A Fifty-three-Year-Old Woman with Left Shoulder Pain
January 2, 2013
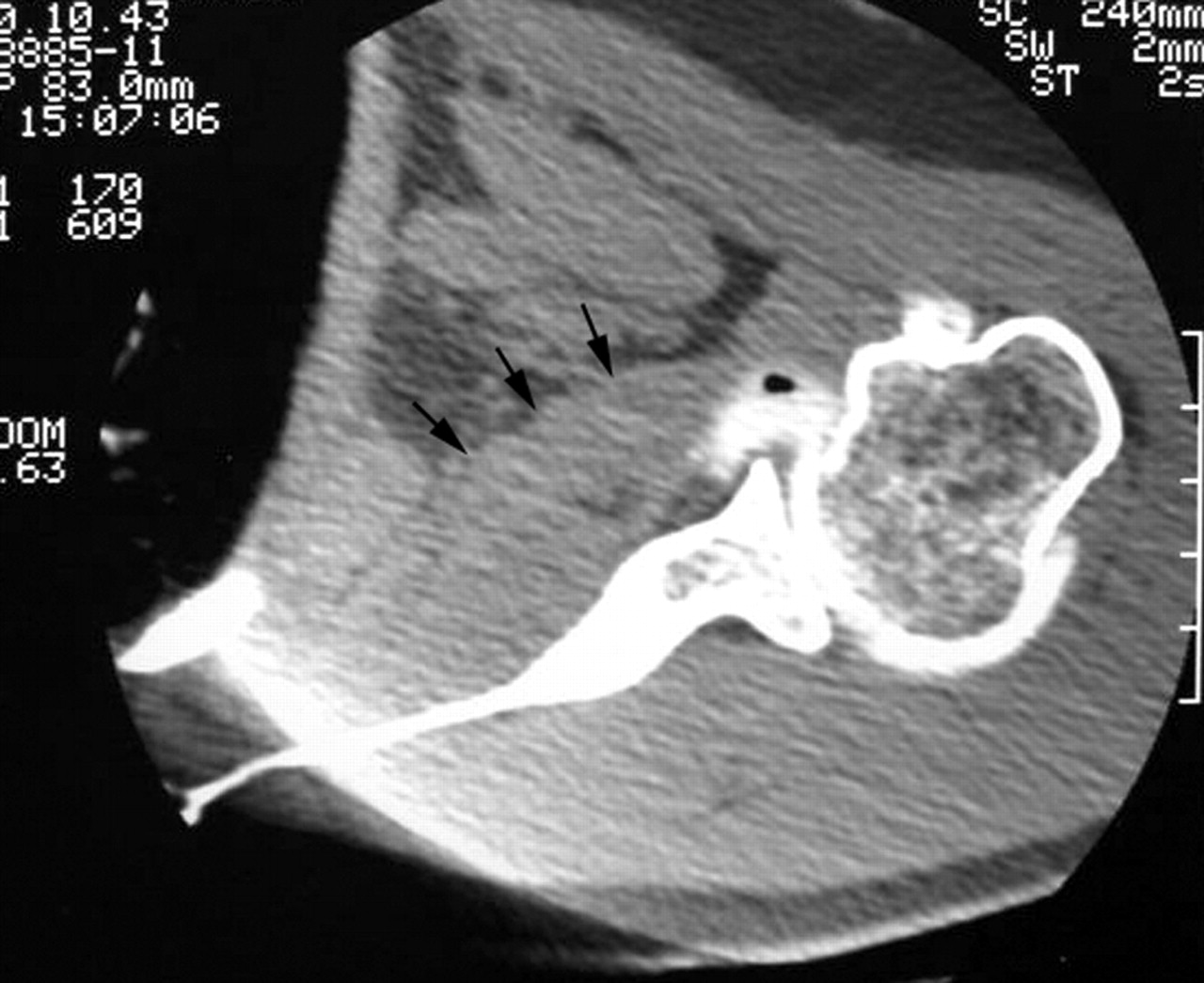

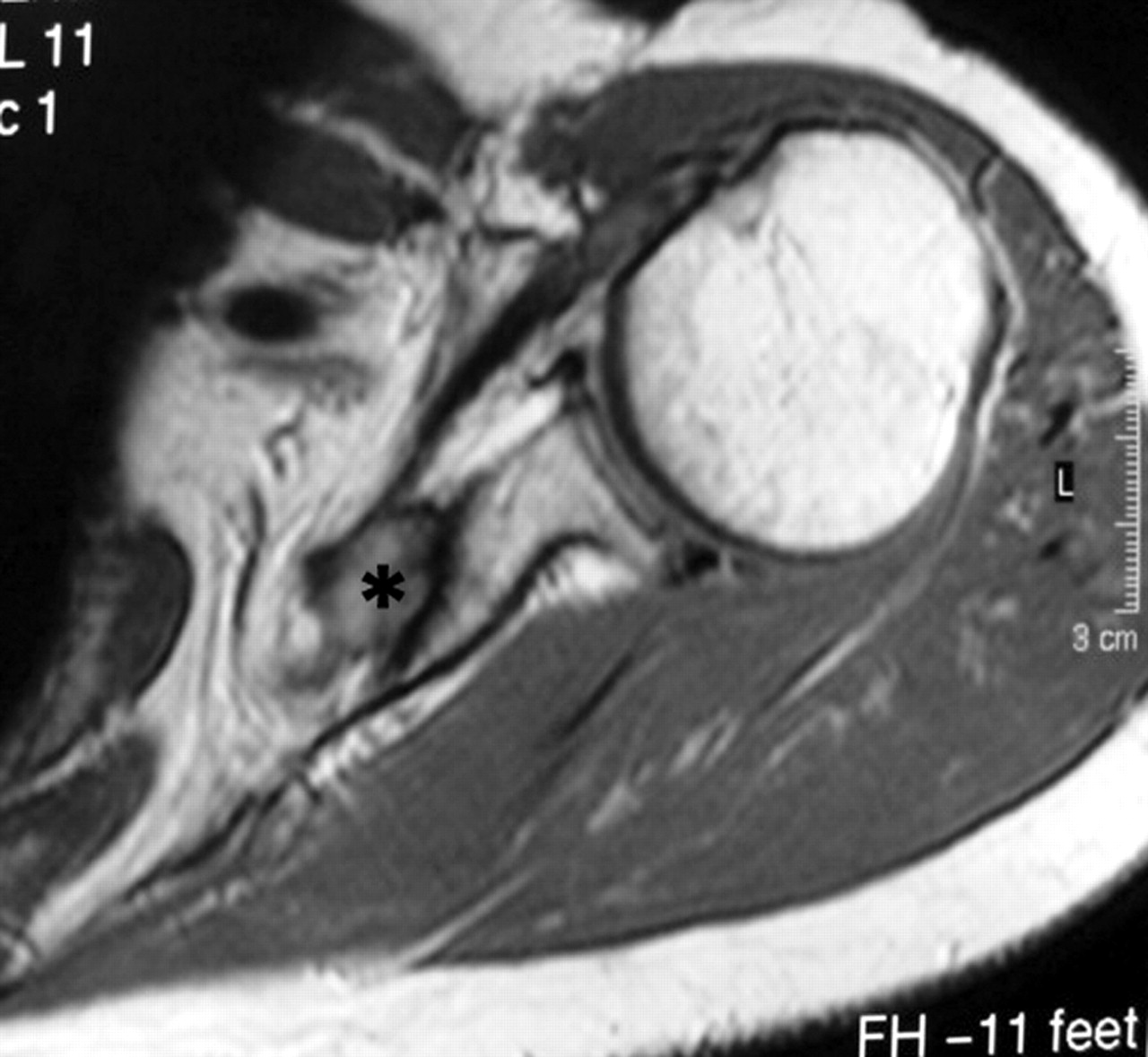
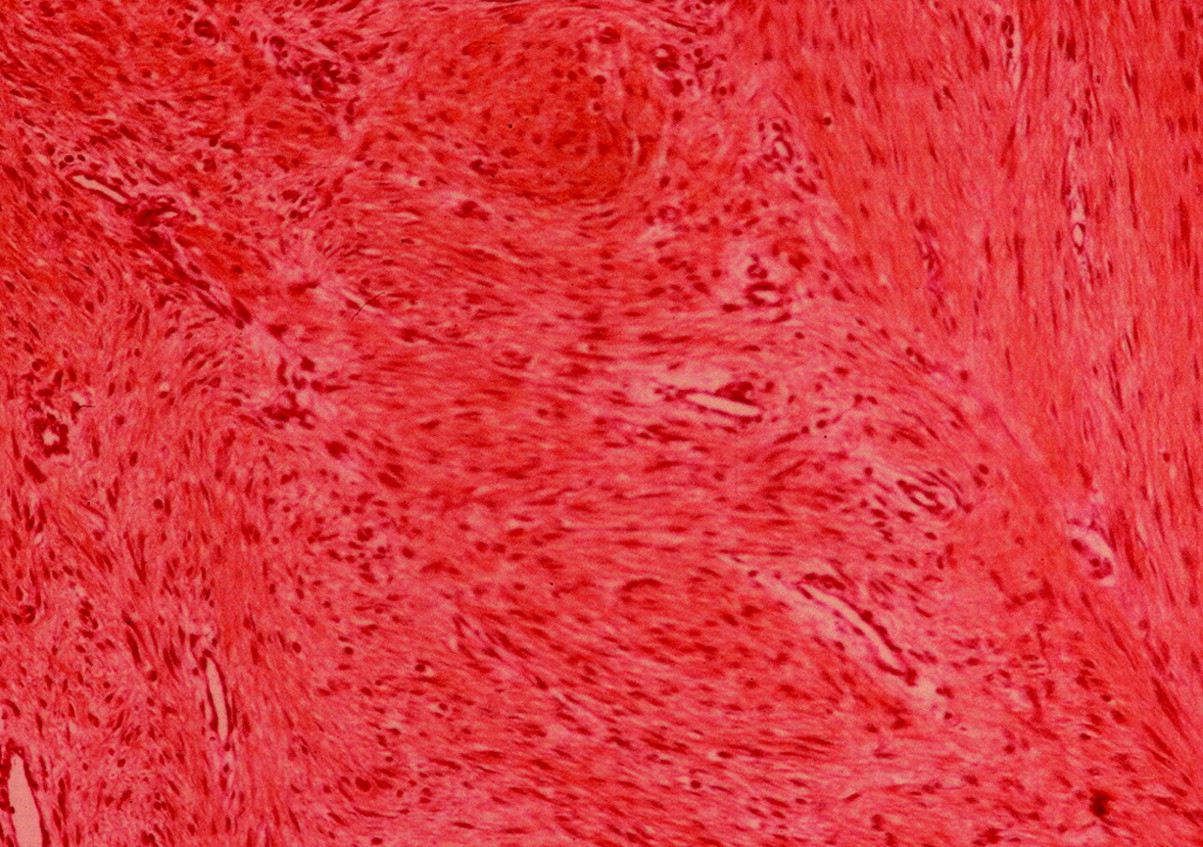
 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 1-C
Fig. 1-C Fig. 1-D
Fig. 1-D Fig. 1-E
Fig. 1-EA fifty-three-year-old woman who was right-hand dominant and worked as an administrator presented with progressive pain in the left shoulder, including mild night pain, of insidious onset occurring over a two-year period. The pain was described as a dull ache of variable intensity deep within the shoulder. She reported that she had not had any fevers or other systemic symptoms. The only prior treatment was a subacromial injection of lidocaine and corticosteroid, which had been given by her primary care physician, and it had provided no relief. Plain radiographs and a computed tomographic arthrogram that had been obtained by her primary care physician were initially interpreted as normal. The medical history and review of systems were unremarkable, she was taking no medication, and she had no history of smoking. On clinical examination, the skin had no abnormalities. No atrophy or asymmetry was noted in the upper extremities or shoulder girdles. Passive and active external rotation with the arm at the side was 10° for the left shoulder and 80° for the right shoulder. The