting bone, which is important for differentiation between enchondroma and chondrosarcoma. Needle biopsy has an inherent limitation for tumor sampling. In addition to histological analysis for adequate tumor samples, radiographic and clinical symptoms, such as a rapid increase in size or pain, should be taken into account when differentiating chondrosarcoma from enchondroma.
Reference: Ogura K, Takeda K, Fujiwara T, Yoshida A, Chuman H, Kawai A. Secondary chondrosarcoma of the proximal part of the humerus arising in a four-year-old boy with Ollier disease: a case report. JBJS Case Connector. 2013 Dec 24;3(4):e131 1-6.

Aneurysmal bone cyst
Enchondroma
Dedifferentiated simple bone cyst
Metaphyseal osteomyelitis
Secondary chondrosarcoma