A 15-Year-Old Girl with Radiating Pain in the Arm
February 2, 2022
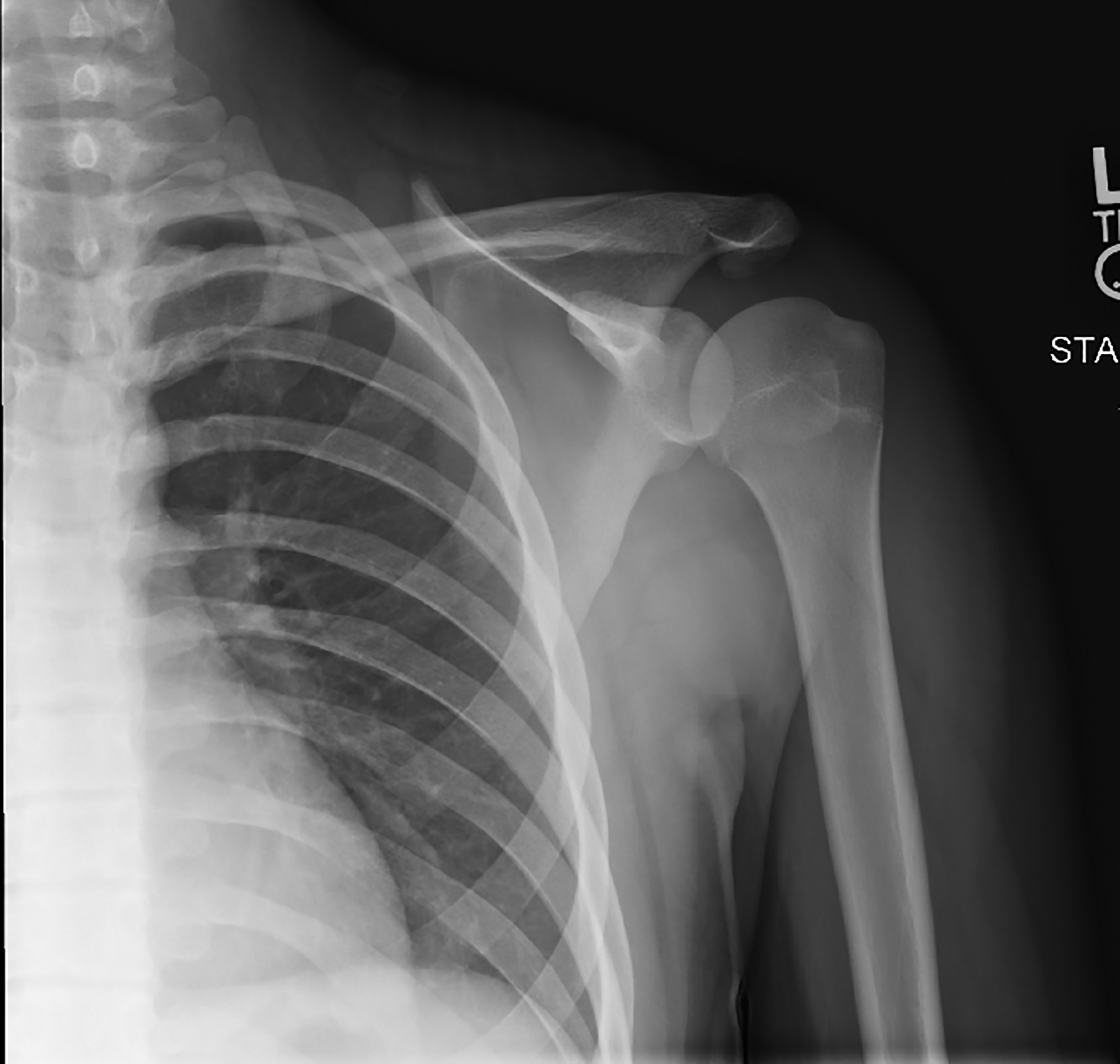
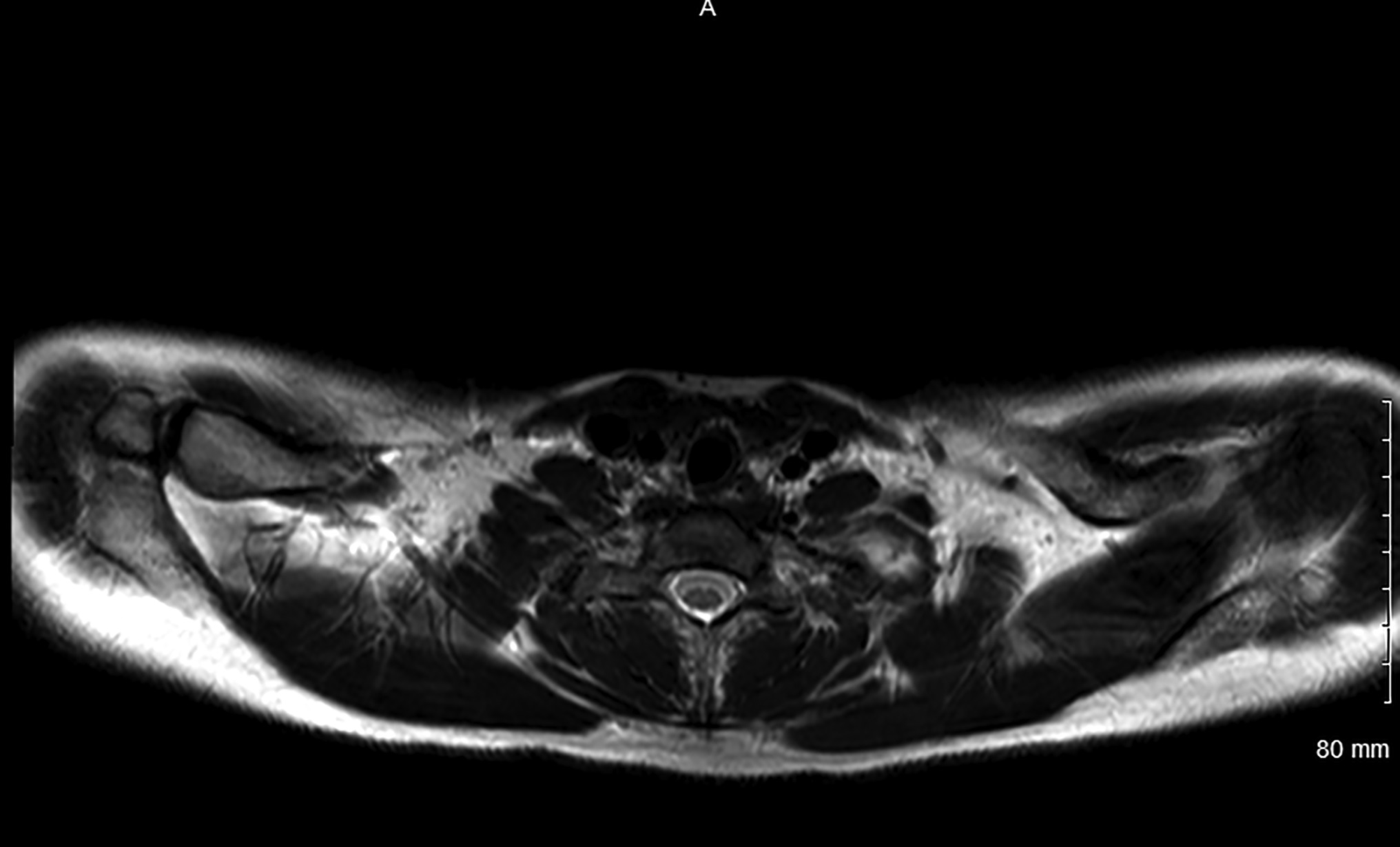
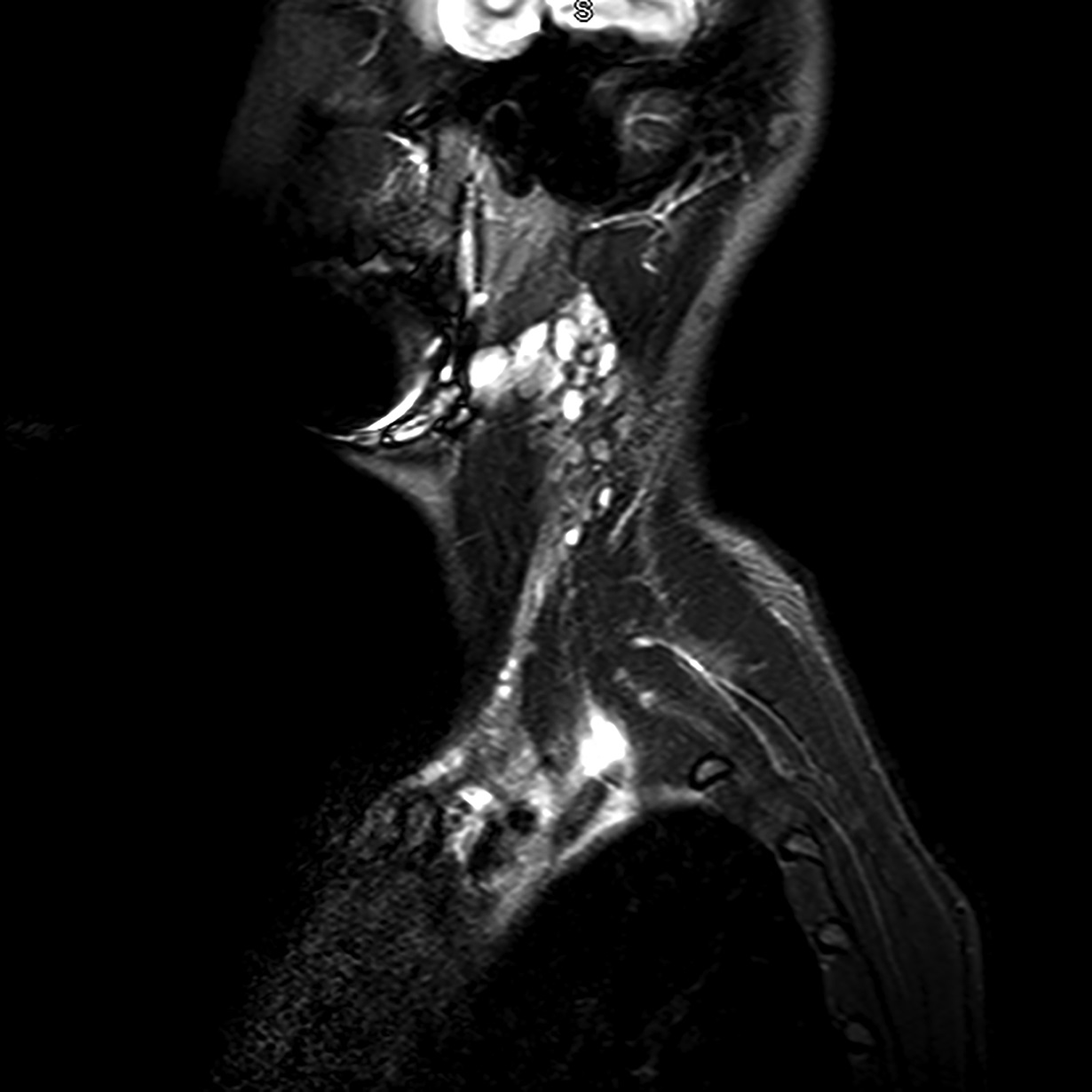
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 3-C
Fig. 3-C Fig. 4
Fig. 4 Fig. 5
Fig. 5A 15-year-old right-hand-dominant female competitive softball player presented 3 days after an injury sustained while playing softball. Although considered a pitcher, she was playing third base at the time of the injury. While she was in a squatting position to tag an opponent sliding into base, the opponent’s helmet directly impacted her left anterior chest wall. To execute the tag, the patient’s arm was placed into a hyperextended position. Immediate left arm pain, paresthesia, and extremity coolness were apparent, and she had deep left subclavicular pain.
Numbness and tingling of the left arm were still present but improving. The patient was then placed into a shoulder immobilizer and was instructed to follow up at the local orthopaedic clinic.
During her initial clinic visit, the patient indicated that she was experiencing pain localized to the left medial scapular border and in the left clavicular region. She also had continued symptoms of mild numbness and tingling of the left arm but noted some improvement in the intensity of the symptoms. On palpation, the clavicle was nontender, but the patient did experience pain deep along the upper ribs superior to the clavicular shaft. The peripheral nerves were intact, and strength and reflexes were considered normal. Full range of motion was observed in both upper extremities, and the patient experienced mild pain with full flexion of the left shoulder. No vascular or neurologic compromise was elicited with provocative testing.
