A Four-Year-Old Boy with Headache and Neck Stiffness
November 4, 2009


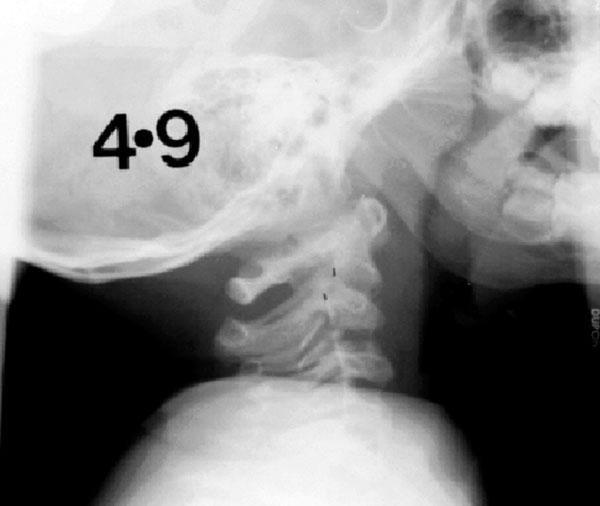
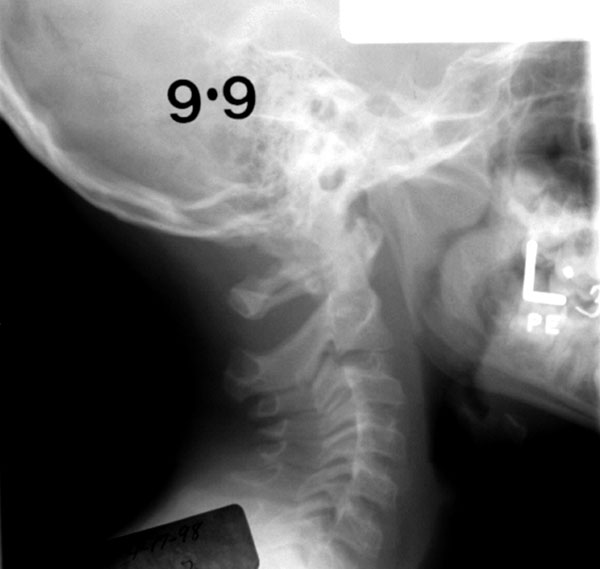
 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 1-C
Fig. 1-C Fig. 1-D
Fig. 1-D Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 1-C
Fig. 1-C Fig. 1-D
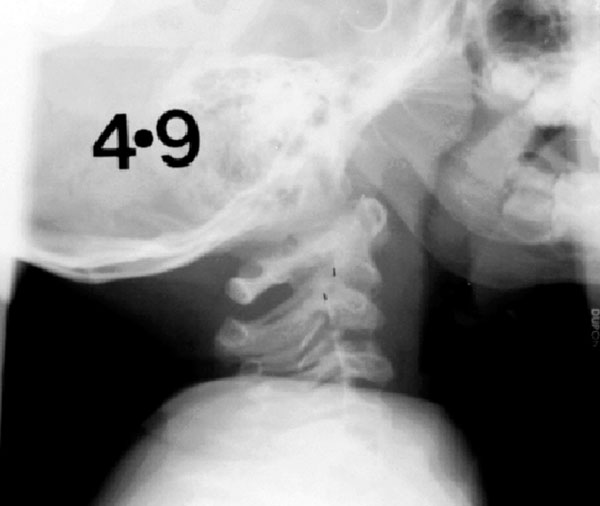
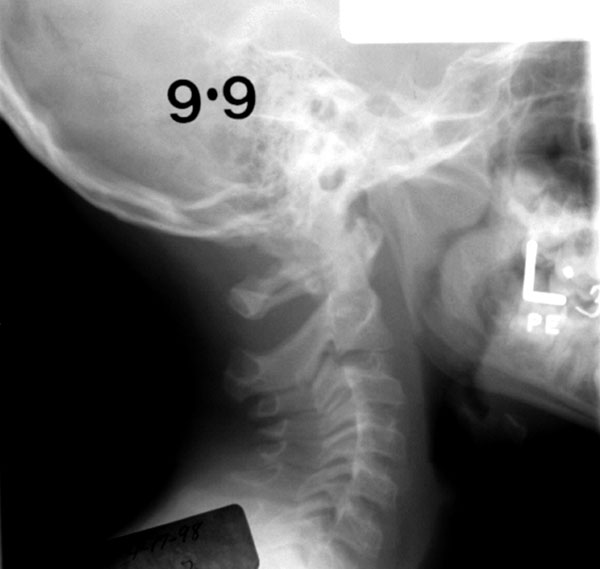
Fig. 1-DIn April 1993, a very active four-year and nine-month-old boy was seen at a hospital in another state because of headache and neck stiffness. No injury was reported at that time. He underwent magnetic resonance imaging of the brain and serum testing for C-reactive protein. The magnetic resonance imaging scan revealed normal findings, and the C-reactive protein level was within normal limits. Two weeks later, he was seen in the emergency department of a local hospital with a very stiff neck. The neurological examination revealed normal findings, as did the radiographic skeletal survey. Cutaneous signs of child abuse were absent. The mother reported that acute neck pain and stiffness had developed in the child two to three weeks earlier. However, for the past year, the boy had experienced short-lasting episodes of intermittent neck pain that spontaneously resolved. A lateral radiograph of the cervical spine was made.
