




 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 2-C
Fig. 2-C Fig. 3
Fig. 3 Fig. 4-A
Fig. 4-A Fig. 4-B
Fig. 4-B Fig. 5-A
Fig. 5-A Fig. 5-B
Fig. 5-BA 51-year-old generally healthy male farmer presented for evaluation. He makes a living by planting dragon fruit and raising poultry. He had no medical history of hypertension, diabetes mellitus, peripheral vascular disease, or osteomyelitis. He visited our orthopaedic outpatient department because of a 3-month history of right plantar heel pain with swelling and tenderness, and a limping gait, without an obvious trauma episode. Before coming to our hospital, he had visited many local clinics, and plantar fasciitis had been diagnosed. He had received several steroid injections and extracorporeal shockwave therapy, but the symptoms had worsened.
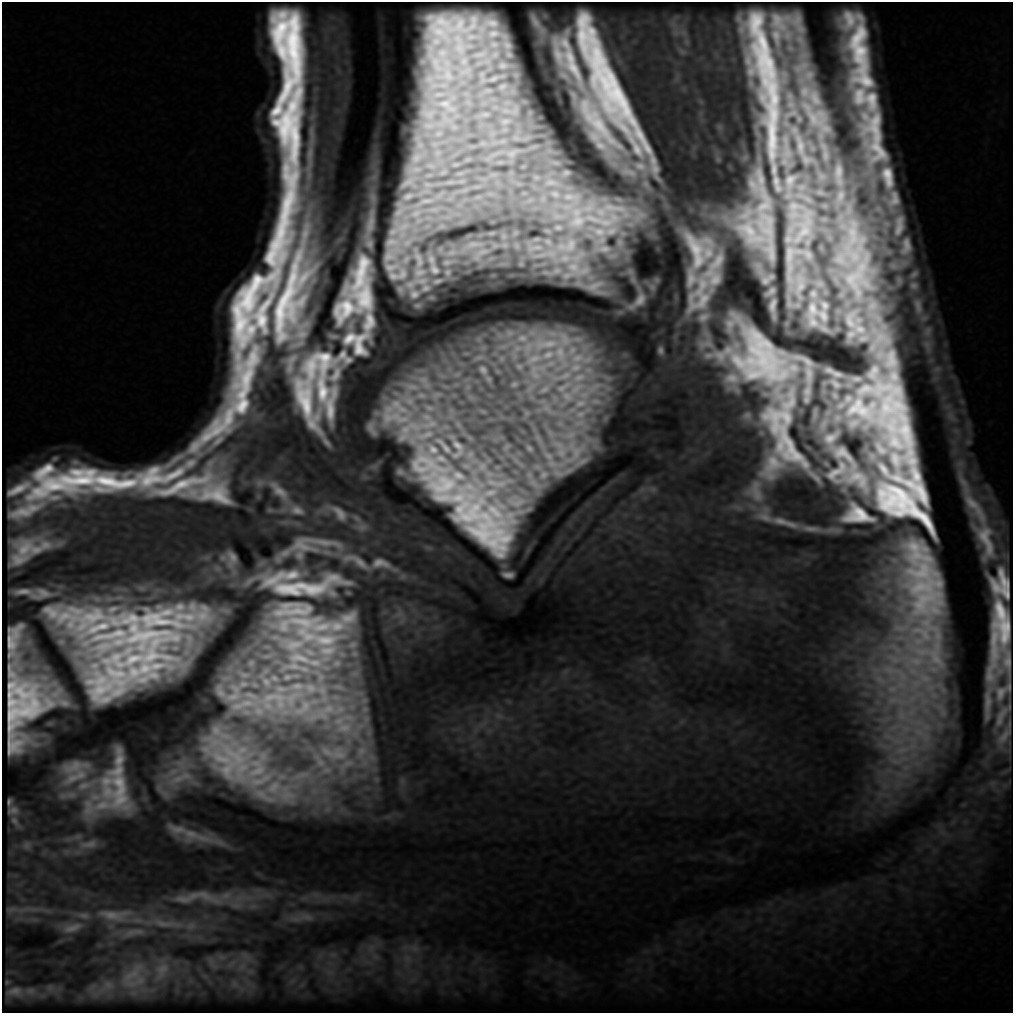
On physical examination, the typical presentation of plantar fasciitis, including the sudden onset of pain and pain in the medial aspect of the heel, was absent. In addition, the calcaneal squeeze test was positive. Because a calcaneal etiology was suspected, radiographs were made; they revealed erosion over the plantar cortex of the right calcaneus (Figs. 1-A and 1-B). Contrast-enhanced magnetic resonance imaging (MRI) suggested osteomyelitis, but a neoplasm also was possible (Figs. 2-A, 2-B, and 2-C). Therefore, we arranged immediate surgical treatment.
