


 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 4-A
Fig. 4-A Fig. 4-B
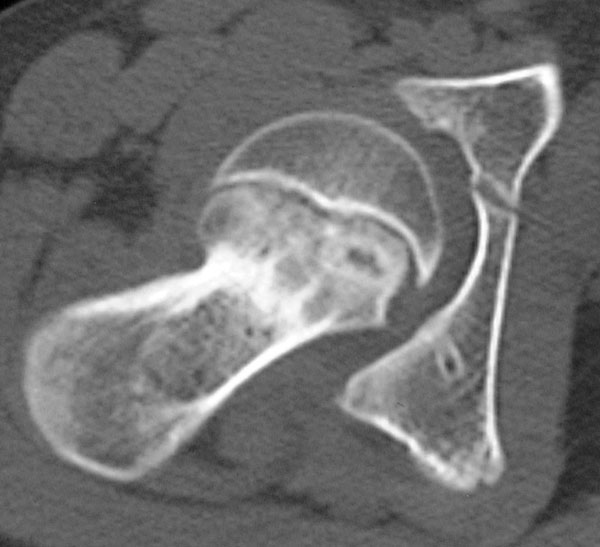
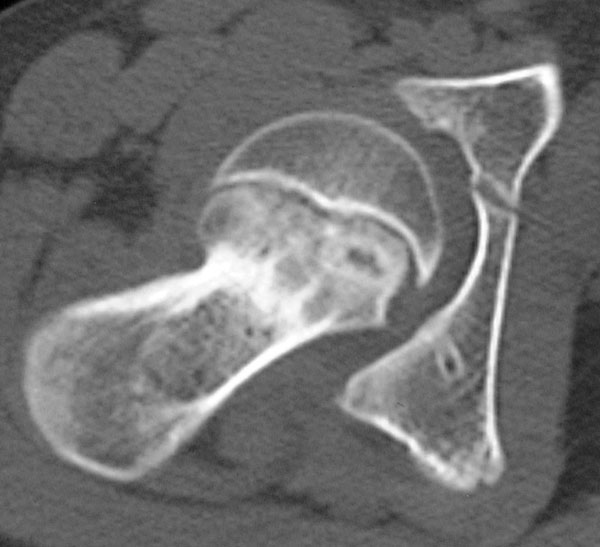
Fig. 4-BAn eleven-year-old girl presented with a two-month history of pain in the right knee. There was no history of trauma to the right hip or knee. Physical examination revealed a well-developed, well-nourished girl. She was 143 cm tall and weighed 39 kg. The body mass index was 19.1. The physical examination was normal, except with regard to the right lower extremity. She walked with a right antalgic gait. The right leg was 2.0 cm shorter than the left. Hip motion was not painful, and there was neither tenderness nor swelling about the right hip. Range of motion of the right hip included 15° of external rotation, 80° of internal rotation, 115° of flexion, and a 30° flexion contracture. As the right hip was flexed, adduction and internal rotation occurred spontaneously. Radiographs and computed tomography were performed.
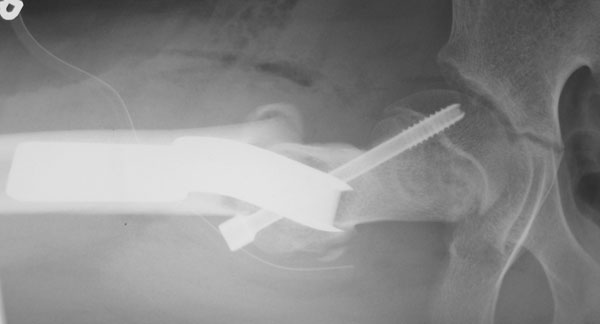
The plain radiographs and computed tomographic images revealed an anterior-inferior slip of the capital femoral epiphysis of the right hip (Figs. 1-A, 1-B, 2-A, and 2-B). The growth plate was still open and was slightly widened and irregular. The angle of the slip was measured according to the method described by Southwick and was −86°. The anterior tilting angle of the contralateral femoral epiphysis was 14°, indicating mild anteversion. She had no endocrinologic or renal disorder. Surgical treatment consisted of an intertrochanteric osteotomy with in situ screw fixation of the capital femoral epiphysis (Figs. 3-A and 3-B), done with the patient in the left lateral decubitus position. The osteotomy, which was a modification of the original Southwick method, resulted in a correction of 30° of extension, 30° of valgus, and 20° of external rotation. A 90° blade-plate was used to fix the osteotomy. The epiphysis was stabilized in its slipped position by a single screw without any attempt at reduction. Because the direction of the slip was anterior, the screw was inserted from a posterolateral entry site under fluoroscopic control. The patient resumed her full range of activities four months after the operation. One year after the operation, union of the osteotomy sites and epiphysiodesis were completely achieved, and the implants were removed. As of the most recent follow-up, thirty months after the operation, the patient was completely asymptomatic. Radiographs of the right hip demonstrated no evidence of osteonecrosis of the femoral head, and the joint space appeared normal (Figs. 4-A and 4-B).
Proceed to Discussion >>Reference: Sasaki M, Nagoya S, Kaya M, Yamashita T. Anterior slip of the capital femoral epiphysis. A case report. J Bone Joint Surg Am. 2007;89:855-8.
Most commonly in slipped capital femoral epiphysis, the femoral head slips posteriorly and inferiorly. Anterior slip of the epiphysis is extremely uncommon, with only two cases reported in the literature. Risk factors for posterior displacement of the femoral head are thought to include external rotatory forces produced by the external rotator muscles, which occur during sitting; increased femoral retroversion; and increased physeal posterior slope. However, the mechanism for the unusual direction of an anterior slip remains unclear. With regard to the mechanism of an anterior slip, the authors of previous reports speculated that a sudden internal rotation of the hip might be a contributing factor. However, the patient in the present case report presented with an anterior slip with no history of trauma, which leaves no explanation for the mechanism of this direction of slip. The anterior tilting angle of the intact contralateral femoral epiphysis was 14°, indicating mild anteversion. Since femoral retroversion is thought to be a risk factor for posterior slipped capital femoral epiphysis, it is tempting to speculate that femoral anteversion may contribute to anterior slip, although this premise remains unproven. According to the classification system of Southwick, the degree of the displacement for this patient would be categorized as moderate to severe. Treating such an advanced condition is difficult because of the high prevalence of postoperative complications, including osteoarthritis, osteonecrosis of the femoral head, and chondrolysis. For a severely slipped epiphysis, an osteotomy at the level of the physis or an intertrochanteric osteotomy with in situ screw fixation of the capital femoral epiphysis has been reported to be successful. Although the correction of the deformity was incomplete in this patient, the use of a Southwick-type osteotomy improved joint congruity and allowed the anteriorly displaced articular cartilage surface to be repositioned into the acetabulum. At the time of the latest follow-up, there was no sign of osteonecrosis of the femoral head or osteoarthritis and the patient had returned to normal activity. Intertrochanteric osteotomy with in situ screw fixation of the capital femoral epiphysis remains one of the options for the treatment of patients with severe anterior slip of the capital femoral epiphysis.
Reference: Sasaki M, Nagoya S, Kaya M, Yamashita T. Anterior slip of the capital femoral epiphysis. A case report. J Bone Joint Surg Am. 2007;89:855-8.






Persistant subcapital femoral neck stress fracture
Anterior slip of the capital femoral epiphysis
congenital coxa vara of right hip
hemangioma of femoral neck with buckle fracture