An 11-Year-Old Boy with a Gradually Swelling Knee
March 3, 2021
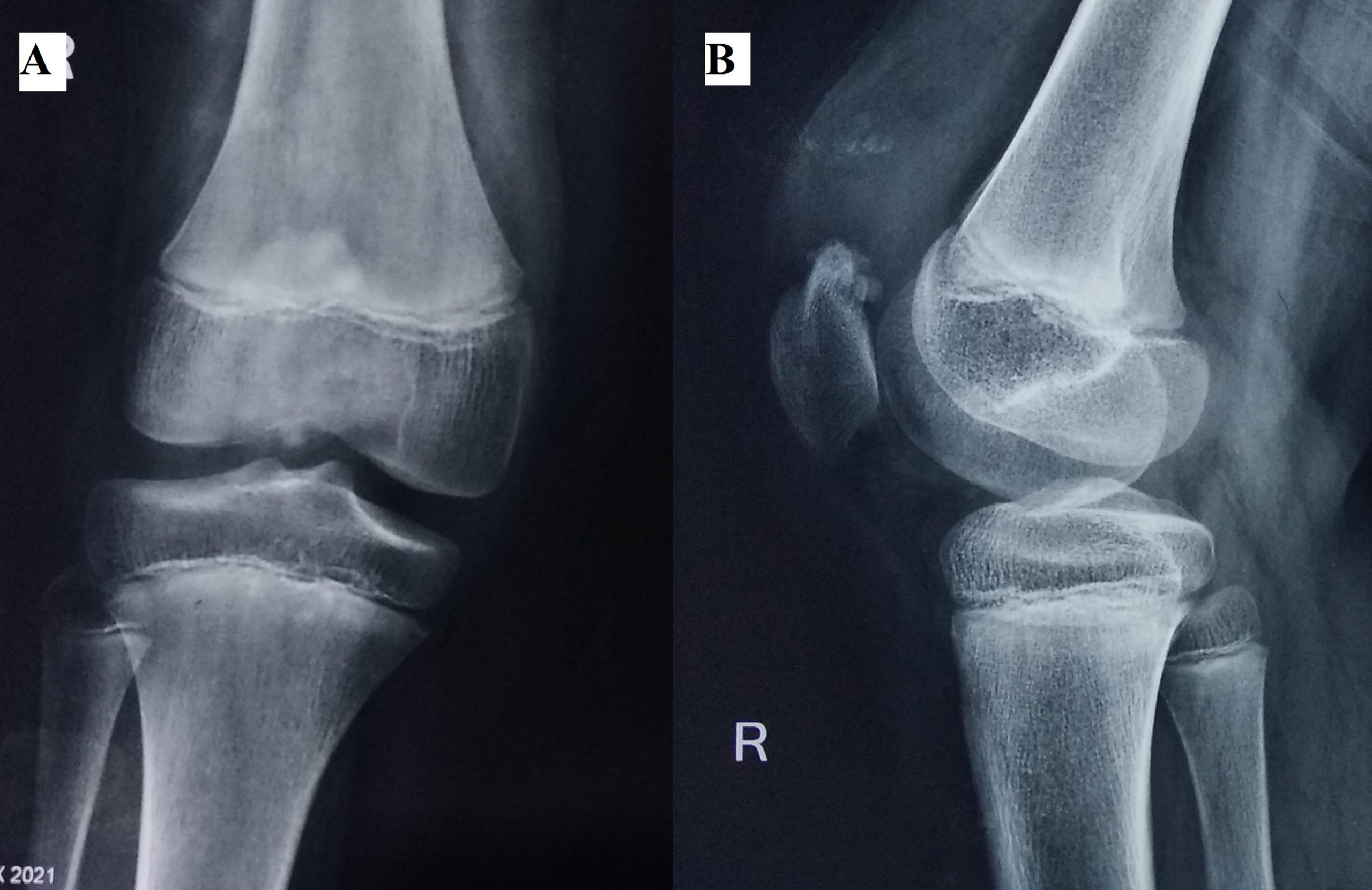
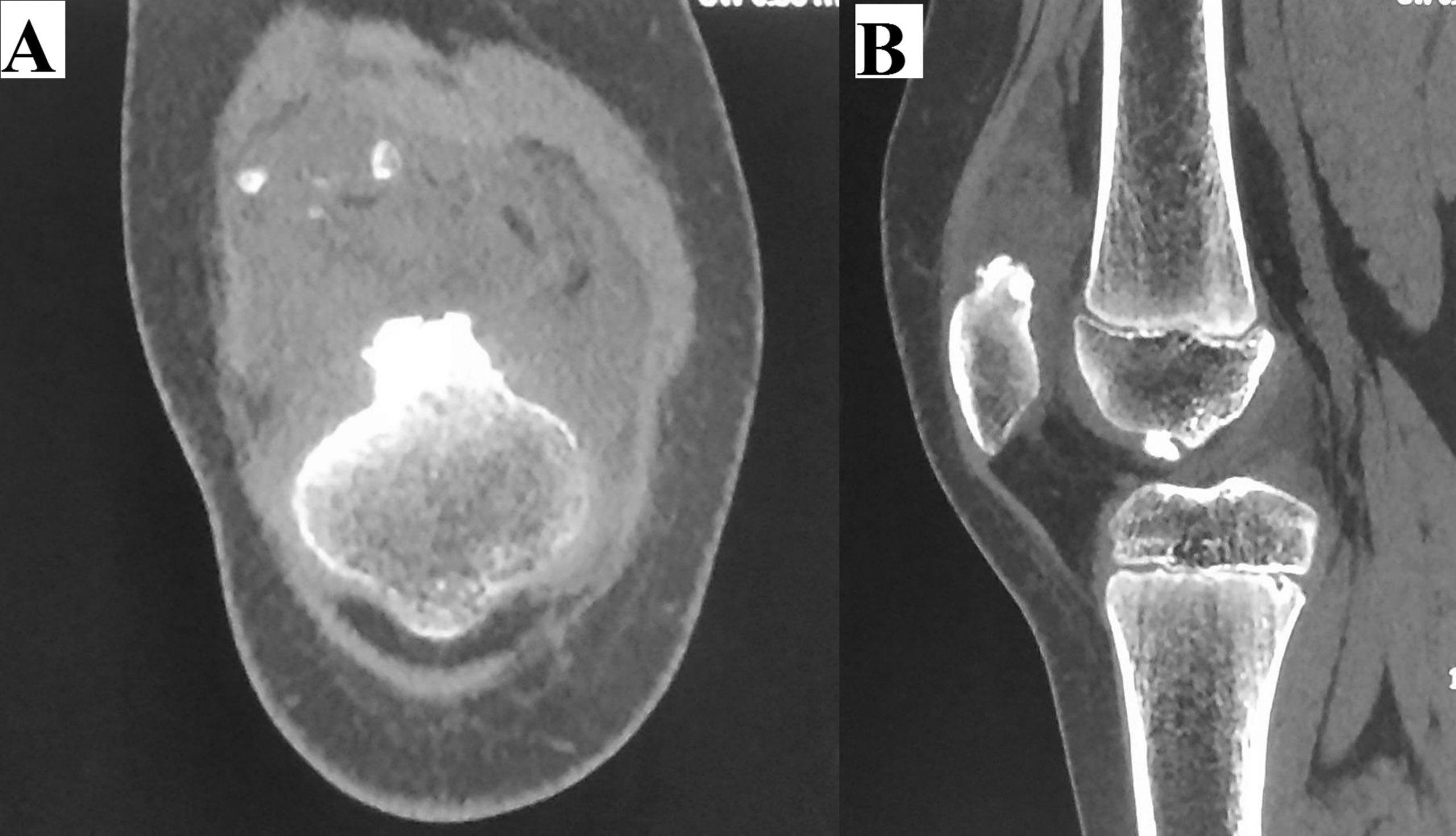
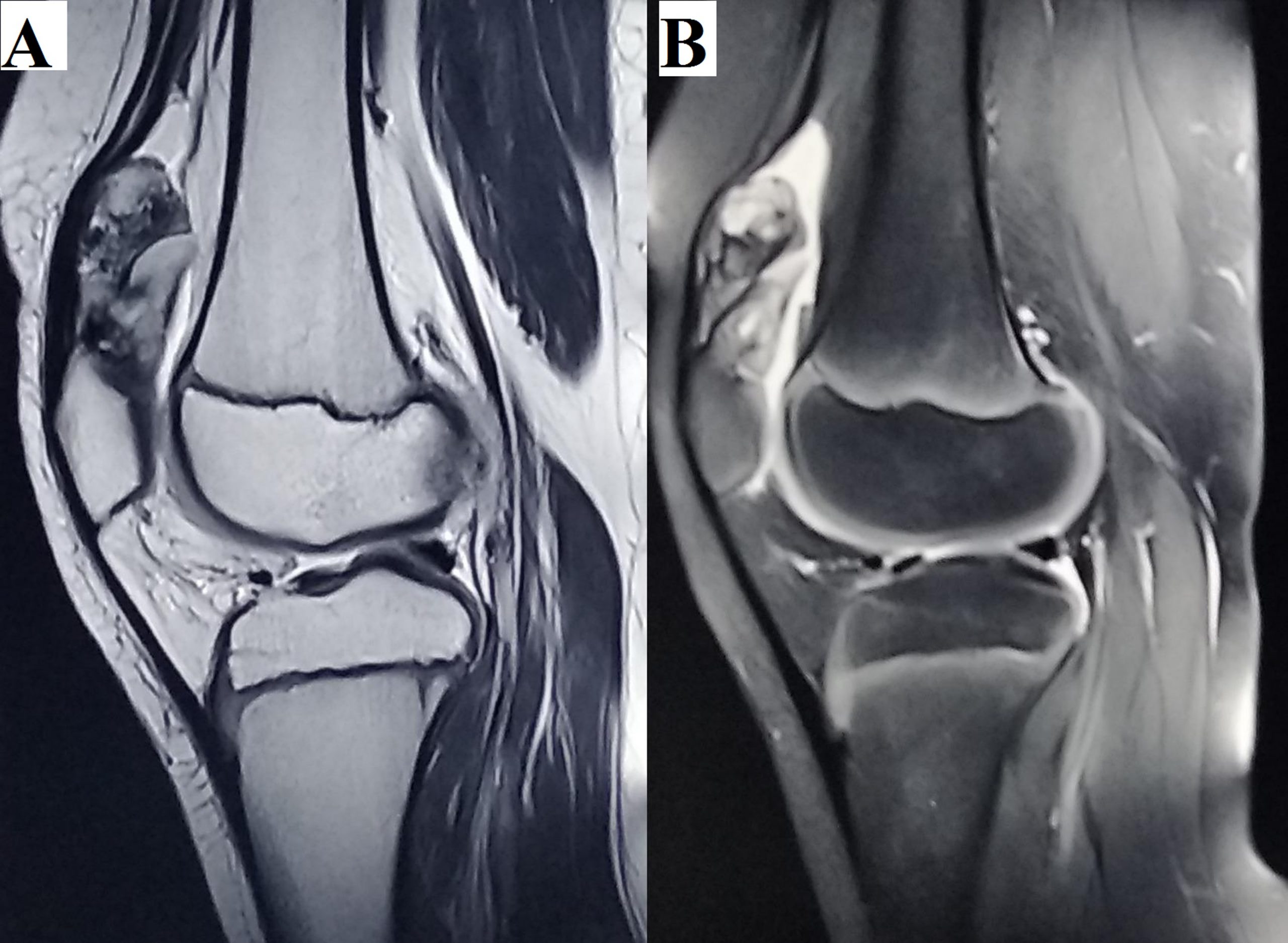
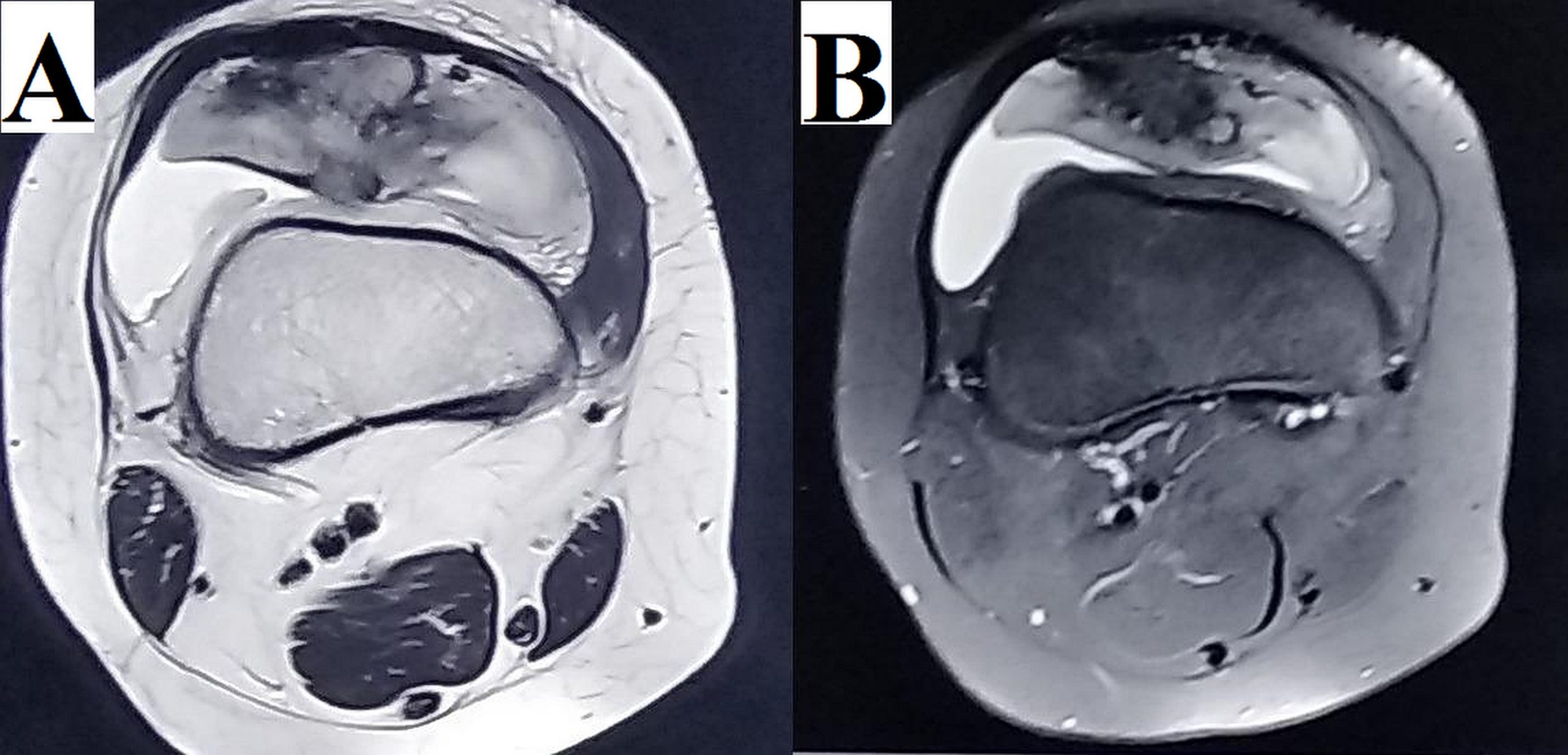
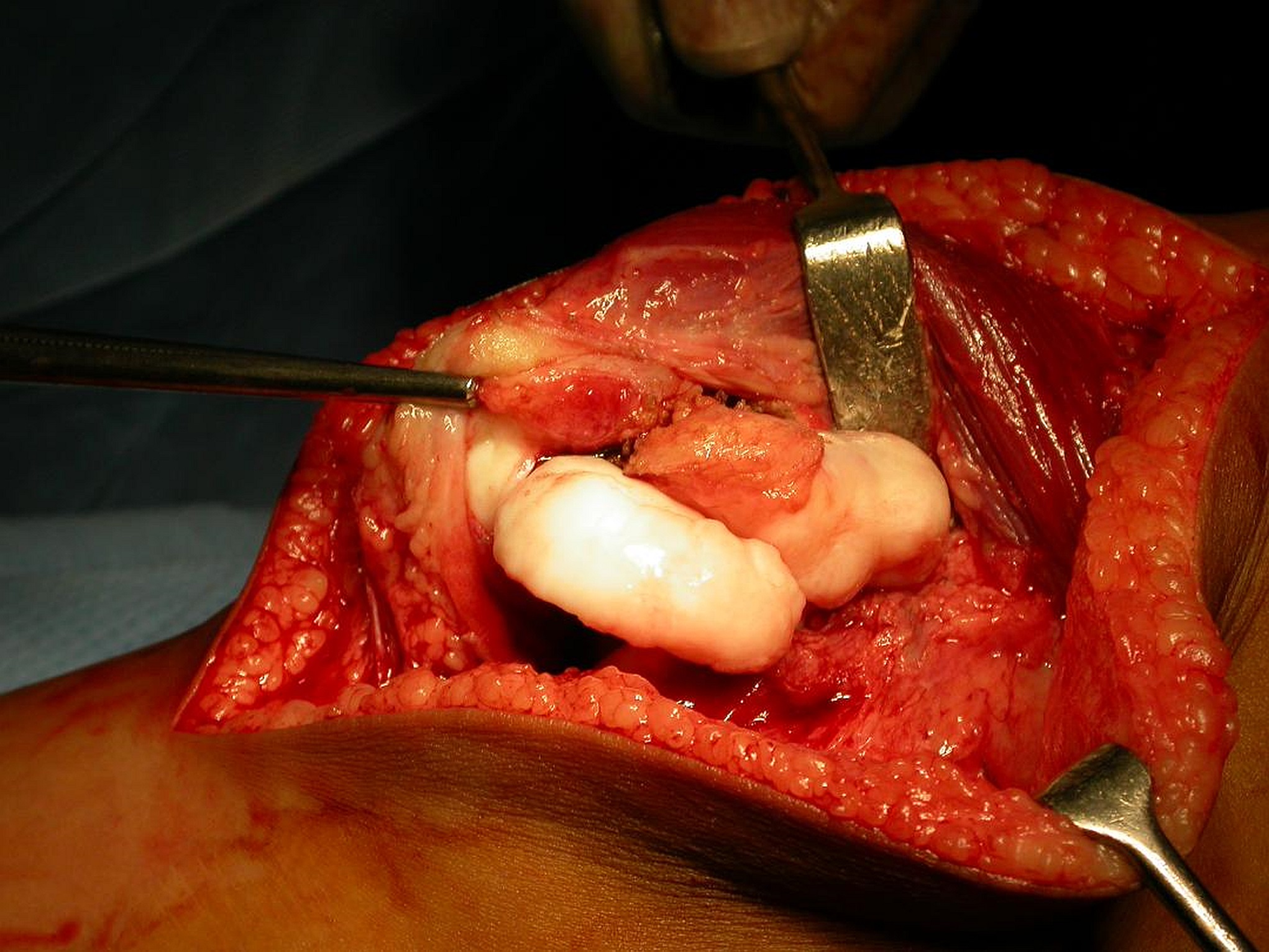
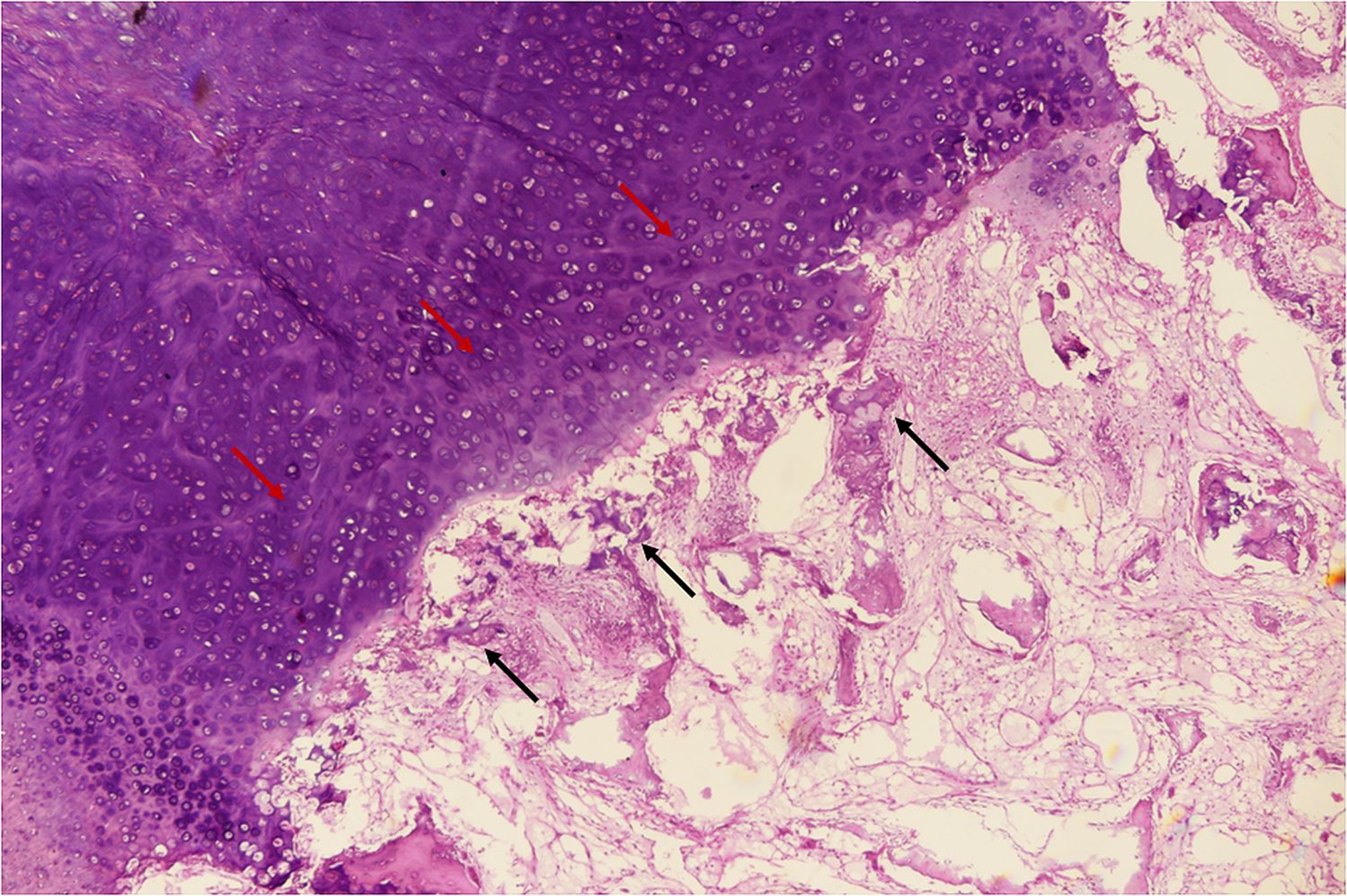
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 6
Fig. 6An 11-year-old boy came to our outpatient department with symptoms of pain and swelling in the right knee. He had noticed the swelling 6 months previously and since then there was a gradual increase