During the surgery, the tumor-like lesions were excised, and the calcaneus was extensively debrided (Fig. 3).
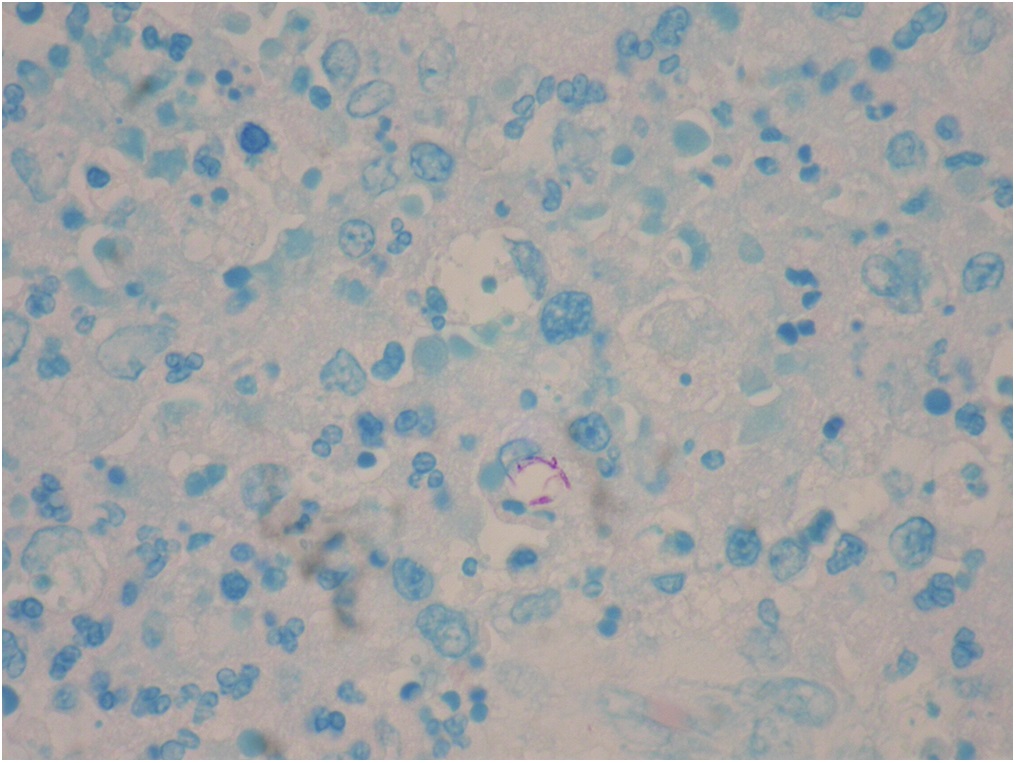
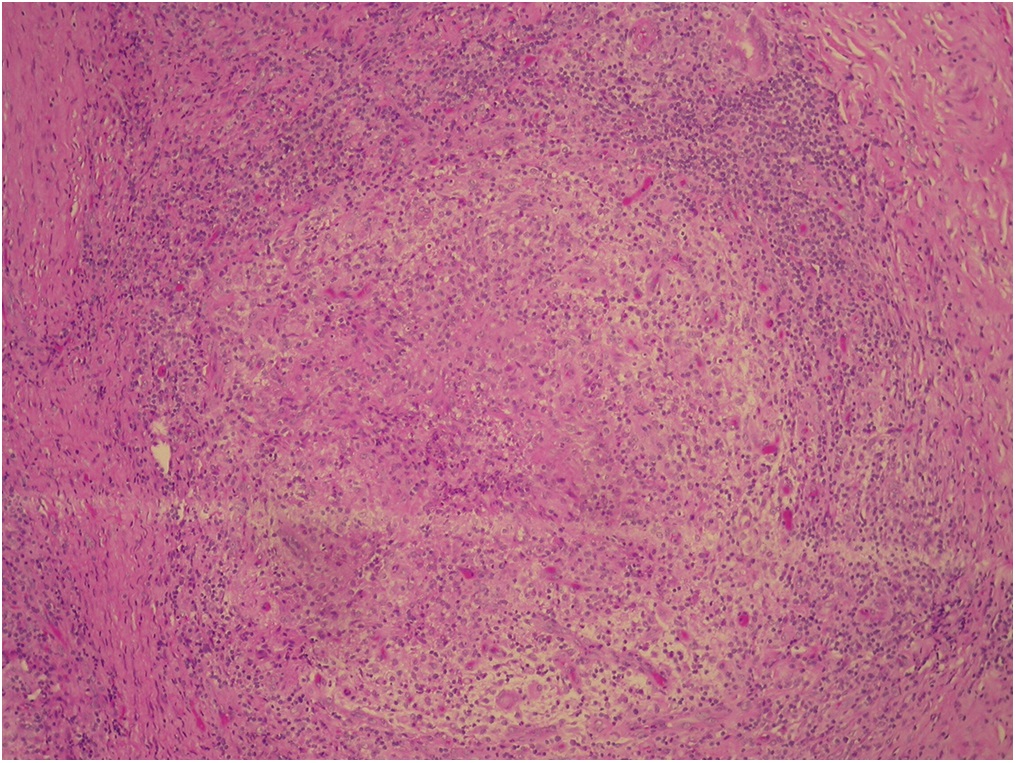
The excised lesions were sent for histologic examination. Intravenous oxacillin was empirically prescribed for infection control. The histology of the excised tissue is shown in Figures 4-A and 4-B.
The histology demonstrated granulomatous inflammation, and a stain for acid-fast bacilli was positive. Consistent with the histology, on postoperative day 14, the mycobacterial culture revealed a rapid-growth non-tuberculous mycobacterial infection. Subsequent typing revealed Mycobacterium abscessus.
Plain chest radiography and 3 sets of sputum cultures were negative for tuberculosis. After the positive cultures were obtained, antibiotics were changed to antimycobacterial agents. Because cefoxitin was not available at our institute, we chose intravenous amikacin and Tienam (500 mg of imipenem with 500 mg of cilastatin per vial) combined with oral clarithromycin as the initial treatment regimen.
The symptoms improved gradually with medication treatment. The patient was discharged 4 weeks later with oral ciprofloxacin, doxycycline, and clarithromycin for additional antibiotic treatment. The local wound condition and the inflammatory markers, including the erythrocyte sedimentation rate and the C-reactive protein level, were checked regularly at each visit after discharge. The inflammatory markers returned to normal values at 12 weeks after surgery. The antimycobacterial agents were discontinued after the patient had completed a 6-month treatment course. Reconstruction surgery for the