A 75-Year-Old Man with Leg Pain Exacerbated by a Fall
October 5, 2022
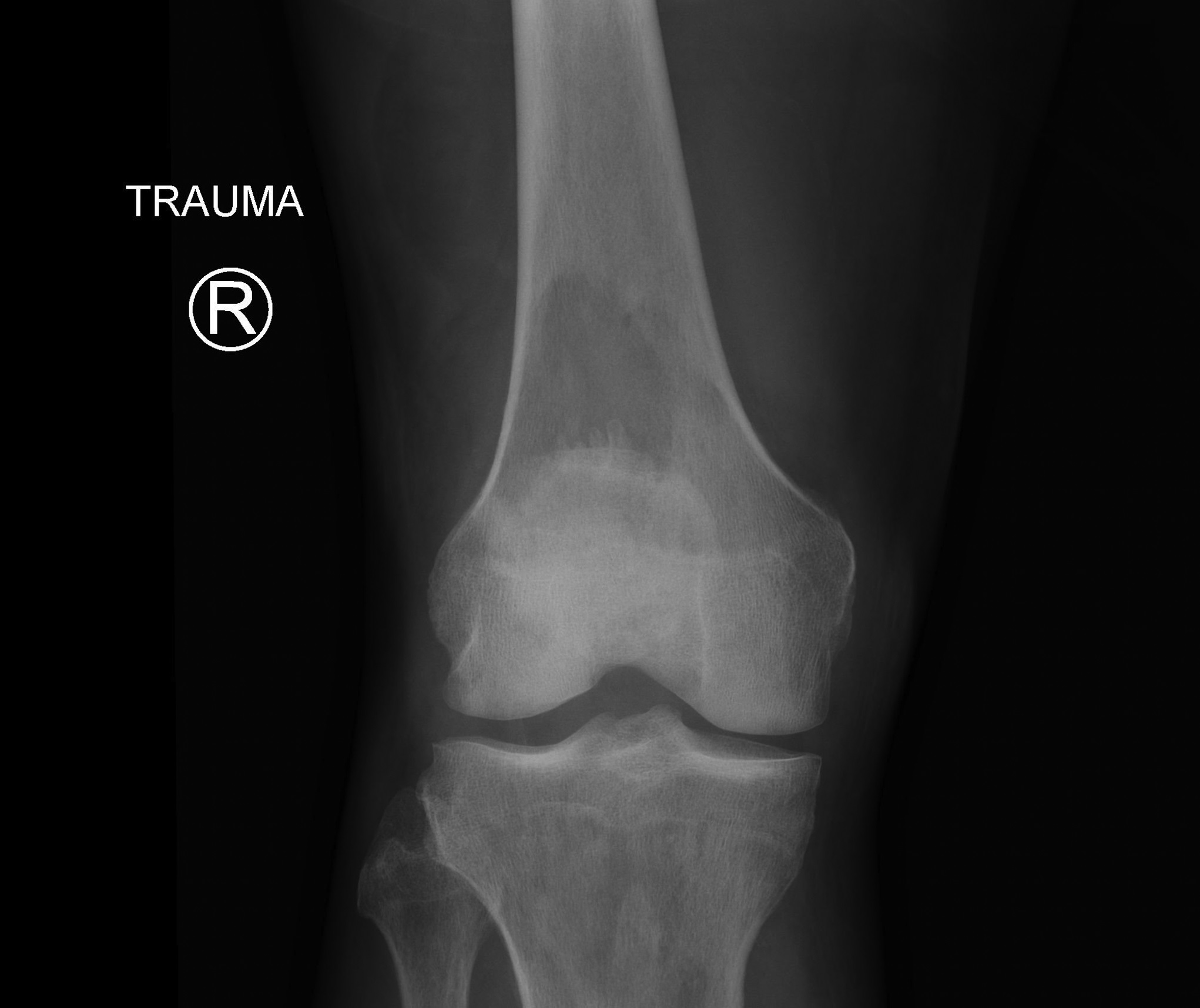

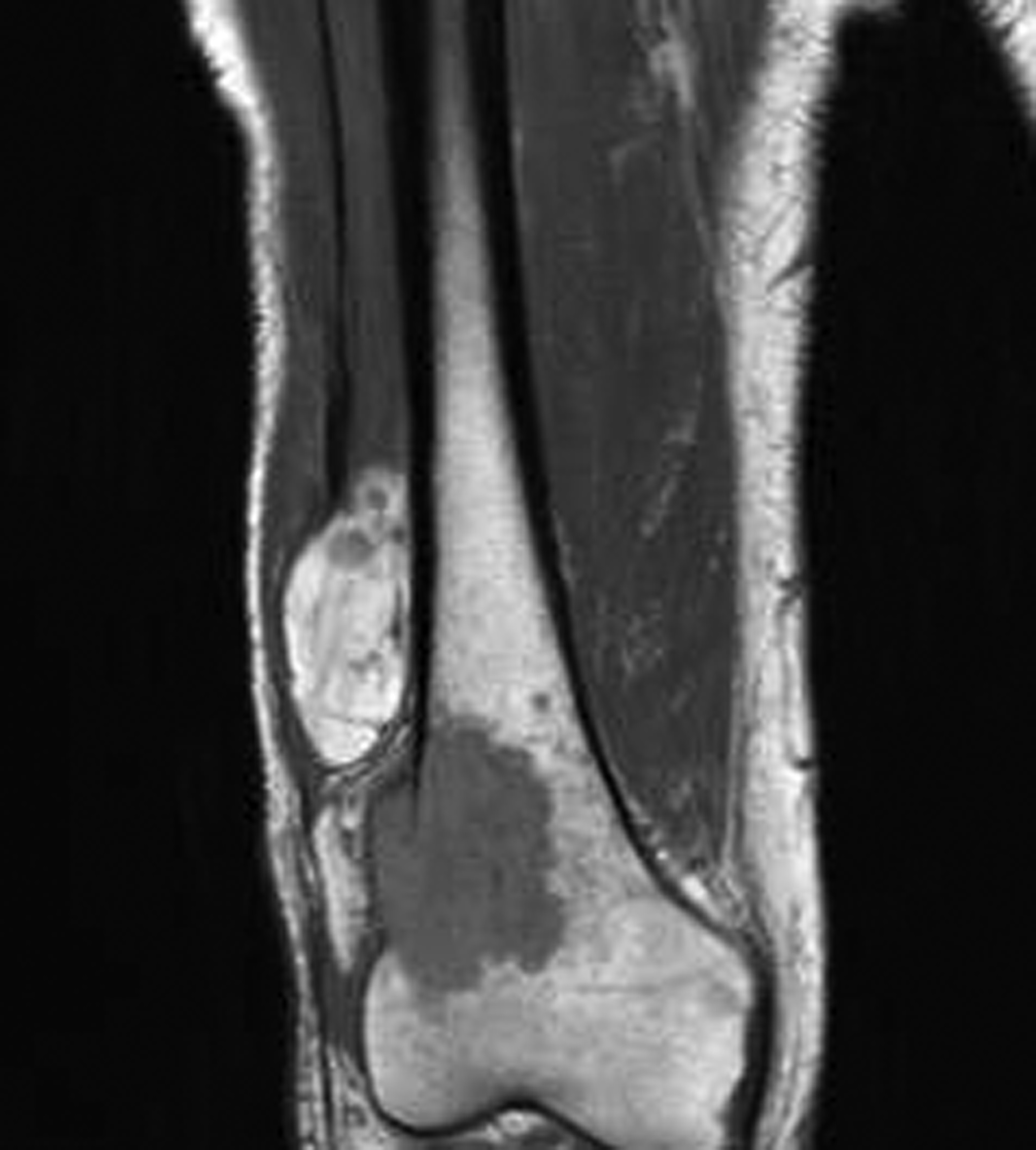
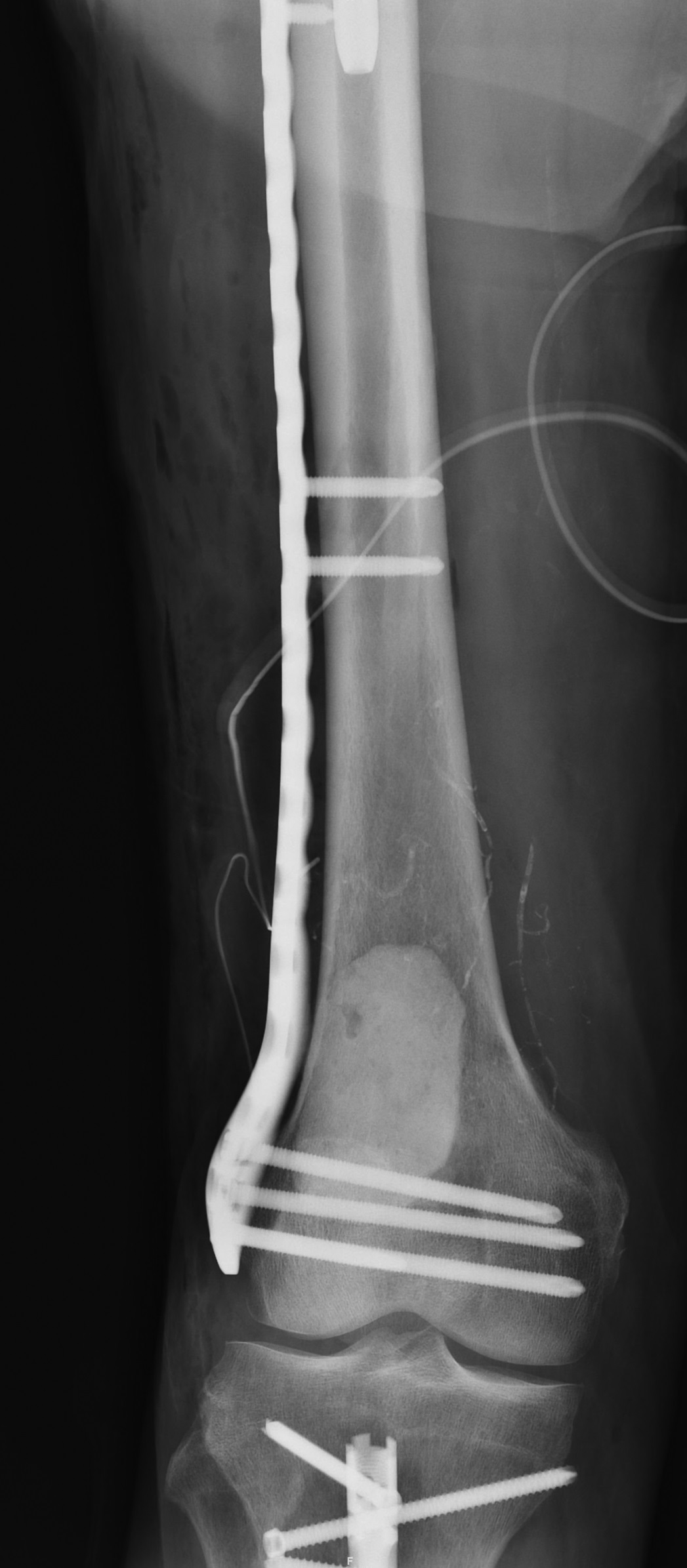



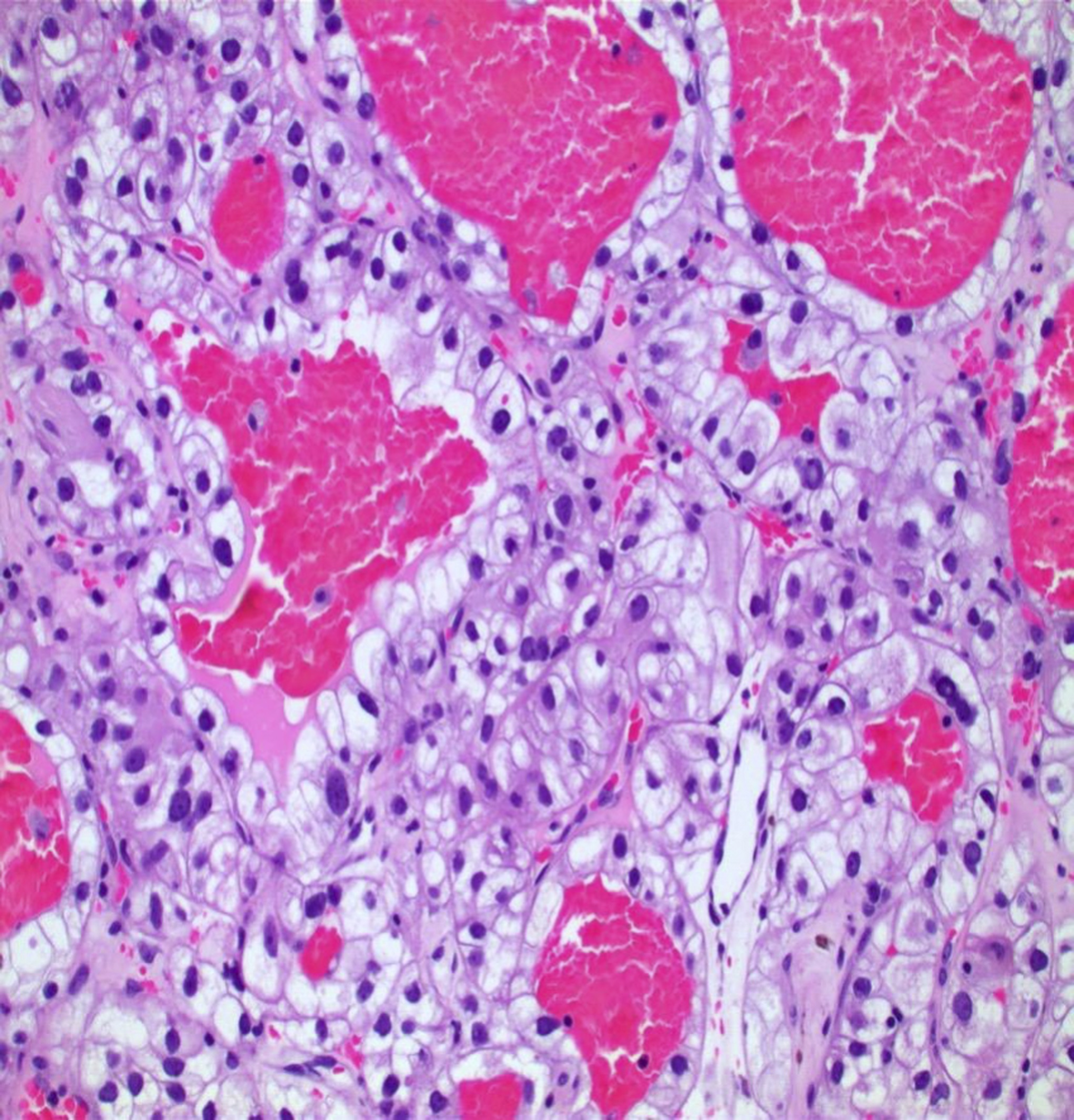
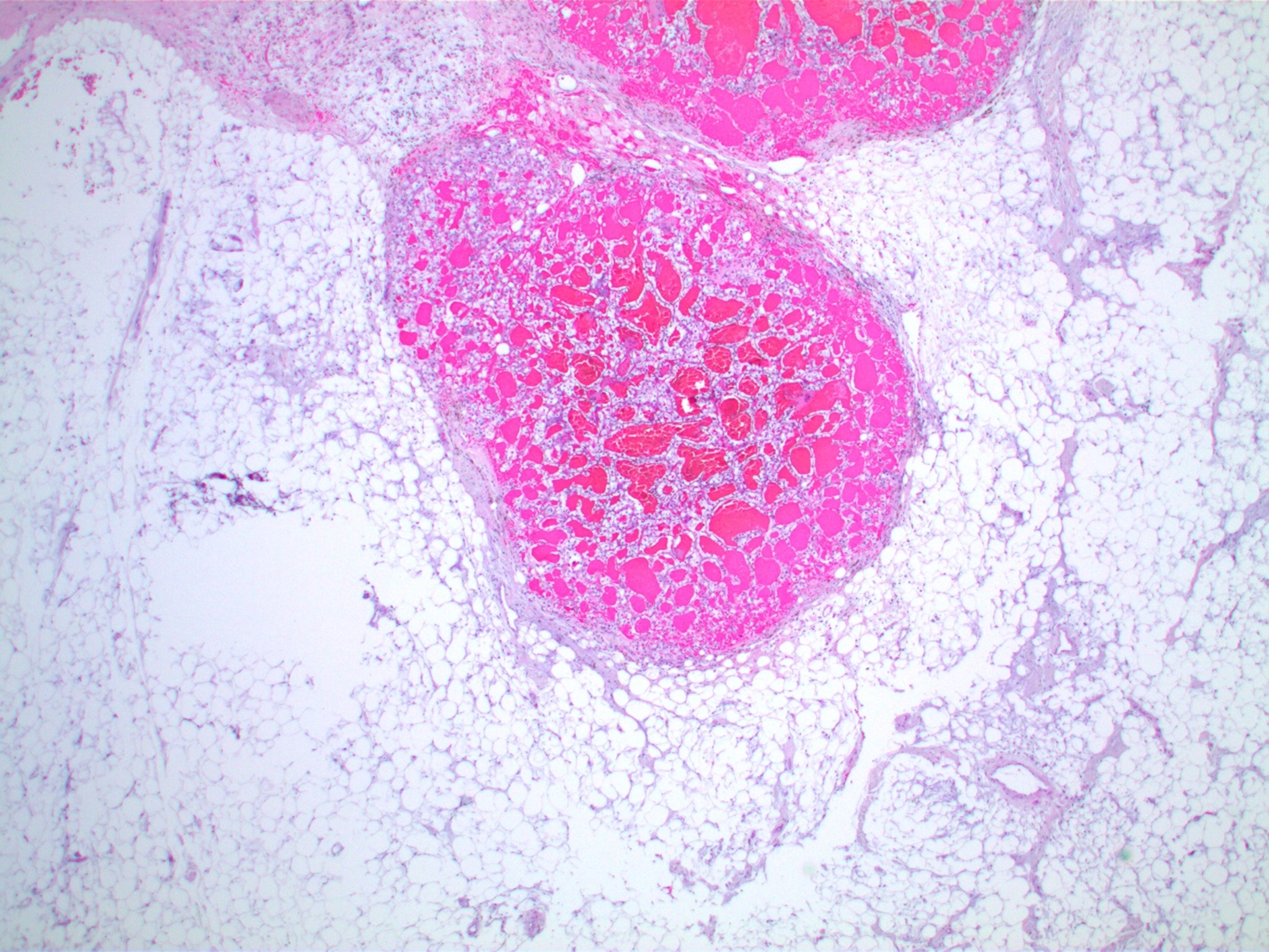
 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 2
Fig. 2 Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 3-C
Fig. 3-C Fig. 4
Fig. 4 Fig. 5-A
Fig. 5-A Fig. 5-B
Fig. 5-BA 75-year-old man with a medical history including type 2 diabetes mellitus with diabetic nephropathy, stage-1b primary renal cell carcinoma, and a left kidney transplant presented to our hospital after falling on ice. He reported antecedent right thigh pain before the fall. The physical