
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4A 23-year-old, Olympic-level, male gymnast presented with the insidious onset of activity-related wrist pain over several weeks. He had recently increased the intensity and duration of his workouts in preparation for a major competition. The pain that he experienced was most severe when he was weight-bearing on the hands while participating in various gymnastics disciplines. This was most noticeable with his primary event, the pommel horse. He had no symptoms at rest or with non-weight-bearing activities of daily living.
There was no notable soft-tissue swelling, deformity, or ecchymosis. Tenderness to palpation was localized about the base of the second metacarpal. Palpation reproduced the symptoms that the patient was experiencing. A vitamin D level obtained at this time was within the normal range at 43 nanograms per milliliter.
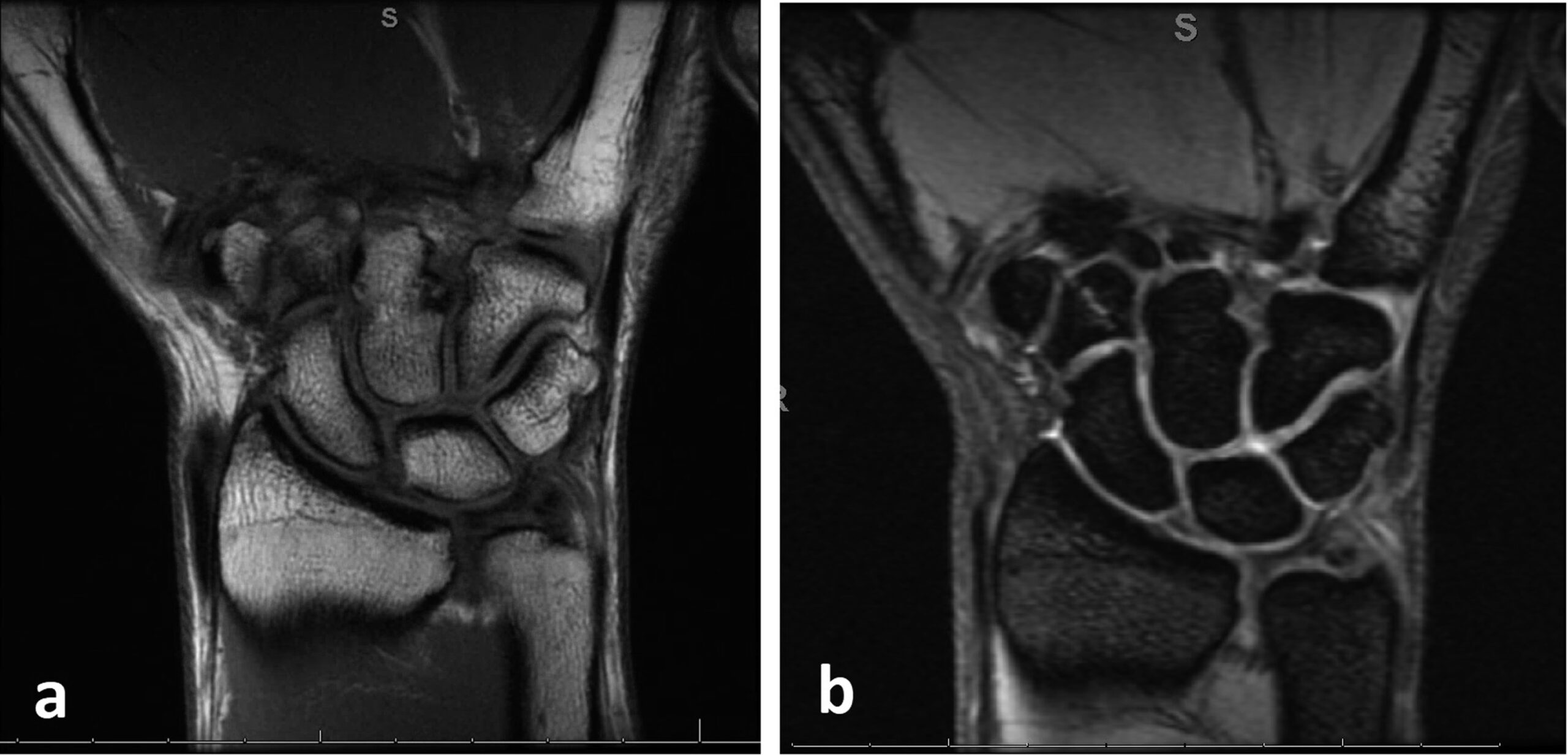
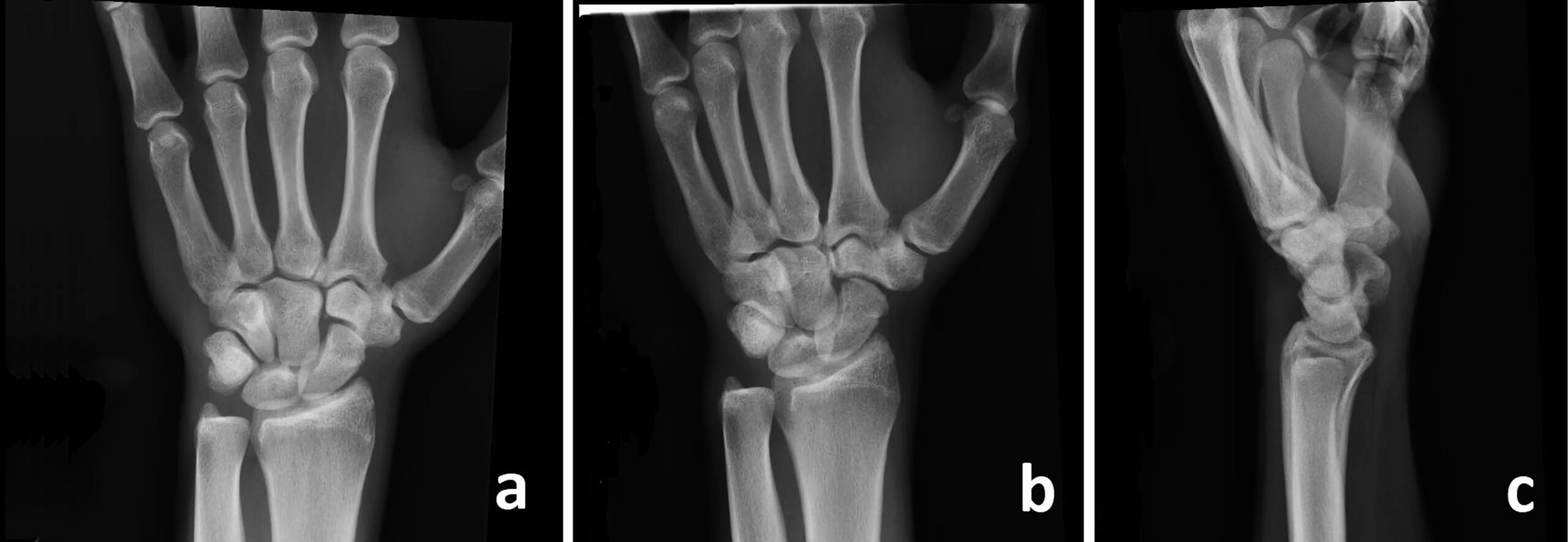
Radiographs of the left wrist (Fig. 1) demonstrated normal alignment and bone mineralization. There was no fracture, abnormal periosteal reaction, or notable carpal boss. There was evidence of sclerosis, best visualized on the scaphoid view (Fig. 1-D). A subsequent magnetic resonance imaging (MRI) scan revealed a linear band of a low-intensity signal on a T1-weighted MRI sequence and of a high-intensity signal on a T2-weighted MRI sequence (Fig. 2).
The sclerosis of the trapezoid on radiographs, along with the linear band of a low-intensity signal on a T1-weighted MRI sequence and of a high-intensity signal on a T2-weighted MRI sequence, was diagnostic of a stress fracture of the trapezoid.
