Severe Unrelenting Pain in the Lumbosacral Paraspinal Area after Skiing
October 7, 2009
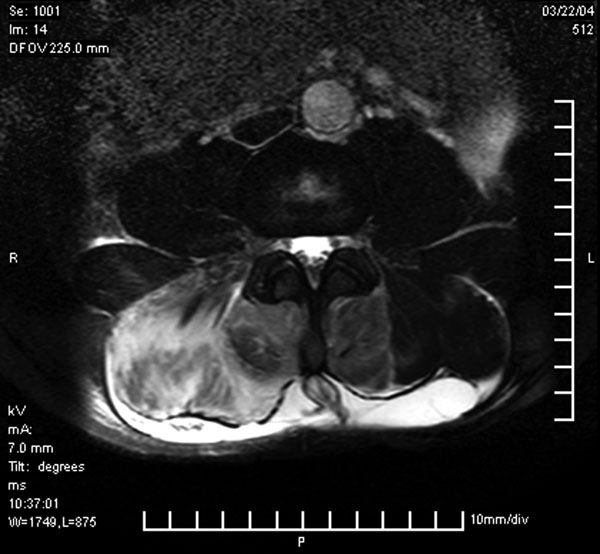
 Fig. 1
Fig. 1 Fig. 1
Fig. 1A thirty-five-year-old man on the third day of a skiing holiday presented to the emergency department because of severe, unrelenting pain in the right lumbosacral paraspinal area, radiating across the abdomen to the groin. The pain had been present for four hours and had begun spontaneously with no history of trauma. In retrospect, the patient had experienced similar but milder pains during previous ski trips and during long-distance running. There was associated numbness in the right lumbosacral area. Positive findings on physical examination were bilateral paraspinal muscle rigidity associated with swelling, marked tenderness, and loss of the lumbar lordosis. There was dense loss of sensation in the paraspinal area to the midaxillary line and altered sensation extending anteriorly to the midline. Reduced abdominal muscle tone on the right side, resulting in asymmetry, was also noted. Active movement of the spine was minimal and exacerbated the pain. The patient had mild tenderness of the abdomen with absent bowel sounds. The initial differential diagnosis included a renal stone, a herniated disc, discitis, and a retroperitoneal abnormality. A urine specimen was dark in appearance, and analysis revealed 3+ myoglobinuria. Blood chemistry studies showed elevation of aspartate aminotransferase (804 IU/L; normal, 17 to 59 IU/L), alanine aminotransferase (141 IU/L; normal, 21 to 72 IU/L), lactate dehydrogenase (3823 IU/L; normal, 313 to 618 IU/L), myoglobin (7961 ng/mL; normal, <116.4 ng/mL), and creatine kinase (48,550 IU/L; normal, 55 to 70 IU/L). Other blood parameters were within normal limits. A spiral computerized tomography study excluded an abnormality of the urinary tract. Swelling of the paraspinal muscles and a paralytic ileus were noted. Angiography showed no evidence of arterial occlusion. The pain was controlled with opioids, and it was elected to continue treatment with intravenous rehydration although a definitive diagnosis had not been made. Twelve hours after presentation, the patient had little improvement. A magnetic resonance imaging scan revealed a marked increase in signal within the medial and lateral right paraspinal muscles as well as the left medial paraspinal muscle (Fig. 1). An increased signal was also noted within the soft tissues adjacent to the spinous processes and posterior to the paraspinal muscles. There was asymmetry of the paraspinal muscles, with the right side notably larger than the left. Some fluid was also noted in the right retroperitoneal region.