examination was notable for diffuse swelling of the entire right lower extremity. Radiographs showed multiple lytic lesions in the distal right femoral metaphysis and a pathologic fracture of the right proximal tibial shaft (Figs. 1-A and 1-B). Before his presentation, the patient was presumed to be in remission from renal cell carcinoma by his medical oncologist, with the most recent treatment occurring 2.4 years previously.
The patient’s workup included a bone scan that showed increased radiotracer uptake in the skull, thoracic and lumbar spine, sternum, left proximal part of the humerus, left elbow, bilateral sacroiliac joints, right proximal and distal parts of the femur, and proximal part of the tibia. A computed tomographic (CT) scan of the chest, abdomen, and pelvis revealed numerous pulmonary nodules, bilateral hilar lymphadenopathy, multiple subcutaneous nodules, abdominal and pelvic ascites with associated atelectasis, and bilateral pleural and innumerable bony metastases. A magnetic resonance imaging (MRI) scan of the right thigh revealed a well-defined fat signal mass in the vastus lateralis, superolateral to the distal femoral metastases. It contained small foci of low T1 and bright T2 signal and enhancement on postcontrast sequences (Fig. 2).
Surgical repair of the patient’s pathological fractures and removal of the soft-tissue lesion were planned for the same operation, and the patient underwent open biopsy with an intraoperative frozen section of the