calcaneus (e.g., bone-grafting) was not performed because there were no symptoms of instability or pain. The patient wore an ankle-foot orthosis and did not bear weight on the affected foot for the initial 6 weeks postoperatively; he then gradually began to increase weight-bearing activities as tolerated. At 6 months postoperatively, he was able to walk without pain; at 1 year postoperatively, radiographs revealed a stable condition (Figs. 5-A and 5-B). The clinical outcome, based on the American Orthopaedic Foot & Ankle Society score (AOFAS), was evaluated at 1 year postoperatively, and the score was 90 of 100.
Proceed to Discussion >>Reference: Chiu YC, Yang SC, Wu CH, Chuang HW, Tu YK, Ma CH. Mycobacterium abscessus osteomyelitis of the calcaneus presenting as tumor-mimicking lesions: a case report. JBJS Case Connect. 2017 Jul-Sep;7(3):e56.
Heel pain is highly prevalent in the senior population, affecting approximately one-third of people >65 years old. Plantar fasciitis is a common cause of plantar heel pain, especially in patients who spend a great deal of time on their feet. It has been reported that approximately 10% of the running community is affected by this disorder. In general, plantar fasciitis is regarded as a self-limiting condition, and most patients can achieve a satisfactory recovery, regardless of treatment method. However, for people with refractory plantar heel pain, as with our patient, some worrisome conditions (e.g., a tumor or osteomyelitis) should be considered. Our patient had swelling and tenderness of the heel. In addition, the calcaneal squeeze test was positive. Therefore, a calcaneal pathology other than plantar fasciitis was suspected.
