A Nineteen-Year-Old Woman with Left Shoulder Pain
September 2, 2015
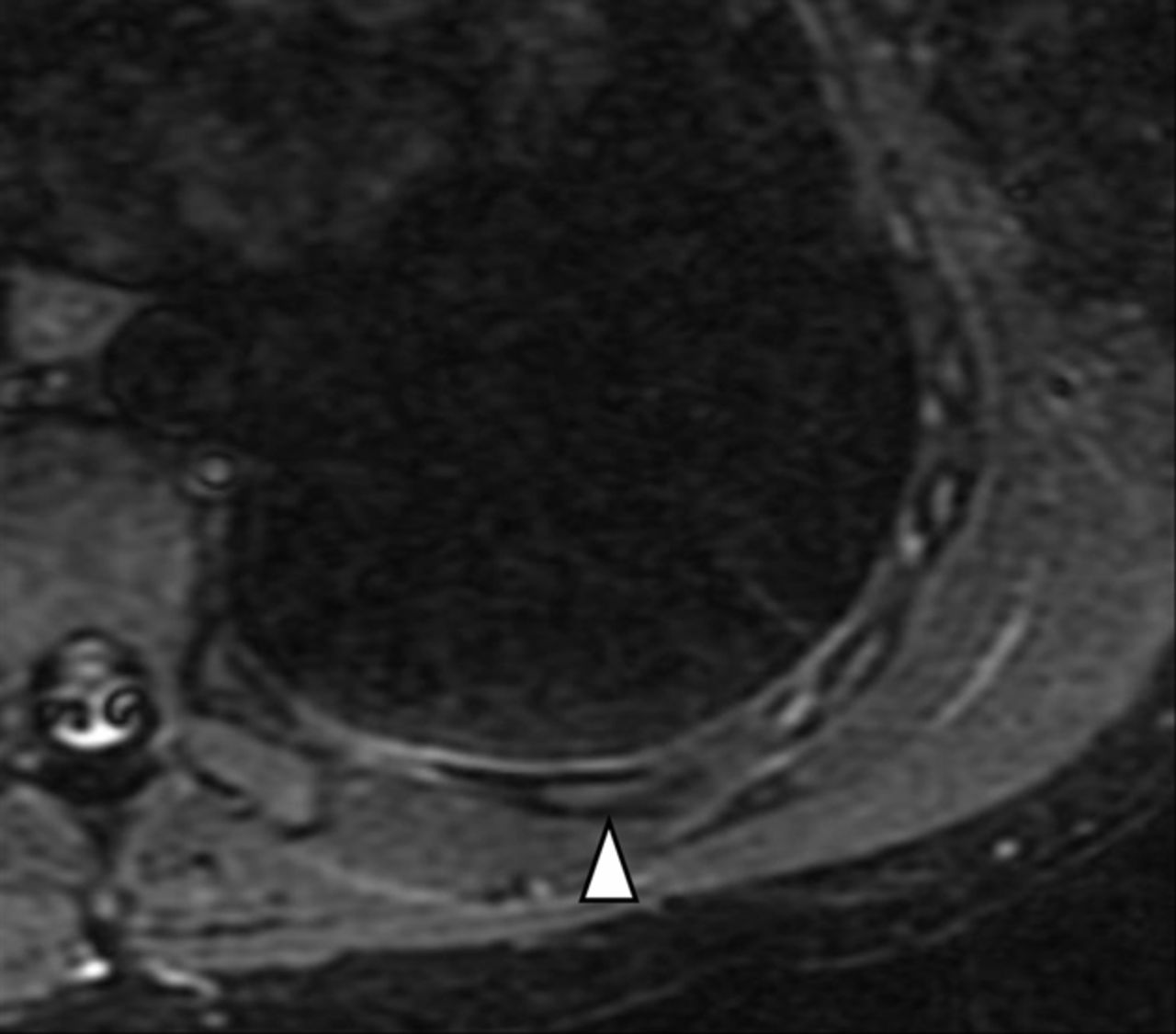
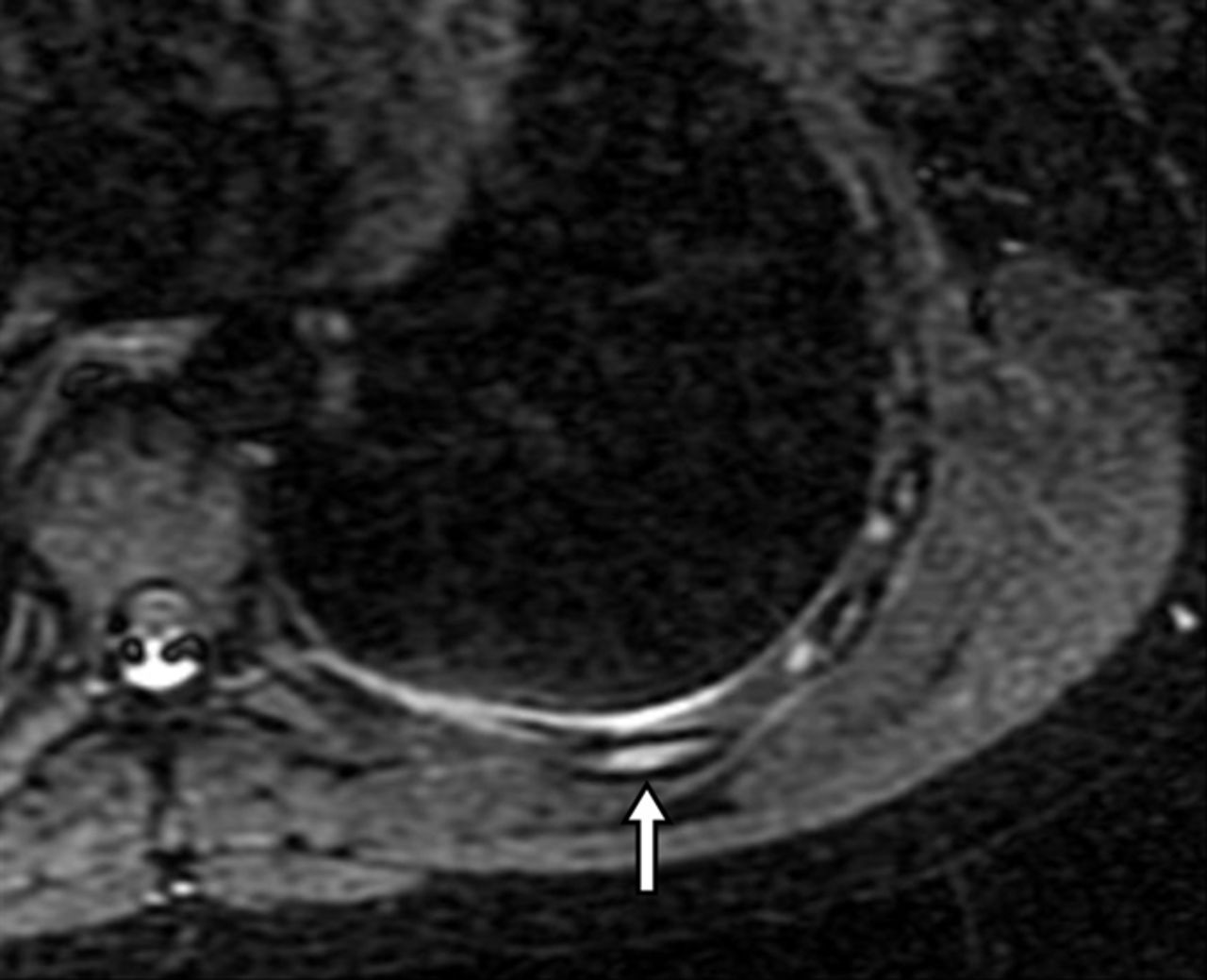
 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2
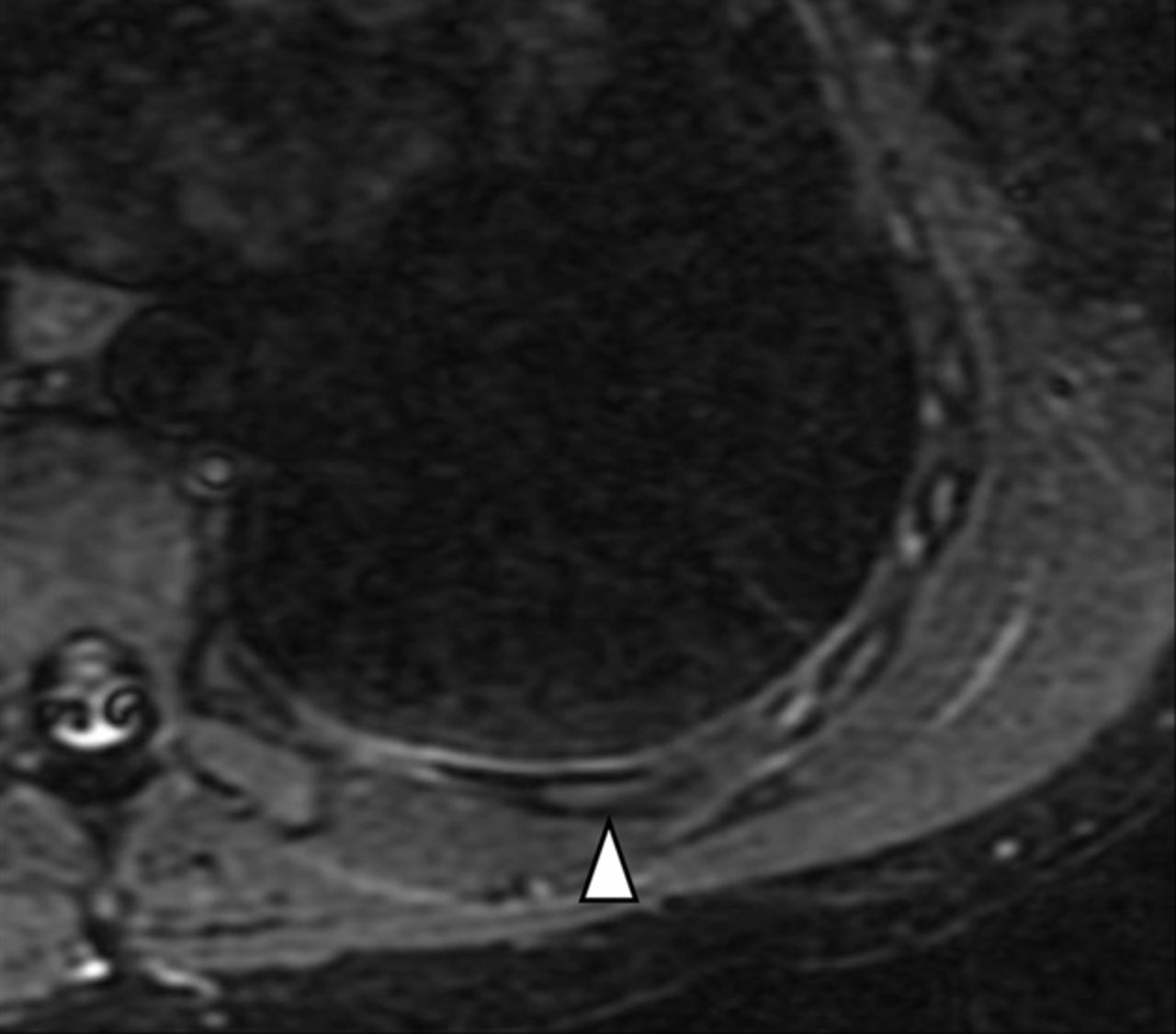
Fig. 2A nineteen-year-old, right-hand-dominant female rower presented to the clinic with left periscapular pain. She had previously experienced right-sided pain of a similar nature when she had been a port-side rower. When she had switched to become a starboard-side rower, the right-sided pain gradually subsided, but over the next year she had developed left-sided pain. She described the pain as starting at the beginning of the finish phase, as well as with full extension and scapular protraction. She noticed this pain most often when she was training on the ergometer. The pain had progressed to the point where she had pain at rest and during sleep, as well as pain in the periscapular region while taking a deep breath. She reported the sensation of having a “knot” in the muscles surrounding the inferior aspect of the left scapula. There was no reported mechanism for an acute injury. There was no history of scoliosis or other back problems. Examination demonstrated neck and shoulder motion within normal limits. There was tenderness over the inferior aspect of the left scapula as well as the lateral chest wall, over the serratus anterior muscle. There was mild restriction in left-sided shoulder internal and external rotation (T5 versus T3) compared with the right shoulder. There was mild winging of the left scapula noted on observation of a wall push-up. Given the clinical history and physical examination, there was very high concern for a stress fracture. At the initial visit, radiographs of the left shoulder demonstrated no abnormalities. As a result, an MRI of the left shoulder and rib cage was ordered (Figs. 1-A and 1-B). In the meantime, the patient began physical therapy, avoiding any ergometer training or rowing activity. On completion of the magnetic resonance imaging (MRI), an additional review of the chest radiographs was performed.