femur, followed by fixation of the right femur and tibial pathologic fractures (Figs. 3-A, 3-B, and 3-C). However, prior to fracture fixation, the patient underwent marginal excision of the mass to ensure no cross-contamination between the femoral lesion and the soft-tissue mass (Fig. 4).
The outer surface of the fatty, soft-tissue mass was smooth, and sectioning revealed tan-yellow lobulated cut surfaces with multiple well-circumscribed hemorrhagic nodules ranging from 0.3 to 0.7 cm. The histology of the mass is shown in Figures 5-A and 5-B.
The histology of the soft-tissue mass was interpreted as a lipoma that was involved by metastatic renal cell carcinoma. The final pathology of the intraosseous bone lesion also showed metastatic renal cell carcinoma. The interval from primary cancer diagnosis to metastasis was 2.6 years. The patient was diagnosed with tumor-to-tumor metastasis (renal cell carcinoma to a benign lipoma).
All 3 pathologic specimens were morphologically identical with polygonal cells of abundant clear glycogen and lipid-rich cytoplasm arranged in cords, and a rich vascular network was notable in the renal cell carcinoma (Figs. 5-A and 5-B). Immunohistological stains of the right tibial lesion were positive for PAX8 and RCC (markers commonly found in renal cell carcinoma).
The patient received radiotherapy postoperatively for lytic lesions. Before he was lost to follow-up after 2 months, he had begun a treatment regimen of chemotherapy with his medical oncologist.