Given the radiographic findings, along with the patient’s history and clinical examination, we placed the patient into a thumb spica cast for immobilization and required the patient to stop all activities involving the left upper limb to begin treatment of the trapezoid stress fracture. The cast was removed at 4 weeks. Repeat radiographs demonstrated the presence of increased bony sclerosis of the trapezoid (Fig. 3). This radiographic finding, commonly visualized as stress fractures heal, was reassuring. The patient no longer had any tenderness over the trapezoid.
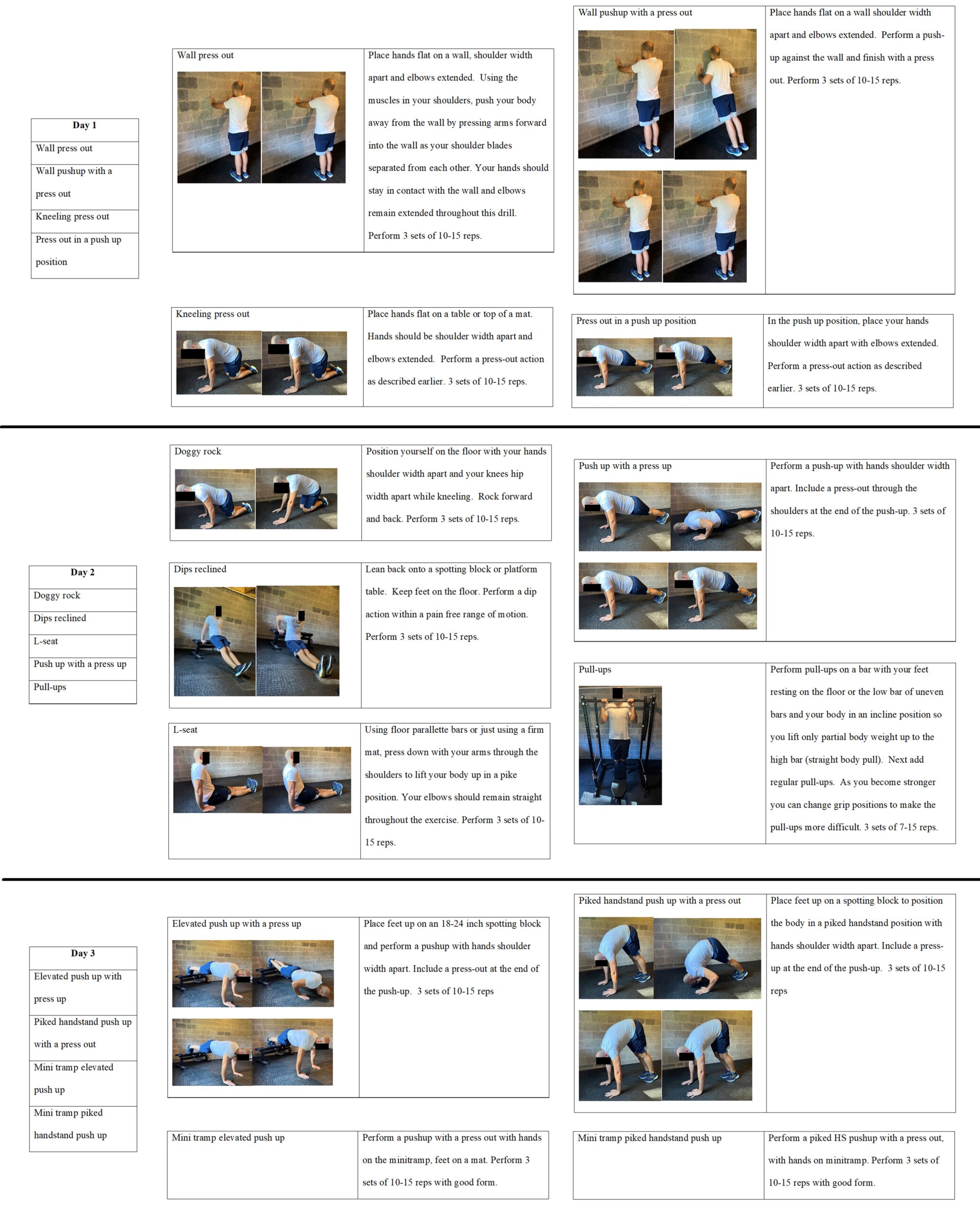
A return-to-sport protocol was initiated at 1 week after removing the cast. The initial emphasis was on progressive weight-bearing to approach the anticipated increased strain from the full weight-bearing required to perform high-level gymnastics disciplines. The patient completed the weight-bearing progression over 3 days (Fig. 4). He then advanced to a return-to-participation protocol, which included a 4-week course of increased gymnastic activity on the pommel horse, parallel bars, and rings, along with a progression through strengthening exercises. This exercise regimen included scissors and pommel circles and then progressed to advanced techniques, including the Kehr position. As the patient progressed through the protocol, he gradually transitioned with skill work from plastic handles to leather.
