
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-BA 37-year-old man presented to the orthopaedic oncology clinic reporting a mobile right knee mass over the anteromedial knee. Per the patient, the mass had been present for at least 2 decades. He noted occasional swelling and pain in the knee and associated popping and clicking in the knee. He had a remote history of 2 mild hyperextension injuries to the knee, but otherwise noted no severe trauma. On physical examination, he had a full arc of motion of the knee. He had a 1+ effusion and a palpable, mobile, 3-cm mass medial to the patellar tendon. He was noted to have substantial tenderness to palpation along the lateral border of the patella as well. The knee was stable on ligamentous stress testing. Radiographs taken at that time demonstrated no osseous abnormality but did show a joint effusion.
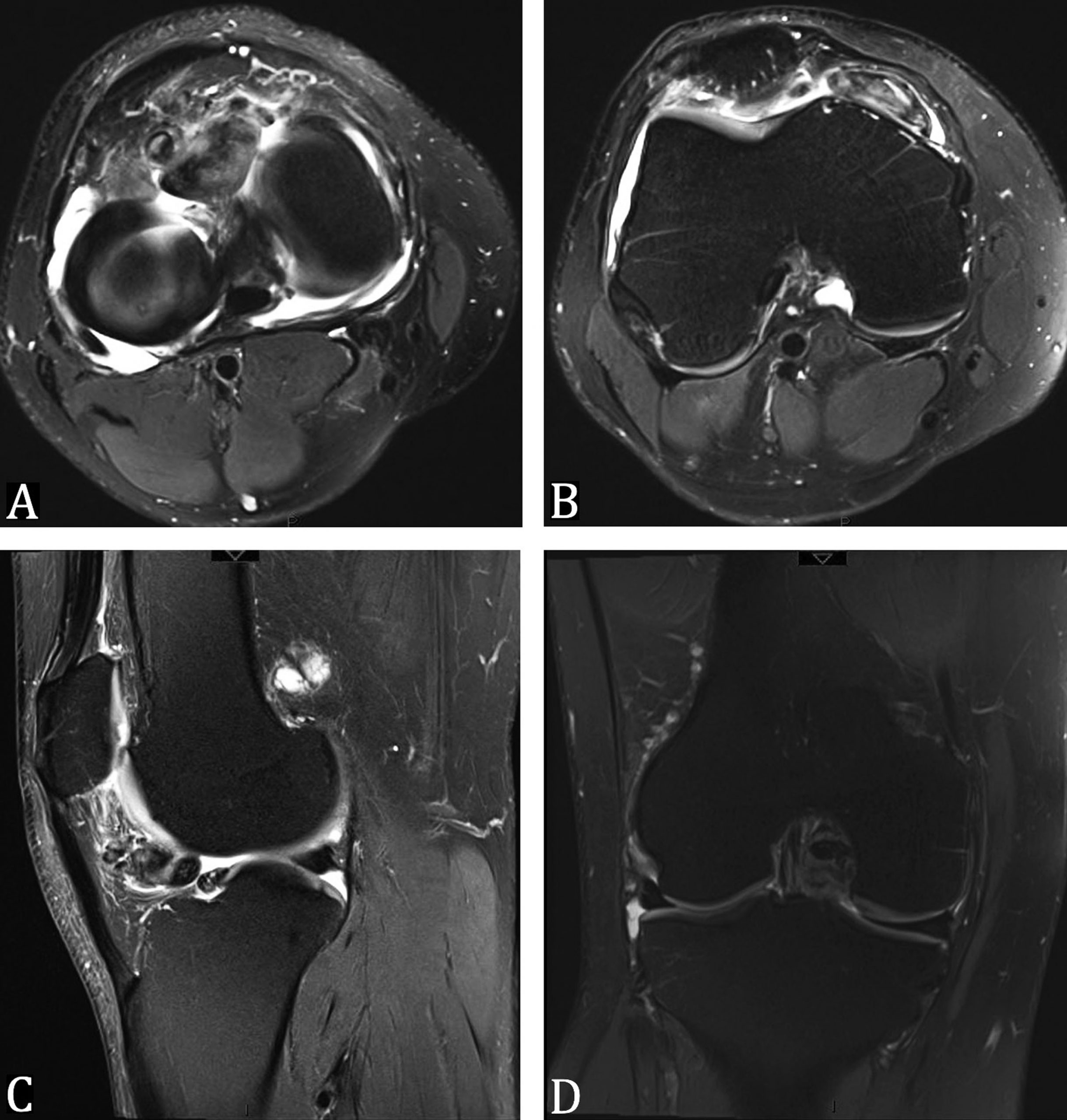
Magnetic resonance imaging (MRI) was obtained, which did demonstrate proliferative synovitis involving the infrapatellar region and femoral notch (Fig. 1). The patient was offered surgical treatment in the form of arthroscopic resection. Informed consent was obtained. Intraoperatively, there were at least 11 discrete lesions encountered in the lateral gutter, femoral notch, and Hoffa fat pad (Fig. 2). These were able to be debrided using the standard inferomedial and inferolateral portals.