Proceed to Discussion >>Reference: Martin K, Rivera-Pintado C, Cerniglia K, Usmani K, Zhu G, Kim TWB. Tumor-to-tumor metastasis: renal cell carcinoma metastasizing to a lipoma of the thigh: a case report. JBJS Case Connect. 2022 Jun 8;12(2).e22.00049.
The 4 current inclusion and exclusion criteria for tumor-to-tumor metastasis include: (1) >1 separate and histologically distinct primary tumor must be in existence to be included; (2) the recipient tumor must be a “true” benign or malignant neoplasm to be included (a “true” neoplasm is described as disorganized and independent hyperplasia of tissues, which tend to invade and metastasize); (3) the metastatic tumor must be a “true” metastasis that is encompassed within the recipient tumor to be included (a “true” metastasis is not a result of a collision tumor or direct extension of the primary tumor); and (4) tumors metastasized to the lymphatic system where lymphoreticular malignancies such as lymphomas and leukemias already exist are excluded. In the present case, the inclusion of renal cell carcinoma metastasizing to a lipoma meets the above criteria.
Cases of tumor-to-tumor metastasis from one primary tumor to another are extremely uncommon, especially in the case of renal cell carcinoma donating the metastasis. Renal cell carcinoma most commonly receives tumor-to-tumor metastasis, reportedly occurring in up to 75% of cases described in the literature. There are several theories that may explain the high incidence of renal cell carcinoma as a recipient for tumor-to-tumor metastasis. In 1889, Paget et al. proposed a “seed and soil” theory indicating the “seed” as specific tumor cells with metastatic potential and the “soil” as any organ or tissue that provides a proper environment for the growth of tumor cells. In 1928, Ewing et al. proposed a “mechanical” theory for metastasis, in which there is consideration for the amount of tumor cells delivered to a specific target organ, and this determines the specificity of metastasis. Renal cell carcinoma itself is a highly vascular tumor that is believed to “prevascularize” the region by secreting its own tumor angiogenic factor. In addition, the kidneys receive substantial blood flow and thus embolic shed. This supports both the “seed and soil” and “mechanical” theories of metastasis.
However, it is still unknown how renal cell carcinoma may instead donate the “seeds” in a given case of tumor-to-tumor metastasis because there are very few cases in the literature. Most cases with renal cell carcinoma as a donor in tumor-to-tumor metastasis involve benign intracranial, thyroid, and pulmonary neoplasms as recipients. In a description of renal cell carcinoma that metastasized to a benign hemangioblastoma, it was suggested that because benign tumors grow slowly and are often unnoticed for long periods, they are more likely to be targeted by a more aggressive tumor in tumor-to-tumor metastasis. There is also a hypothesis that suggests that the environment of the recipient tumor may encourage tumor-to-tumor metastasis, especially in the case of a glycogen and lipid-rich environment. In this case report, renal cell carcinoma metastasized to a benign lipoma in the setting of widespread osseous metastasis, which is a phenomenon that has not been reported in the literature, to the best of our knowledge.
Lipomas are common, benign, soft-tissue tumors occurring in adults. They are typically slow-growing, with little risk of malignant transformation, and usually are managed with observation. An orthopaedic oncologist may perform a marginal excision if the mass increases in size, is cosmetically undesirable, or is symptomatic. In this patient, the lipoma was incidentally identified on an MRI scan that was acquired to evaluate for osseous metastases. At the time, the radiology report raised the suspicion that the lipoma might be targeted by metastases. The lipomatous mass was excised, and pathology revealed a lipoma involved with metastatic renal cell carcinoma. We noted that the femoral metastases, pathological fractures, and tumor-to-tumor metastasis to the lipoma were all ipsilateral, which is likely not purely coincidental, because the primary tumor was also right-sided.
This case ultimately highlights the possibility that renal cell carcinoma can be the “donor” in tumor-to-tumor metastasis, albeit a rare event.
Reference: Martin K, Rivera-Pintado C, Cerniglia K, Usmani K, Zhu G, Kim TWB. Tumor-to-tumor metastasis: renal cell carcinoma metastasizing to a lipoma of the thigh: a case report. JBJS Case Connect. 2022 Jun 8;12(2).e22.00049.
What is the diagnosis?
Clear cell sarcoma
Dedifferentiated lipoma
Tumor-to-tumor metastasis (renal cell carcinoma to a benign lipoma)
Epithelioid hemangioendothelioma
Amelanotic melanoma, probably metastatic