A Seven-Year-Old Girl with a Three-Week History of Pain in the Upper Arm without a History of Trauma
July 21, 2010
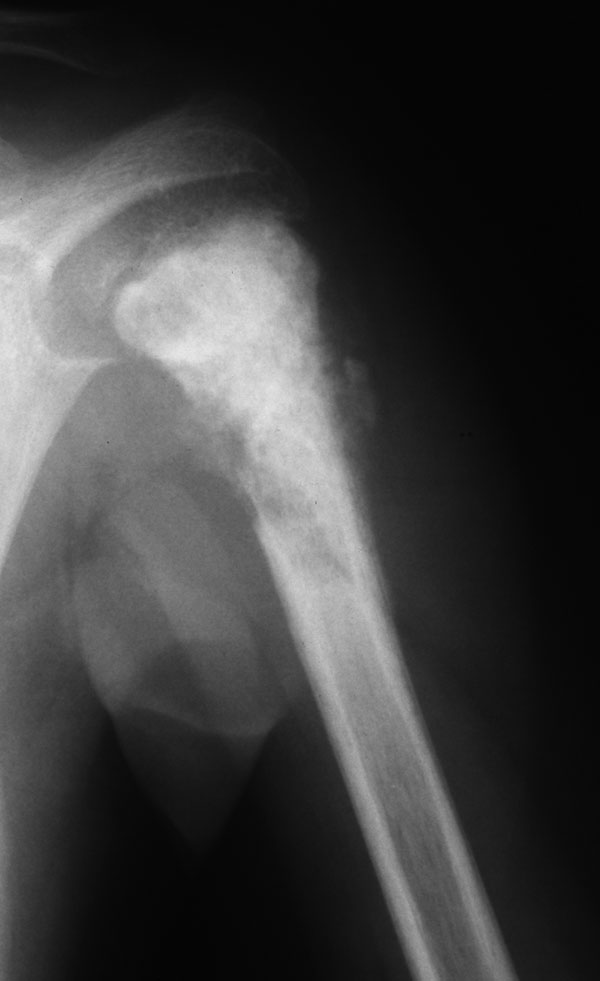
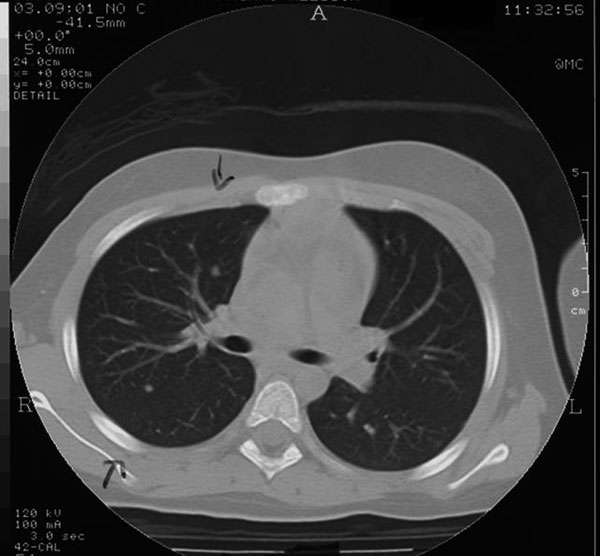

 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
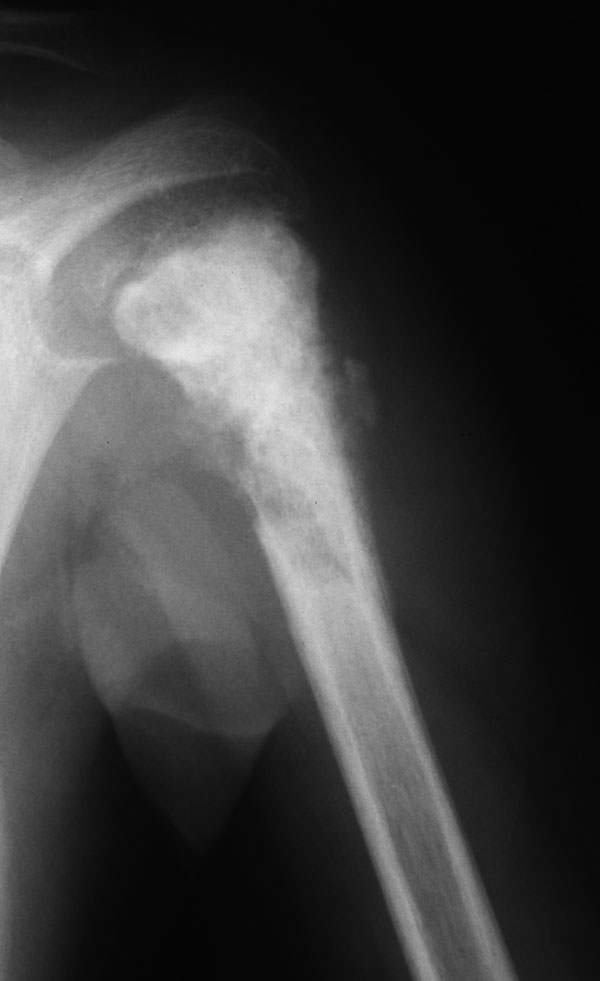
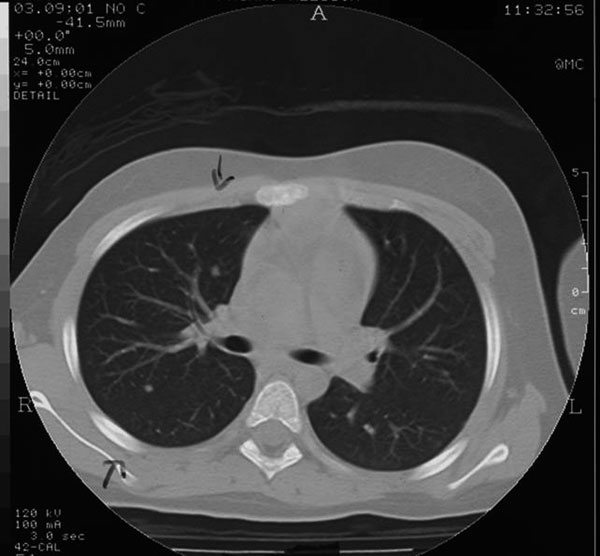
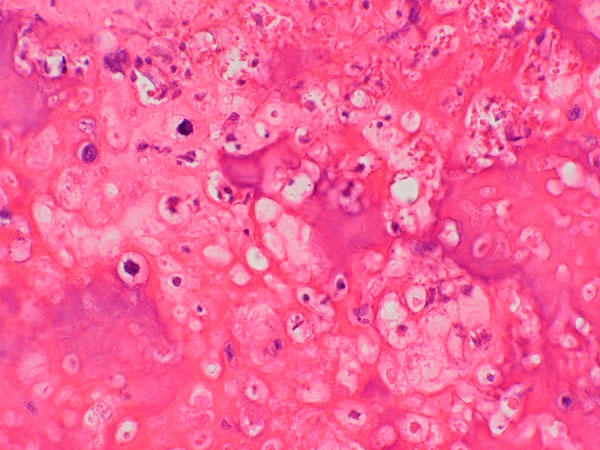
Fig. 3A seven-year-old girl was admitted to the hospital with a three-week history of pain in the left upper arm. Physical examination revealed a hard and tender swelling in the proximal part of the humerus. The only abnormal result of laboratory tests was a very high level of serum alkaline phosphatase (1600 U/L; normal values, 190-490 U/L). A radiograph is presented in Figure 1. The computed tomography scan and magnetic resonance imaging scan of the left upper arm confirmed the described aspects of the lesion. The staging was completed with a total-body technetium-99 bone scan and a computed tomography scan of the chest. The bone scan showed increased uptake in the proximal part of the left humerus, and the computed tomography scan of the chest showed ten pulmonary nodules with indistinct margins (Fig. 2). Three nodules were located in the left lung and seven nodules were located in the right lung. All nodules had diameters of between 0.2 cm and 0.35 cm. A core needle biopsy of the bone lesion was performed.