in size. There was no history of fever or trauma. On examination, local temperature was normal. There was no tenderness. Swelling was localized to the anteromedial aspect of the right knee in the suprapatellar region. It seemed to be fixed to the patella because both were moving as a unit. It was firm on palpation. The patient had full knee extension, but flexion was restricted by 30° on the affected side in comparison with the contralateral normal knee. On radiographic evaluation, there was a bony outgrowth with associated mass originating from the superior pole of the patella. This mass had focal areas of calcification (Fig. 1). On computed tomographic (CT) scans, similar findings were noted (Fig. 2). On magnetic resonance imaging (MRI), the mass had low to intermediate signal intensity on T1-weighted images and isointense to hyperintense signal on T2-weighted images, suggestive of a cartilage component (Figs. 3 and 4). Routine blood investigations were within the normal limits. After diagnostic evaluation, an excision biopsy of the mass was planned. The patient underwent an operation that included an anterior midline incision and a medial subvastus approach. A multilobulated mass was found to be arising from the superior pole of the patella. The surface of the mass was in continuity with the articular cartilage of the superomedial aspect of the patella. The mass was excised along with its bony stalk. It measured 6.2 cm longitudinally, 3.7 cm in transverse extent, and 3 cm in depth (Fig. 5). The histology of the excised tissue is shown in Figure 6.
The radiographic, intraoperative, and histologic findings were interpreted as dysplasia epiphysealis hemimelica (Trevor disease) of the patella.
The postoperative period was uneventful. The patient was able to regain full range of movements by 4 weeks. The patient was regularly followed, and at the last follow-up visit, there was no evidence of recurrence.
Proceed to Discussion >>Reference: Vashisht S, Aggarwal P, Bhagat R, Garg A, Gupta PN, Garg SK. Dysplasia epiphysealis hemimelica (Trevor disease) of the patella: a case report. JBJS Case Connect. 2020 Jul-Sep;10(3):e20.00003.
The patella is a sesamoid bone that develops in the tendinous expansion of the quadriceps femoris muscle on the anterior aspect of the knee. At 4 to 5 years of age, it is an expanding mass of cartilage similar to unossified epiphyseal cartilage. The centrally located ossification center appears at this age, and there is rapid enlargement of ossification center. Slowdown of ossification occurs at 10 to 11 years of age. During adolescence, ossification extends to the whole of the patella except its articular surface. Dysplasia epiphysealis hemimelica of the patella can occur at any time in the period between the appearance of the ossification center and the completion of the ossification.
