A Ninety-one-Year-Old Man with Pain, Tenderness, and Swelling in the Right Foot
April 16, 2014


 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
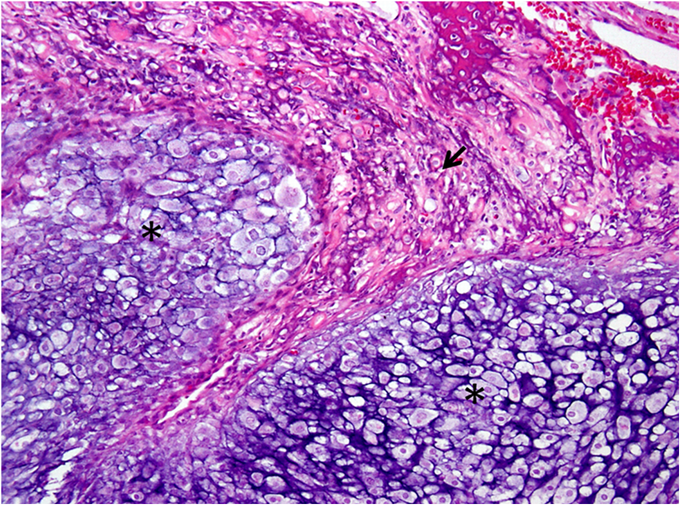
Fig. 3 Fig. 4
Fig. 4A ninety-one-year-old man presented with a six-month history of pain, tenderness, and swelling in the right foot, as well as increasing difficulty with walking. He denied recollection of any trauma or antecedent event. Initially evaluated by a community podiatrist six months previously, the foot pain was attributed to peripheral vascular disease with diabetic neuropathy. Three months later, maceration in the second and third web spaces of the foot had increased, but was attributed to hammer-toe deformities. At that time, podiatric examination confirmed full motor strength and minimal toe range of motion. After one additional month, pain, swelling, and erythema of the third toe increased, and a low-purine diet was initiated for suspected gout. Within three weeks, a 3 × 3 cm swelling at the base of the third toe had become evident, with increased erythema and tenderness as well as minimal range of motion and markedly diminished motor strength in the affected toe. The patient was referred for radiographs and magnetic resonance imaging (MRI), with subsequent consultation of an orthopaedic oncologist. At the time of referral, the patient had recently initiated use of a rolling walker for support while walking because of pain, which he described as a combination of sharp pain and tenderness with pressure, as well as burning pain with paresthesias. Because of opioid sensitivity, the patient was given naproxen for pain and gabapentin for paresthesias. He reported a maximal pain score of 6 on a 10-point visual analog scale, and stated that he experienced maximal pain with full weight-bearing on the right foot. The history was noteworthy for coronary artery disease, hypertension, non-insulin-dependent diabetes mellitus, chronic hematuria, osteoarthritis, asthma, and benign prostatic hypertrophy, for which he had undergone a transurethral resection of the prostate. He reported a twenty-seven pack-year history of cigarette smoking, but had stopped smoking thirty-nine years earlier. There was no prior patient or family history of malignancy. Upon presentation at our center, gross swelling of the right forefoot measured 3 × 3 cm and was centered at the base of the third phalanx, with a tender nonmobile nodule that was palpable on the dorsal surface. Erythema of the right second and third toes extended proximally toward the metatarsals. The dorsalis pedis pulse was nonpalpable on the right lower extremity, but a posterior tibialis pulse was evident bilaterally with brisk capillary refill. Sensation to light touch was mildly diminished in both feet, but present in all nerve distributions. Pitting edema of the right lower extremity was present, extending proximally to the midcalf level. No lymphadenopathy was identified. Laboratory results included a normal white blood-cell count, hemoglobin, hematocrit, platelet count, and alkaline phosphatase. Glucose levels were elevated at 119 mg/dL, and the glycosylated hemoglobin was elevated at a level of 6. Serum alkaline phosphatase measured 79 U/L. All other values were within normal limits. Initial radiographs showed a 7 mm lytic focus within the proximal aspect of the third proximal phalanx, without cortical disruption or soft-tissue extension. Upon presentation to our center, subsequent radiographs revealed lytic, permeative changes involving the proximal phalanx of the third digit, with an associated extraosseous soft-tissue mass abutting the adjacent digits (Figs. 1-A and 1-B). A subtle periosteal reaction along the lateral cortical margin was also evident, with a lateral focal cortical breach extending to the proximal interphalangeal joint. Subtle pressure erosions of the lateral aspects of the second and third metatarsal heads suggested possible tumor infiltration. MRI with gadolinium contrast revealed a 2.9 × 2.4 × 2.7 cm septated mass of the proximal phalanx of the third toe, in which the normal marrow signal was entirely replaced by tumor (Figs. 2-A through 2-D).