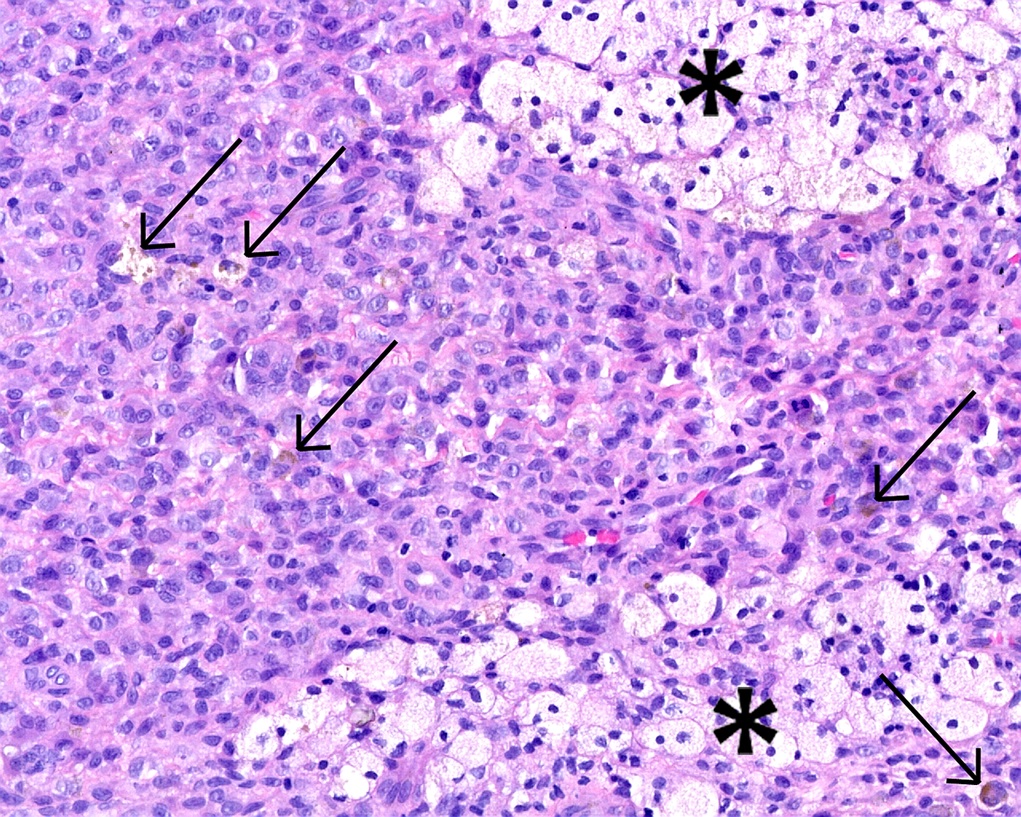
The histopathologic analysis of the debrided specimens confirmed benign, multifocal, localized tenosynovial giant cell tumor (LTSGCT) with areas of healthy, normal synovium (Figs. 3-A and 3-B).
Postoperatively, the patient was allowed to bear weight as tolerated on the involved leg. His postoperative course was uncomplicated, and, at his most recent follow-up at 2 years postoperatively, he had regained full motion in the knee and had no limitations in his activity.
Proceed to Discussion >>Reference: Tedesco AJ, Tedesco NS. Monoarticular, multifocal, localized tenosynovial giant cell tumor of the knee: a case report. JBJS Case Connect. 2020 Jan-Mar;10(1):e0479.
Being able to differentiate between the diffuse and localized forms of TSGCT is paramount to give patients a realistic outlook on future prognosis and chance of recurrence, as well as plan for the optimal treatment course. This particular case presents a unique challenge in that it does not quite fit in either the localized category or the diffuse category. Most synovium in the knee was healthy and unaffected, which is generally not the case for the diffuse form. In addition, the synovium lacked the characteristic villous, hyperemic proliferation of the affected areas typically seen in diffuse TSGCT (DTSGCT, formerly termed “pigmented villonodular synovitis”). However, there were multiple discrete nodules in multiple different areas of the synovium, which is unusual for the localized form. To our knowledge, this is the first such intra-articular case of this presentation in the literature.
