A 52-Year-Old Man with Sharp Hip Pain After a Fall
December 2, 2020


 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
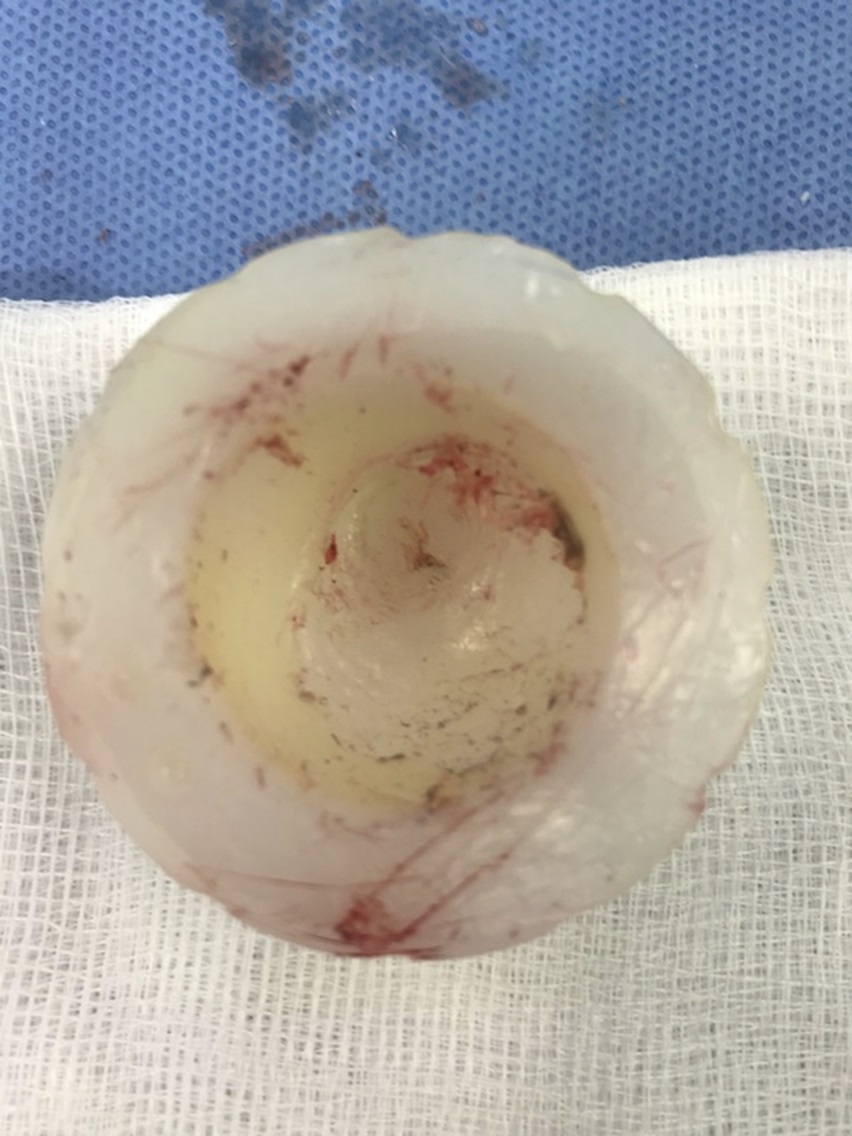
Fig. 5 Fig. 6
Fig. 6A 52-year-old fit and well man with a body mass index of 26 kg/m2 and no medical history underwent right total hip replacement for primary osteoarthritis. Postoperatively, he had an uncomplicated recovery, mobilizing on day 1 and being discharged on day 2, independent on 2 elbow crutches. He was reviewed in the clinic at 6 weeks by the consultant orthopaedic surgeon who performed the operation. At that time, he was mobilizing with relief from pain and unaided and had returned to driving. He had a good range of movement at the hip and had no evidence of a Trendelenburg gait. Radiographs were taken at the time, which showed satisfactory positioning of all implants and equal leg lengths.
At 8 months following the primary surgical procedure, the patient slipped on black ice and fell heavily onto the right hip (trochanteric region). He was able to mobilize immediately afterward while experiencing only minimal pain. He was rereviewed by the operating orthopaedic surgeon within 1 week, and radiographs were taken, which were unremarkable (Fig. 1). The patient returned to normal activities soon after as he experienced pain relief. However, 1 month later, he noticed a sudden sharp pain and a sensation of grinding in the right hip following swimming. He was unable to bear weight and presented to the emergency department.
On examination in the emergency department, the patient had a well-healed posterior approach scar. There was no evidence of infection. He had tenderness to palpation of the groin. Passive and active ranges of movement were unrestricted, and the patient had some pain at 90° of passive hip flexion. He did not experience pain with internal and external rotations, but the examiner noticed palpable crepitus. Blood levels, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), were within normal limits. A radiograph of the hip is shown in Figure 2.
The patient was diagnosed with a fracture of the ceramic femoral head.
The introduction of ceramic bearing components (either ceramic-on-polyethylene or ceramic-on-ceramic) promised the benefit of superior wear characteristics compared with metal-on-polyethylene bearing surfaces in total hip arthroplasty (THA), with the intention of improving joint replacement survival rates in young and active patients.
Fractures of ceramic components used in THA have been reported since their introduction over 40 years ago, but progressive modifications of the material have been associated with fewer fractures. The fourth and most recent version of the CeramTec, BIOLOX delta femoral head has been optimized with zirconia, strontium oxide, and chromium oxide to diffuse crack energy, limit crack propagation, and improve hardness. This is thought to have reduced the incidence of ceramic head fractures.