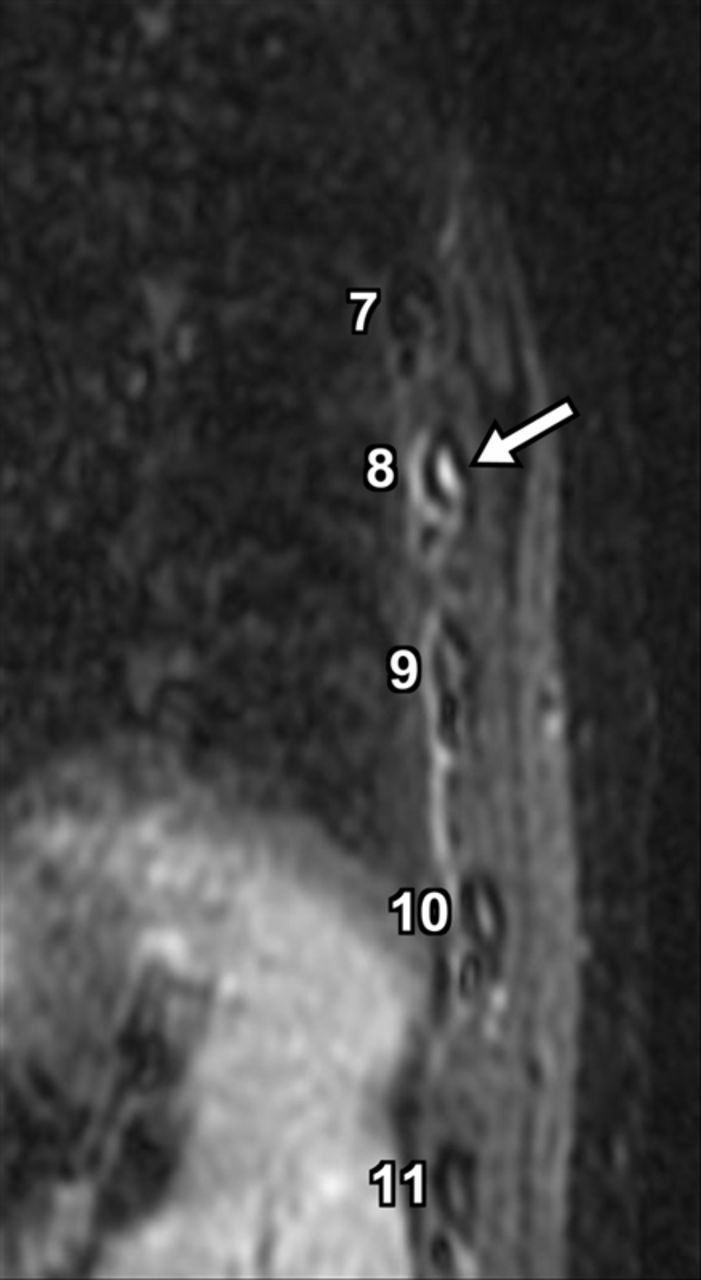
The chest radiograph demonstrated cortical discontinuity along the posterolateral aspect of the eighth rib, and the MRI demonstrated increased marrow signal along the posterior level of the eighth rib. The difference between normal and abnormal marrow was clearly seen in axial short tau inversion recovery (STIR) images (Figs. 1-A and 1-B). Sagittal images demonstrated increased signal intensity in the eighth rib compared with the other ribs (Fig. 2). After the diagnosis of stress fracture of the eighth rib was confirmed, the patient began rehabilitation, with restriction from rowing activities for six weeks.