A core-needle biopsy of the bone lesion demonstrated a grade-4 osteoblastic osteosarcoma according to the carcinoma grading system of Broders et al. (Fig. 3). The patient underwent a nine-week preoperative chemotherapy regimen with high-dose methotrexate, Adriamycin (doxorubicin), and ifosfamide according to the Istituto Ortopedico Rizzoli/Osteosarcoma-4 (IOR/OS-4) protocol, as previously reported. After the preoperative treatment, the pain disappeared completely, the soft-tissue swelling decreased, and the serum alkaline phosphatase level returned to normal. At the end of the preoperative chemotherapy regimen, a radiograph of the left upper arm showed marked ossification of both the intramedullary and extraosseous components. A computed tomography scan of the upper arm confirmed these findings, showing almost complete ossification of the tumor. The lesions in the humerus and lungs remained unchanged over twelve years of follow-up.
Proceed to Discussion >>Reference: Palmerini E, Staals EL, Ferrari S, Rinaldi R, Alberghini M, Mercuri M, Bacci G. Nonresectable multiple lung metastases of high-grade osteosarcoma of the humerus: stable after twelve years. A case report. J Bone Joint Surg Am. 2008;90:2240-4.
Computed tomography scans of the chest are routinely performed in the diagnostic workup and follow-up of patients with osteosarcoma. Because of the high sensitivity and low specificity of computed tomography scans of the chest for the detection of lung lesions, false-positive results are frequent. It has been suggested that 25% of the lung nodules seen in new patients with osteosarcoma who present with between one and three lung nodules on the initial computed tomography scan of the chest turn out to be nonmetastatic on histological examination. Occasionally, patients with other types of cancer have shown stabilization of histologically proven pulmonary metastases for many years after adequate chemotherapy, and follow-up biopsies have shown necrosis without signs of viable tumor cells. These "sterilized" nodules are radiographically indistinguishable from residual viable tumor. It must be noted that in all previously reported cases of stable ("sterilized") metastatic lung nodules, the number of nodules has been small (from one to four). The case presented here is unique for two reasons: First, there were more than ten bilateral pulmonary nodules. Second, the histological examination of five of these, performed one year after the end of treatment, showed viable osteosarcoma cells in all nodules. Spontaneous regression of a single, biopsy-proven metastatic lesion of the lung from osteosarcoma has been previously reported, but, to our knowledge, this is the first description of a patient who had multiple bilateral metastatic lesions of the lung from osteosarcoma and in whom the condition was stable twelve years after the initial diagnosis. The spontaneous regression or stability of multiple metastatic malignant lesions as documented on computed tomography scans has been described in a wide variety of cancers but, to our knowledge, has not been described before in osteosarcoma. The reason for this stability is not clear. Stimulation of the cellular and/or humoral immune system, triggered for example by infections or surgery, may activate natural cytotoxic defenses. Cole and Everson observed that eight of 176 cases of spontaneous tumor regression reported in the literature were associated with infection. However, there were no signs of infection in the patient highlighted in this Image Quiz. Therefore we are not able to give any explanation of the uncommon outcome of this case to date. In a recent review on molecular mechanisms of metastasis, it was reported that metastasis suppressor genes have a role in controlling proliferation of cancer cells in a lung environment. Further studies on the mechanisms of the metastatic process may aid in the treatment of metastatic osteosarcoma and other malignant tumors.
Reference: Palmerini E, Staals EL, Ferrari S, Rinaldi R, Alberghini M, Mercuri M, Bacci G. Nonresectable multiple lung metastases of high-grade osteosarcoma of the humerus: stable after twelve years. A case report. J Bone Joint Surg Am. 2008;90:2240-4.
sclerosing osteomyelitis
osteoblastic osteosarcoma
Ewing sarcoma
leukemia