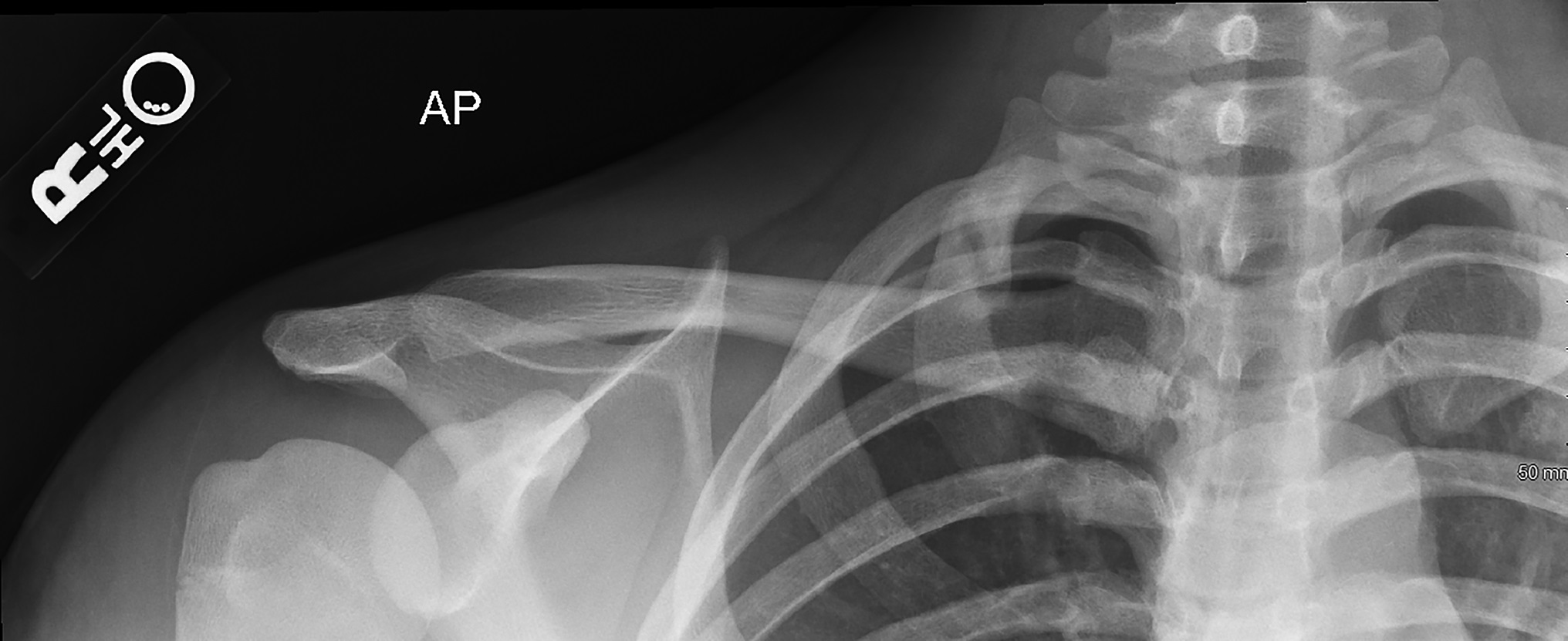
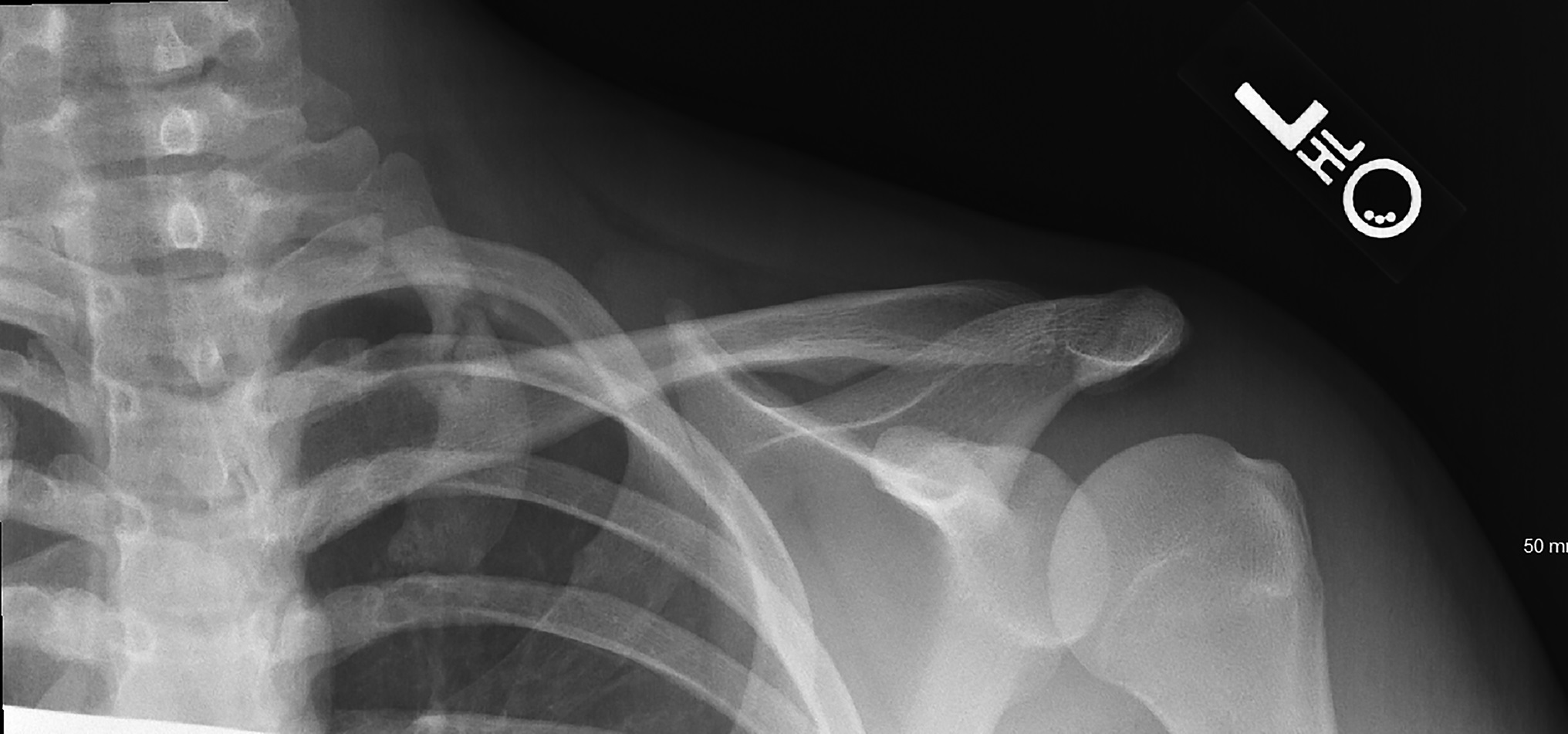
A radiograph from an outside facility is shown in Figure 1. Magnetic resonance imaging (MRI) scans showed increased inflammation to the brachial plexus with hypertrophy and inflammation of all 3 scalene muscles (Figs. 2-A and 2-B).
An anteroposterior radiograph showed a nondisplaced fracture of the middle third of the left first rib and evidence for a mesoacromion. The patient was diagnosed with a nondisplaced fracture of the left first rib.
A sling was prescribed for comfort, and the patient was given anti-inflammatory drugs for pain. The patient was instructed to restrict activities and begin a formal course of physical therapy. A return visit 4 weeks later revealed improved symptoms. Computed tomography (CT), along with repeated radiographs, with comparison views of the contralateral shoulder, revealed bilateral persistent lucency with sclerosis of the middle third of the first rib (Figs. 3-A, 3-B, and 3-C). Radiographs showed fracture healing of the left first rib at 2 months after the injury (Fig. 4). The patient was able to return to full activity and competitive softball at 3 to 4 months after the initial injury and was completely asymptomatic. By 8 months after the injury, the fracture had healed (Fig. 5).