Pressures were measured with a transducer (Intra-Compartmental Pressure Monitor; Stryker, Kalamazoo, Michigan). The needle was inserted into the paraspinal muscle compartment at the level of maximal tenderness (approximately L2). Pressure in the paraspinal muscle was 44 mm Hg on the right side and 26 mm Hg (normal, 3.1 to 10.8 mm Hg) on the left side. By this time, the serum creatine kinase level had increased to 59,863 IU/L. The diagnosis of acute compartment syndrome of both paraspinal muscle groups with rhabdomyolysis was confirmed. The patient underwent bilateral fasciotomy of the lumbar paraspinous muscle through a midline incision, from the level of the first lumbar vertebra to the first sacral vertebra. At the time of surgery, the deeper muscles were pale but soon turned pink, bled, and responded to stimulation following decompression. Intraoperatively, the pressures returned to normal (<10 mm Hg). Postoperatively, the patient had notable improvement with respect to pain and, by the following day, he was able to walk with crutches. The serum creatine kinase level decreased to 4600 IU/L over the next five days. There were no postoperative complications apart from a wound seroma that resolved following six aspirations. Within four weeks, the patient had returned to sports with no further back pain. The numbness and reduced abdominal muscle tone resolved after three months.
Proceed to Discussion >>Reference: Khan RJK, Fick DP, Guier CA, Menolascino MJ, Neal MC. Acute paraspinal compartment syndrome. A case report. J Bone Joint Surg Am. 2005;87:1126-8.
Anatomic cadaver studies have demonstrated a well-defined closed paraspinal space comprised of the erector spinae muscle enclosed by the posterior and middle lamellae of the thoracolumbar fascia. The fascial envelope is anatomically and physiologically similar to other muscle compartments known to be susceptible to compartment syndrome. Physiological studies have measured compartment pressures within the paraspinal muscle groups. Normal compartment pressure has been reported to be between 3.1 and 10.8 mm Hg when measured in the prone position, and the pressure at which subjects have muscle fatigue during exercise has been reported as 14 mm Hg. Pressures have been reported to vary with posture, and they are particularly high when standing with the knees in flexion, which simulates the skiing stance. Chronic compartment syndrome of the paraspinal muscles has been recognized as an uncommon cause of back pain. Acute paraspinal compartment syndrome, conversely, is very rare. It appears to have three causes: direct trauma to the paraspinal muscles; occlusion of the blood supply to the paraspinal muscles during aortic abdominal aneurysm repair, followed by a reperfusion injury; or atraumatic acute compartment syndrome. A closer analysis of the cases of three other patients who had atraumatic acute compartment syndrome revealed that they had many features in common that have not previously been recognized (see Appendix in reference 1). These features include bilateral lumbar paraspinal muscle spasm with loss of lordosis and marked tenderness as well as reduced or absent bowel sounds. The laboratory investigations showed myoglobinuria, normal acute phase inflammatory markers, and elevated levels of aspartate aminotransferase, alanine aminotransferase, myoglobin, and serum creatine kinase. Interestingly, two of the patients also had associated numbness involving the cutaneous nerves traversing the paraspinal muscle compartment—a relatively late sign in compartment syndrome of the leg. In addition, our patient had a motor disturbance with a reduction of abdominal muscle tone. All four patients, including ours, who had atraumatic acute compartment syndrome were initially managed with fluid resuscitation and opioids, since the diagnosis was unclear. Of the three patients in whom the diagnosis was confirmed during hospitalization, two had no improvement in the clinical condition and surgical intervention was undertaken. It is of note that both of these patients went on to make a full recovery without recurrence of the previous pain, even on exertion. Both patients who were managed nonoperatively reported at the follow-up examination that they had pain with exercise. Surgeons need to be aware of the existence of acute paraspinal compartment syndrome to aid in its early identification. There should be a low threshold for measuring paraspinal compartment pressures, particularly in patients with severe back pain who present with paraspinal muscle rigidity and increased levels of serum creatine kinase, when other diagnoses have been excluded.
Reference: Khan RJK, Fick DP, Guier CA, Menolascino MJ, Neal MC. Acute paraspinal compartment syndrome. A case report. J Bone Joint Surg Am. 2005;87:1126-8.

Rhabdomyosarcoma of paraspinal muscles
Necrotizing fasciitis of paraspinal muscles
Acute compartment syndrome of paraspinal muscles