Proceed to Discussion >>Reference: Knesek M, Walsh CP, Sabb B, Bedi A. Magnetic resonance imaging diagnosis of rib fracture in a competitive collegiate rower: A case report. JBJS Case Connect. 2012 Oct 10;2(4):e56.
Rib stress fractures account for a substantial amount of time lost from training and competition for rowers. Various studies report the rate of rib stress fractures in competitive rowers to range from 6.1% to 22.6%. There are numerous theories regarding the mechanism and pathophysiology of rib stress fractures in these rowers. Multiple muscles acting on the ribs have been implicated because of considerable repetitive forces and possible muscle imbalances that may predispose to stress fractures. Analysis in cadavers has shown that the serratus anterior muscle can generate force that is sufficient enough to break ribs in the posterolateral region. Scapular retractors have been implicated as well, potentially because of force generated during the drive phase with leg extension. The abdominal oblique muscles have also clearly demonstrated deforming actions on ribs that could contribute to stress fractures. A high clinical suspicion for rib stress fractures in elite rowers is very important since these injuries are relatively infrequently encountered in the general clinical setting. The history and physical examination remain important in the diagnosis, and several different imaging modalities can be used to confirm the clinical diagnosis. Conventional radiographs are often normal in the early setting of a stress reaction since abnormalities are only detected later, when periosteal or endosteal new bone formation is evident. Computed tomography (CT) imaging is also poorly sensitive in the early stages of stress injuries; however, fracture lines may be identified. Radionuclide bone scanning is extremely sensitive for detecting osseous stress injuries, even in the early stages, by screening the entire skeleton. Positron emission tomography has also been used to diagnose osseous stress reaction since it is another modality that screens for global metabolism. MRI is at least as sensitive as radionuclide scanning to detect osseous stress injuries by demonstrating marrow edema and periosteal fluid. MRI does offer certain advantages over other modalities such as radionuclide scanning, including shorter scan time, no ionizing radiation, improved specificity from the spatial resolution of the MRI, and simultaneous imaging of both bone and soft tissue. However, MRI is limited because it is not used for screening the entire skeleton. Thus, multiple imaging modalities allow the clinician to confirm or disprove stress fractures in competitive rowers. To the best of our knowledge, our case is one of the first reported uses of MRI to diagnose a stress fracture involving the rib of a competitive rower, and we believe that this modality holds promise for future early diagnoses of rib stress fractures. Rib stress fractures in elite rowers can be a common cause of chest pain, back pain, or periscapular pain. There are, however, multiple other causes of these symptoms, and diagnostic workup is necessary for a definitive diagnosis. Prompt recognition and diagnosis is important for correct therapy and rehabilitation. Various studies, including conventional radiographs, CT scans, radionuclide scans, and MRI, all have the ability to confirm stress fractures, although some are more sensitive than others. Although radionuclide scans remain the most commonly ordered study to confirm the diagnosis of rib stress fracture, MRI is a very good alternative that has multiple advantages over other imaging modalities. Our case highlights the ability of MRI to very clearly identify a stress fracture involving the eighth rib of a competitive rower.
Reference: Knesek M, Walsh CP, Sabb B, Bedi A. Magnetic resonance imaging diagnosis of rib fracture in a competitive collegiate rower: A case report. JBJS Case Connect. 2012 Oct 10;2(4):e56.

Periostitis of the scapular body
Osteoblastoma of the eighth rib
Fibrous dysplasia of the eighth rib
Stress fracture of the eighth rib
Scapular body osteoblastoma