Proceed to Discussion >>Reference: Gibson TW, Carson L. Acute thoracic outlet syndrome associated with congenital pseudarthrosis of the first rib: a case report. JBJS Case Connect. 2021 Jul 30;11(3).e20.00594
The first rib is protected on all sides by the shoulder girdle and the surrounding musculature. Hence, first rib fractures due to direct trauma are rare, and isolated bilateral first rib fractures are extremely rare. A fracture of the first rib usually occurs at the thinnest and weakest anatomical point, which is at the groove for the subclavian artery, also known as the subclavian sulcus. When an injury occurs in this region, the rib is subject to opposing forces of the scalenus anterior and the serratus anterior. A quick and unexpected forceful contraction of the scalene muscle can result in a fracture of the first rib at the subclavian sulcus. Most patients with a first rib fracture present with nonspecific shoulder pain.
The diagnosis of a first rib pseudarthrosis can be determined by radiographs, CT, or MRI. Angiography, CT, or MRI scan is frequently executed to assess patients with presumed thoracic outlet syndrome. Chest radiograph is also usually performed in these patients because it can assist in outlining bone deformities. The etiology of a first rib pseudarthrosis may be related to a congenital condition or secondary to a nonunion after a fracture of the first rib. Nonunions of a first rib fracture may be related to persistent overhead activities after the injury. Fractures or subluxations of the first rib are uncommon, especially in athletes.
Pseudarthrosis of the first rib is typically a painless mass or fullness discovered as an incidental finding. Pseudarthrosis of the first rib is a union formed by fibrous tissue at the fracture site and can be associated with congenital weakening of the bone. Partial dislocations of the first rib may be caused by an underlying congenital condition such as congenital pseudarthrosis.
Fractures of the first rib are stress-induced because of repetitive muscular forces, such as overhead throwing, and typically heal with minimal treatment. In addition, fractures occur because of acute traumatic events with associated pain and other symptoms. Treatment is usually conservative and includes sling immobilization for a short period, pain relievers, and modification of activity. Physical therapy may be used to encourage range of motion. First rib resection with scalenectomy could be performed to resolve pain and improve function in an athlete with nonunion desiring to continue with sports who has not obtained relief with other treatment approaches.
Excessive callus formation at the site of the pseudarthrosis may lead to compressive pathologic conditions such as thoracic outlet syndrome. Whether thoracic outlet syndrome is caused by an acute event such as a first rib fracture or a predisposition from anatomic or congenital anomalies is uncertain. Thoracic outlet syndrome is compression on the nerves or blood vessels in the space between the clavicle and the first rib. Symptoms of thoracic outlet syndrome include numbness, temperature change, or paresthesia of the extremity. It has been documented that thoracic outlet syndrome has been caused by pseudarthrosis of the first and second ribs. The symptoms of this are usually neurologic.
This is a review of a single case to describe and report an acute thoracic outlet syndrome with bilateral first rib pseudarthrosis discovered incidentally during radiographs after a shoulder injury. Based on the clinical information provided, we were unable to determine the actual association of the brachial plexus injury from shoulder hyperextension and how it related to the radiographic finding of the first rib pseudoarthrosis. The goal of this report was to raise awareness of this very uncommon radiographic finding. It is obvious from the follow-up radiographs that there was an acute injury to the first rib based on the presence of fracture callus during the follow-up. The MRI findings suggested an acute event surrounding the brachial plexus. We recommend a high suspicion of bilateral first rib pseudarthrosis in a throwing athlete with acute thoracic outlet symptoms when a forced hyperextension mechanism of injury is present. Of note, a predisposition of thoracic outlet syndrome may be present in this patient population. Fortunately, these symptoms resolve with conservative care, and return to sports is typical.
Unlike previously reported cases, the patient described in this report had sustained trauma to the extremity. In addition, previously reported patients had a gradual onset of pain in the upper extremities from repetitive movement. Pseudarthrosis of the first rib has been rarely reported to be symptomatic. These pseudarthroses seem to be a common incidental finding that should not be mistaken for pathology in imaging after trauma. Our patient was unique in that the bilateral pseudoarthrosis of the first rib may not have been discovered without the traumatic injury and subsequent workup.
Reference: Gibson TW, Carson L. Acute thoracic outlet syndrome associated with congenital pseudarthrosis of the first rib: a case report. JBJS Case Connect. 2021 Jul 30;11(3).e20.00594


What is the diagnosis?
Torn rotator cuff
Acromioclavicular joint dislocation
Calcified supraspinatus tendinitis
Nondisplaced fracture of the left first rib
Hill-Sachs lesion suggestive of prior anterior dislocation