Cytologic analysis of a fine-needle aspirate demonstrated neoplastic cells with chondromyxoid features. Fluorescence in situ hybridization analysis showed no rearrangement of the Ewing sarcoma EWSR1 gene (22q12) in interphase cells, ruling out extraskeletal myxoid chondrosarcoma. Preoperative radiographic staging showed no metastases. Given the underlying diabetes and advanced age, a transmetatarsal amputation with a wide resection margin was performed. Wound edges were closed primarily. The postoperative course was uneventful. Grossly, the pathologic specimen demonstrated a 4.4 × 3.7 × 2.8 cm soft, gelatinous, and partly cystic mass that involved the proximal and middle phalanges of the third toe with a substantial soft-tissue component. Bone, skin, and soft-tissue margins were macroscopically negative. There was no gross involvement of the phalanges and metatarsals of the second and fourth toes (Fig. 3). Histopathologic analysis showed a dedifferentiated chondrosarcoma arising from a Grade-II chondrosarcoma with predominantly myxoid features. The spindle-cell component showed differentiation toward osteogenic sarcoma, and comprised approximately 5% of the primary tumor mass (Fig. 4). The tumor was associated with a soft-tissue extension involving the dermis. Microscopic margins were negative. The tumor was classified as Stage IIA according to the staging system of the American Joint Committee on Cancer. The patient was followed regularly in clinic for fifty-five months and recovered well, with no clinical or radiographic signs of recurrence or metastasis. No chemotherapy or radiation was given. At the most recent follow-up, he required no orthosis or assistive device for walking, reported no pain, and had a Musculoskeletal Tumor Society functional score of 24 of a possible 30.
Proceed to Discussion >>Reference: Levin A, Morris CD. Acral dedifferentiated chondrosarcoma of a toe phalanx: a case report. JBJS Case Connector. 2014 Feb 12;4(1):e16 1-5.
Dedifferentiated chondrosarcoma, initially described as well-differentiated chondrosarcoma juxtaposed with areas of fibrosarcoma or osteogenic sarcoma, now includes tumors bearing both a low or intermediate-grade chondrosarcoma as well as a spindle-cell-sarcoma component. The most frequent histologic variants of the spindle-cell component are osteogenic sarcoma and malignant fibrous histiocytoma/undifferentiated pleomorphic sarcoma, although other subtypes have been well described. Debate continues regarding the prognostic importance of the histologic variant of the spindle-cell component, and current evidence remains equivocal. However, some analyses suggest that patients with a dedifferentiated chondrosarcoma demonstrating a low-grade spindle-cell component may have improved disease-free and overall survival. Our patient was ninety-one years old at the time of diagnosis. Although dedifferentiated chondrosarcoma is commonly diagnosed in the sixth or seventh decade, about 6% of patients present after eighty years of age; very few of the published cases report long-term survival. We are aware of only one other nonagenarian who survived longer than three years after a diagnosis of dedifferentiated chondrosarcoma. The most remarkable characteristic of this case is the tumor’s anatomic location. Previous case series indicate that 60% to 72% of dedifferentiated chondrosarcomas present in the appendicular skeleton, with only about 4% of these tumors found in acral sites. The single published report of dedifferentiated chondrosarcoma of the foot lacked specific anatomic, clinical, and pathologic details. To our knowledge, no other case of a dedifferentiated chondrosarcoma of the phalanx of the foot has been reported. Unlike other chondrosarcoma subtypes, appendicular location does not appear to confer a favorable prognosis for patients with localized dedifferentiated chondrosarcoma. Acral dedifferentiated chondrosarcoma occurs infrequently, and cases distal to the wrist or ankle are even more rare; therefore, conclusions cannot be drawn from the literature about whether such locations affect prognosis. A locally aggressive course with low metastatic potential has been documented among patients with conventional chondrosarcoma of the phalanges of the hand or foot, and evidence suggests improved disease-free survival in such patients, particularly when treated with amputation. In contrast, chondrosarcomas arising in the hindfoot tend to metastasize more frequently. Although the typical prognosis associated with dedifferentiated chondrosarcoma is dismal, with a median overall survival ranging from six to seventeen months, long-term survival is possible; five-year disease-free survival occurs in approximately 7% of patients. The factors that contribute to prolonged survival are unknown, but this case of dedifferentiated chondrosarcoma with an atypical location, advanced patient age, and postamputation survival of longer than four years provides details to augment our knowledge of the varied presentations and pathological features of this condition, and confirms the value of aggressive management.
Reference: Levin A, Morris CD. Acral dedifferentiated chondrosarcoma of a toe phalanx: a case report. JBJS Case Connector. 2014 Feb 12;4(1):e16 1-5.

Aneurysmal bone cyst
Dedifferentiated chondrosarcoma
Metastatic lung carcinoma
Osteogenic sarcoma
Metastatic prostate carcinoma