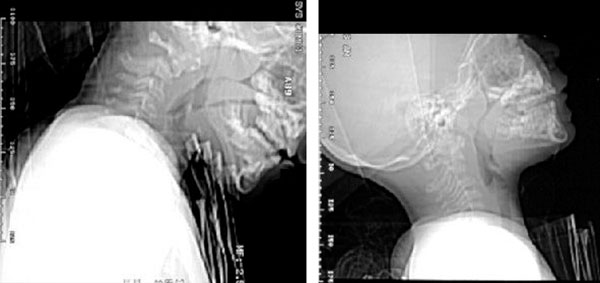
Cervical spine radiographs demonstrated a fracture of the odontoid, with 8 mm of anterior displacement and a severe local kyphotic deformity (Fig. 1-A). Retropharyngeal soft-tissue swelling measured 14 mm at the lower end plate of C2. Computerized tomographic scout images revealed that the fracture reduced with neck extension (Fig. 1-B). The child was hospitalized. With the patient under general anesthesia, a halo connected to a plaster body jacket was applied. Six halo fixation pins were used, with a reduced insertion torque of 4 in-lb. The kyphotic angulation at the fracture site was improved; however, 3 mm of anterior displacement persisted (Fig. 1-C). One month later, one of the metal supports that connected the halo to the cast cracked, and it was replaced. The fracture reduction remained unchanged during the time of halo wear despite a high level of activity and a severe fall from a bicycle. The pin sites became infected three months after the application. The halo cast was removed, and a plaster body jacket with a neck mold was applied for six more weeks. Flexion and extension radiographs that were made four and one-half months after the initial halo treatment demonstrated fracture-healing. Five years later, a cervical spine radiograph demonstrated remodeling at the site of the odontoid fracture (Fig. 1-D). At the age of seventeen years, the boy reportedly experienced occasional neck pain that did not require medication and he continued to be very physically active.
Proceed to Discussion >>Reference: Tavares JO, Frankovitch KF. Odontoid process fracture in children: delayed diagnosis and successful conservative management with a halo cast. A report of two cases. J Bone Joint Surg Am. 2007;89:170-6.
In children, the synchondrosis between the odontoid and the body of the axis is particularly vulnerable to injury, with the average age at the time of the injury being three years. These fractures can result from high-energy trauma as well as from more trivial injuries. The treatment of choice for acute odontoid fractures is conservative management, with reduction by extension of the neck and immobilization in either a Minerva cast or a halo cast or halo brace. There is only one previous report of an established nonunion of the odontoid in a child, a five-year-old boy. The diagnosis had been delayed for four months after the time of injury. The patient underwent a primary posterior C1-C2 fusion. Postoperatively, a deep infection developed, the implant was removed, and the graft resorbed. Nonetheless, the fracture healed after the patient had been placed in a Minerva cast for three months. Seimon reported on a child who had an untreated, undisplaced fracture of the odontoid process. The odontoid fracture gap progressively widened on segmented radiographs, similar to changes seen in association with a nonunion of the carpal scaphoid. Our patient had unstable family conditions and an absence of acknowledged injury, leading to suspicions of child abuse and neglect. He did not have lacerations, scars, or bruises consistent with recent abuse. The caretakers reported that he had had minimal complaints for several months before the onset of acute symptoms. It is possible he could have had a nonunion of the odontoid and then experienced a trivial injury that acutely increased odontoid displacement. There appears to be a critical age at which trauma to the upper cervical spine may result in an os odontoideum. There is no documented case in which an acquired os odontoideum has been reported following a neck injury in a child older than three years of age. The fracture in this patient reduced easily with neck extension as a hinge of periosteum likely existed anteriorly. After reduction, the halo cast was used for immobilization. Because of the decreased thickness of a child's skull, six halo fixation pins were used with a reduced insertion torque of 4 in-lb instead of the four pins at 8 in-lb as used in adults. At the time of treatment, plastic vests for children were not commercially available, so a plaster body jacket was used instead. The fracture appeared to be healed in eight to sixteen weeks, the time expected for acute odontoid fractures.
Reference: Tavares JO, Frankovitch KF. Odontoid process fracture in children: delayed diagnosis and successful conservative management with a halo cast. A report of two cases. J Bone Joint Surg Am. 2007;89:170-6.

Os odontoideum
Fracture of the odontoid process
Rotatory C1-C2 subluxation
Congenital odontoid hypoplasia