The patient returned to full gymnastic activities without limitations at 3 months after initiating nonoperative treatment. He reported no pain with activity and had no tenderness over the trapezoid. At the final follow-up at 6 months after presentation, he performed all gymnastic activities without symptoms.
Proceed to Discussion >>Reference: Bertha NM, Wisinski JJ, Taylor KF. Trapezoid stress fracture in an Olympic-level gymnast: a case report. JBJS Case Connect. 2023 Mar 16;13(1):e22.00626.
The differential diagnosis for patients presenting with pain near the base of the second metacarpal is broad. It must include insertional tendonitis, carpal bossing, metacarpal fracture, carpal fractures, and less common stress fractures of the metacarpal or carpal bones. Metacarpal stress fractures have been described in racquet sports. It is believed that the second metacarpal has the highest force generated across it because it is the longest metacarpal and has the largest base. Scaphoid stress fractures and distal radial epiphysiolysis have also been described and need to be considered in the differential diagnosis in patients presenting with pain about the radial wrist.
The patient’s particular sport and activity level played a large role in sustaining a trapezoid stress fracture. This patient had multiple protective factors against stress fractures, including age, male sex, and normal vitamin D level. The only identifiable risk factor of stress fracture was the increase in repetitive weight-bearing activity. Gymnasts, particularly at the elite level, participate in long hours of practice daily and have high rates of injury. Despite strict adherence to proper form, the rates of injury in gymnasts tend to increase at higher levels of competition because of the intensity of training. Trapezoid fractures occur through an axial load through the second metacarpal with or without forced wrist flexion and extension. The performance of gymnastic activities can generate forces up to 16 times the body weight and can increase the risk of injuries such as a trapezoid fracture. The pommel horse particularly involves abrupt changes in the wrist position during weight-bearing. These excessive loads across the wrist occur in the setting of a firm and rigid pommel where the forces generated occur with the wrist in extreme ranges of motion and place the athlete at an increased risk of injury. Increased duration and intensity of training, with associated forces on the weight-bearing wrist, resulted in the stress reaction seen.
For treatment, other reports of both acute fractures and stress fractures have focused on nonoperative treatment and have kept patients immobilized for a period. There are limited return-to-training protocols available for gymnasts, but, of those available, the focus has been on slowly increasing activities in each discipline over a course of 8 to 10 weeks. Gymnastics is relatively unique, in that rehabilitation requires weight-bearing progression in the upper extremities. In general, the weight-bearing progression ranges from starting in a quadruped position and then progressing into a push-up position and, finally, through a progression of handstands. We believe that our protocol used for this patient was able to allow him to return to his sport in a safe and efficient manner.
When encountering a patient with pain at the base of the index finger metacarpal, particularly in patients who are engaging in activities placing large physiologic load on the carpal bones, providers must consider trapezoid stress fractures in their differential. In our experience, these patients can be managed nonoperatively with a graduated return to sport with excellent outcomes.
Reference: Bertha NM, Wisinski JJ, Taylor KF. Trapezoid stress fracture in an Olympic-level gymnast: a case report. JBJS Case Connect. 2023 Mar 16;13(1):e22.00626.
What is the diagnosis?
Kienbock’s disease
Stress fracture of the scaphoid
Stress fracture of the base of the second metacarpal
Stress fracture of the trapezoid
Osteonecrosis of the scaphoid