The calcaneus is involved in 7% to 8% of all cases of osteomyelitis. Unlike long-bone osteomyelitis, calcaneal osteomyelitis often undergoes an indolent course. Wang et al. reviewed 52 cases of calcaneal osteomyelitis and found that the clinical symptoms were less dramatic than those of long-bone osteomyelitis, blood culture tests were positive in only 41% of cases, routine hematologic tests were unremarkable, and radiographic changes often were delayed. For these reasons, calcaneal osteomyelitis can be difficult to diagnose early. Because our patient was initially misdiagnosed with plantar fasciitis, he had received inadequate treatment.
In the past decades, the incidence of nontuberculous mycobacteria (NTM) infection has markedly increased, but this increase cannot be explained solely because of advances in diagnostic tools. The M. abscessus complex, 1 species of NTM, comprises a group of rapidly growing, multidrug-resistant NTM that exist in soil and water. The M. avium complex is the NTM species that is most commonly responsible for disease; however, M. abscessus complex infections are more difficult to treat because of their drug-resistant characteristics. Lungs, skin, and soft tissue are the most common sites of M. abscessus infection, but M. abscessus can cause disease in almost all organs.
According to recent major studies concerning resistance rates for the M. abscessus complex, resistance rates were relatively low for clarithromycin, cefoxitin, and amikacin. However, doxycycline, quinolones, and imipenem had high resistance rates. The recommended treatment for serious M. abscessus complex disease usually involves an initial combination of a macrolide and intravenous agents for at least 2 weeks, followed by prolonged oral macrolide-based therapy. The drugs of choice for initial intravenous therapy are amikacin plus cefoxitin or imipenem. Tigecycline exhibited low minimum inhibitory concentrations in recent in vitro studies, and should be considered for treating the infection.
Distinguishing between hematogenous osteomyelitis and a bone tumor can be difficult, especially in patients without trauma or local infection. The penumbra sign on MRI, represented as a rim of vascularized granulation tissue around a bone abscess cavity that has a higher T1-weighted signal intensity than the cavity itself, is reported to be highly specific for osteomyelitis, but it was nearly absent in our patient. The surgical findings revealed a soft-tissue mass formation; therefore, a metastatic bone tumor could not be excluded. Hence, obtaining an intraoperative bone culture specimen and histologic examination is crucial for the correct diagnosis.
To the best of our knowledge, there have only been a few similar cases reported in the literature. Elsayed and Read described a unique case of culture-confirmed M. haemophilum osteomyelitis in an adult woman with polycythemia vera. Yi et al. reported a case of NTM calcaneal osteomyelitis in a 51-year-old woman that was initially misdiagnosed as plantar fasciitis. Michelarakis and Varouhaki reported a case of recurrent osteomyelitis in the calcaneus due to an atypical mycobacterial species that was associated with interferon-gamma-receptor deficiency. To our knowledge, our patient represents the first described case of calcaneal osteomyelitis caused by an M. abscessus infection that presented as tumor-mimicking lesions.
There is currently no consensus on guidelines for treating skeletal NTM infections. In our patient, we performed extensive debridement, followed by prolonged antimycobacterial therapy. At 6 months after surgery, the patient was able to walk without pain. Accurate diagnosis is crucial for the prognosis. A physician should keep in mind that refractory heel pain can be caused by NTM infection. Careful history-taking, physical examination, and proper diagnostic tests, including intraoperative culture specimens and histologic examination, are necessary.
Reference: Chiu YC, Yang SC, Wu CH, Chuang HW, Tu YK, Ma CH. Mycobacterium abscessus osteomyelitis of the calcaneus presenting as tumor-mimicking lesions: a case report. JBJS Case Connect. 2017 Jul-Sep;7(3):e56.


What is the diagnosis?
Synovial sarcoma
Epithelioid sarcoma
Mycobacterial infection
Granulomas suggestive of sarcoidosis
Aneurysmal bone cyst