Following informed consent regarding the challenges of revising a ceramic femoral head fracture, the patient underwent revision to a ceramic-on-ceramic articulation. Upon visualization at the time of revision surgical procedure, the femoral head was found to be in 4 main fragments and multiple smaller fragments (Fig. 3). A thorough synovectomy was performed, and all visible fragments of debris were removed along with the polyethylene liner, which was substantially damaged (Fig. 4). The metal shell was well fixed with no internal damage and therefore retained. There was visible damage to the trunnion (Fig. 5) with associated metallosis, and therefore, a cement-in-cement revision was performed using a new 50-mm offset, no. 1 Exeter stem. A 32-mm internal diameter ceramic BIOLOX liner was inserted along with a new 32-mm BIOLOX delta ceramic head applied to the new femoral stem.
The patient made a full recovery and was mobilizing unaided at the 6-week clinic follow-up appointment. Radiographs of the revised hip were satisfactory (Fig. 6). At the 1-year follow-up, the patient was doing well with full restoration of preoperative function and pain relief.
Proceed to Discussion >>Reference: Rankin CS, Robinson PG, Beattie N, Gaston P. Fracture of a BIOLOX delta ceramic femoral head: a case report and update of the literature. JBJS Case Connect. 2019 Dec;9(4):e0336.
Ceramic-on-polyethylene total hip replacements have shown excellent survivorship and wear rates, particularly for younger patient cohorts and patients with smaller femoral head sizes. However, fractures of the ceramic head are a feared complication because of mandatory revision surgical procedures and the high rates of failure of revision surgical procedures secondary to third body wear. Rates of fractures with previous generations of ceramic heads have been described as 0.1% in a recent review of the literature. However, there have been few reports in the literature regarding fourth-generation BIOLOX delta ceramic head fractures.
Although the rate of fractures of fourth-generation ceramic femoral heads seems to have reduced compared with previous generations, this risk of fracture is still present despite strengthening of the alumina with zirconia, strontium oxide, and chromium oxide. Crack initiation in ceramic is the process by which cracks form on the surface of the material if stresses exceed the tensile strength of the material. Propagation of the cracks can occur and can ultimately lead to fracture. The resistance of the material to withstand almost simultaneous occurrence of crack initiation, propagation, and fracture secondary to trauma is known as the burst strength.
It cannot be proven what the cause of the fracture was in our reported case. However, we believe that the delayed presentation following previous trauma was secondary to the slow crack growth hypothesis. Most cases of fractured ceramic occur when a stress from trauma immediately exceeds the ceramic’s burst strength threshold and catastrophic failure occurs. However, the hypothesis of slow crack growth or subcritical crack growth has previously been documented in the biomaterial and dental literature. When water molecules interact with a crack tip that is under stress and the subsequent chemical reaction between ceramic and water breaks, the metal oxide bonds. The resultant hydroxides allow the crack to grow slowly until it reaches a critical size for fracture (for a given applied stress), which leads to failure. This hypothesis could also explain a previous case report of fourth-generation ceramic head fracture, which occurred in a patient at 2 months after a fall.
There was evidence of black marking on both the internal taper of the ceramic head and the femoral neck taper. This may be secondary to corrosion or metal transfer. The black marking did not cover the entire circumference of the ceramic head (Fig. 3) or the femoral neck (Fig. 5). These findings may suggest that there was nonuniform loading at the head-neck interface, and this may have been a cause for the crack initiation. Unfortunately, we did not have access to fractographic analysis facilities to further analyze the components. An atraumatic fracture of a BIOLOX delta ceramic head was reported in the literature; the authors of that study reported that the manufacturers could find no cause for the fracture and suggested that there may have been debris at the head-neck interface. Nonuniform loading due to contamination of blood or bone at the head-neck interface has been shown to reduce the resistance of ceramic heads to fracture.
This unusual presentation does raise the question as to how best to follow patients who have sustained trauma to the hip replacement with a ceramic head in situ. One retrospective case-control study that assessed risk factors for ceramic liner fractures reported that 80.7% of patients with diagnosed fractures had previously had documented noise at follow-up compared with only 6.1% in the non-fracture group. It is likely that delayed presentation could lead to greater head fragmentation, more extensive metallosis, and potentially poorer results following a revision surgical procedure. A recent study reported the detection of two fractures of ceramic liners not detectable on radiograph, which were subsequently detected on computed tomography (CT) without the use of conventional bone windowing; the authors described the need for an increase in the standard window level to 2,500 Hounsfield units (HU) and the width to 7,000 HU.
In summary, this case demonstrates the requirement for the close follow-up of patients sustaining trauma to fourth-generation ceramic head THAs despite the implants’ new strengthened properties. There are now 2 reports, including this one, of possible delayed fracture following trauma. An understanding of the process of slow crack growth may help to guide arthroplasty surgeons in their assessment and investigation of patients presenting with pain and reduced mobility in the context of ceramic hip components. Furthermore, discussion with musculoskeletal radiologists regarding custom settings during CT may be of benefit for the detection of undisplaced ceramic implant fractures.
Reference: Rankin CS, Robinson PG, Beattie N, Gaston P. Fracture of a BIOLOX delta ceramic femoral head: a case report and update of the literature. JBJS Case Connect. 2019 Dec;9(4):e0336.



What is the diagnosis?
Fracture of a ceramic femoral head
Dissociation of the metal femoral head from the trunnion
Fracture of the trunnion, likely related to corrosion
Trunnion with a bird-beak appearance due to corrosion and toggling of the femoral head
Fractured ceramic acetabular insert of ceramic-ceramic arthroplasty