The pathogenesis of dysplasia epiphysealis hemimelica is not yet fully known. Trevor considered it to be a congenital defect in the development of epiphyseal bud resulting in persistent proliferation of articular cartilage, leading to the formation of a large cartilaginous mass. Other authors have suggested that dysplasia epiphysealis hemimelica occurs because of a defect in the regulation of cartilage proliferation in the affected epiphysis leading to formation of cartilaginous exostosis. The abnormalities in microvasculature of fetal epiphysis and abnormal polarity of epiphyseal chondrocytes might be other possible explanations.
Radiographic appearance may vary and depends on the age at which dysplasia occurs. Commonly observed radiographic features include lobulated ossific mass, irregular ossification center, asymmetric epiphyseal enlargement, or a combination of the features. Hypertrophic disorganized cartilage component before ossification may present as an abnormal soft-tissue mass. In the initial stage, the lesion is primarily cartilaginous and then enchondral ossification occurs. Therefore, initially, MRI shows a low to intermediate T1-weighted signal and a hyperintense T2-weighted signal. Due to the disorganized hypertrophy of the cartilage, the T2-weighted signal is more hyperintense in comparison with the normal cartilage. At the later stage, after ossification, there is a low signal on both the T1-weighted and T2-weighted sequences.
The differential diagnosis of dysplasia epiphysealis hemimelica includes osteochondroma, multiple epiphyseal dysplasia, metachondromatosis, and synovial chondromatosis. Osteochondromas originate from the metaphyseal region and grow away from the joint. In contrast to dysplasia epiphysealis hemimelica, skeletal dysplasias are characterized by the small size of the epiphysis and have an association with dwarfism. Metachondromatosis is a genetic disorder caused by involvement of the PTPN11 gene and characterized by both osteochondroma and enchondroma formation. This disorder usually affects the hands and feet and consists of periarticular calcified soft-tissue mass. Chondromatosis does not have a predilection for the ossification center and has diffuse intra-articular distribution.
Dysplasia epiphysealis hemimelica is classified into 3 types: localized, classic, and generalized. In the localized form, there is involvement of only one epiphysis. In the classic form, there is involvement of more than one epiphysis in the same limb, and in the generalized form, there is involvement of the entire lower extremity. Because only the patella was involved in our case, it was a localized-type disease. There are certain pitfalls of this classification because isolated upper-extremity and combined upper and lower-extremity involvement were not included. To overcome these pitfalls, another classification system was proposed where disease was classified into 6 types based on the number of joints involved and the extremity affected. There is a single lower-extremity involvement in Type 1, multiple joint involvement of the lower extremity in Type 2, single joint involvement of the upper extremity in Type 3, multiple joint involvement of the lower extremity in Type 4, both upper and lower-extremity involvement in Type 5, and spine involvement in Type 6. However, this classification did not include patients with bilateral involvement. A comprehensive classification system has been proposed that incorporates features of both of the above mentioned classifications and bilateral involvement.
The management of dysplasia epiphysealis hemimelica patella depends on the symptoms. In asymptomatic patients, conservative treatment is advised. In symptomatic patients having pain, large swelling, limitation of joint movements, or deformity, surgical treatment in the form of complete excision of the mass and curettage of the ossification center are recommended. Recurrence is usually associated with partial excision of the mass lesion. Radical treatment in the form of partial or total patellectomy should be reserved for a recurrent lesion. In this case, complete excision was performed because the patient reported pain, progressive increase in swelling, and restricted movements of the affected knee.
On histopathology, there are similarities between the dysplasia epiphysealis hemimelica and osteochondroma. In the present case also, histopathological findings were similar to osteochondroma with a large cartilaginous cap.
Written consent was obtained from the patient’s parents to publish this case report.
Reference: Vashisht S, Aggarwal P, Bhagat R, Garg A, Gupta PN, Garg SK. Dysplasia epiphysealis hemimelica (Trevor disease) of the patella: a case report. JBJS Case Connect. 2020 Jul-Sep;10(3):e20.00003.
What is the diagnosis?
Dysplasia epiphysealis hemimelica (Trevor disease)
Giant juxta-articular (para-articular) osteochondroma
Synovial chondromatosis
Periosteal chondroma of the patella
Heterotopic ossification of a Hoffa fat pad