There have been previous reports in the literature of the multifocal, localized form. However, to our knowledge, none of those reports have described multiple discrete lesions in multiple compartments of the same joint. Rather, they described either polyarticular involvement, multifocal disease along a tendon, or combined intracompartmental and extracompartmental LTSGCT. Yamashita et al. presented a case of a 14-year-old adolescent girl who was found to have LTSGCT involving the anteromedial compartment of the knee joint and extra-articular TSGCT in the same knee along the surface of the deep medial collateral ligament. She was treated with both arthroscopic and open synovectomies and did have one episode of recurrence inside a 2-year follow-up period. Other concurrent intra-articular and extra-articular lesions have been reported, and the extra-articular lesions occur around the same joint as the intra-articular foci. Gao et al. presented a case of a 37-year-old woman who was treated for florid DTSGCT, which affected most of the knee synovium. She was also found to have discrete lesions with extension into the patella and extra-articularly in the popliteal fossa. She was treated with combined open and arthroscopic resection as well and had not experienced any recurrence at the 1-year follow-up.
It is generally accepted that LTSGCT responds well to arthroscopic partial synovectomy, whereas DTSGCT has had mixed results with arthroscopic resection alone. Moskovich et al. reviewed 9 patients who underwent arthroscopic resection of LTSGCT lesions and experienced no recurrence at 48 months after surgery. Similarly, Kim et al. reviewed a series of 11 patients with LTSGCT treated with arthroscopic partial synovectomy alone and did not have any evidence of recurrence in any patient at the minimum 2-year follow-up. Shekhar et al. presented a series of 10 patients treated for LTSGCT affecting the posterior compartment of the knee and showed good success with arthroscopic resection alone. At 23 months, no patient had experienced any signs of recurrence.
Conversely, DTSGCT lesions treated with arthroscopic resection have not had the same universal success. Ogilvie-Harris et al. described 20 cases of DTSGCT treated with arthroscopic synovectomy. They had 11 patients who were treated with complete synovectomy and 9 who were treated with partial synovectomy. There was recurrence found in 5 of the 9 patients who had undergone partial synovectomy and only 1 of the 11 patients who had undergone complete synovectomy. The authors concluded that arthroscopic treatment alone for DTSGCT can be successful but requires extensive, complete synovectomy, often requiring multiple accessory portals. De Ponti et al. had similar results in a series of 15 patients with DTSGCT treated with arthroscopic resection. Half of the patients treated with partial synovectomy experienced recurrence under 2 years of treatment, but 80% of the total synovectomy group was symptom-free at 2 years.
In reviewing the literature on arthroscopic treatment of DTSGCT lesions, it is clear that complete synovectomy is the preferred method to prevent recurrence. The question then becomes how to manage patients like the one presented in this study. Each of the discrete lesions had the appearance of the typical, pedunculated, lobular lesions associated with LTSGCT. However, multiple different compartments of the knee were affected, similar to that seen with the diffuse form. In this patient’s case, the remainder of the synovium was unaffected and healthy in appearance, which is generally not the case for DTSGCT. Continued monitoring of this patient for recurrence will be required given the paucity of information on the natural history of this rare presentation. In the interim, at 2 years of follow-up, it does seem that arthroscopic partial synovectomy of each of the tumor foci appears to be adequate. Although the multiple foci may have appeared to demonstrate more aggressive behavior, treatment and outcome seem to mimic isolated LTSGCT.
TSGCT is a rare condition of the synovium that can be difficult to treat and does carry some risk of recurrence, dependent on the form of TSGCT. This study presents a unique case of uniarticular, multifocal, localized TSGCT that was treated successfully with arthroscopic partial synovectomy. The patient experienced pain relief and had no signs of recurrence at the 2-year follow-up. Continued monitoring of this patient going forward will be required and can provide clinicians with the ability to present more realistic prognostic data and plan surgery more appropriately for patients who do not exactly fit into either the localized or diffuse forms of TSGCT.
Reference: Tedesco AJ, Tedesco NS. Monoarticular, multifocal, localized tenosynovial giant cell tumor of the knee: a case report. JBJS Case Connect. 2020 Jan-Mar;10(1):e0479.

What is the diagnosis?
Multifocal, localized tenosynovial giant cell tumor
Intra-articular Langerhans cell granuloma
Intra-articular synovial sarcoma
Granulomatous inflammation suggestive of mycobacterial or fungal infection
Synovial involvement by chondroblastoma