remainder of the examination demonstrated no discrepancies between the right and left upper extremities, including anterior elevation in the plane of the scapula (170°), abduction (175°), internal rotation (seventh thoracic vertebra), and external rotation with the arm abducted to 90° (95°). The rotator cuff strength was completely intact to manual testing. The findings of the lift-off and bellypress tests and the external rotation lag sign were negative. No tenderness was noted about the shoulder, and no masses were palpable. No signs of instability or abnormality of the biceps or labrum were discovered. Although the computed tomographic arthrogram obtained by the primary care physician was initially interpreted as normal closer inspection revealed that the subscapularis appeared to be excessively thick in its anteriorposterior diameter (Fig. 1-A). Magnetic resonance imaging of the shoulder was then performed (Fig. 1-B) and demonstrated a lesion within the subscapularis musculature. At another institution, the patient underwent an incisional biopsy that revealed a soft-tissue tumor. A local resection of the tumor with lengthening and repair of the subscapularis tendon was performed. Following the tumor resection, the patient did well for approximately two years and then she began to have a progressive return of the prior symptoms over a three-month period. At that time, the findings on the clinical examination were nearly identical to those on the initial evaluation (external rotation with the arm at the side was 0°, but the findings were otherwise unremarkable). Magnetic resonance imaging showed a tumor recurrence within the subscapularis muscle in the region in which the tumor had initially occurred (Fig. 1-C). The histology slides from the initial resection were reviewed to determine the precise diagnosis prior to additional surgery. A photomicrograph of the tumor tissue is shown in Figure 1-D.
The diagnosis was a desmoid tumor. The patient then underwent a wide excision of the tumor including excision of the superior two-thirds of the subscapularis muscle and a portion of the scapular body adjacent to the tumor. A deltopectoral approach was used, and the scar from the previous skin incision was excised. The conjoined tendon was retracted medially, and a wide Homan-type retractor was placed anterior to the subscapularis muscle hinging on the medial border of the scapula. The mass within the subscapularis was palpated and excised en bloc with a cuff of normal-appearing tissue including a full-thickness resection of the portion of the scapula posterior to the tumor. All tissue margins were found to be free of reactive tissue and tumor. At the time of writing, twelve months after the most recent procedure, the patient had no signs of recurrence. On clinical examination, she had persistent weakness on internal rotation (grade 4 of 5) but otherwise had normal shoulder function. The findings of the lift-off and belly-press tests were negative, and the apprehension test, drawer test, and load and shift test demonstrated no signs of glenohumeral instability. The scapular body was partially resected during revision surgery (Fig. 1-E).
Proceed to Discussion >>Reference: Sikka RS, Vora M, Edwards TB, Szabo I, Walch G. Desmoid tumor of the subscapularis presenting as isolated loss of external rotation of the shoulder. A report of two cases. J Bone Joint Surg Am. 2004 Jan;86(1):159-64.
This case represents an uncommon presentation of tumor about the shoulder girdle. Although the patient presented with symptoms similar to those seen in association with adhesive capsulitis, i.e., pain and loss of motion, the loss of motion occurred in only one plane (external rotation with the arm at the side) in contrast to a frozen shoulder, which has loss of motion in multiple planes. Although tumors of the shoulder girdle are rare, they must be considered in the differential diagnosis when one is faced with this uncommon presentation. A desmoid tumor in the shoulder girdle typically presents as a solitary painless, deep, firm mass that ranges between 5 and 10 cm in size. Pain can be spontaneous but is usually produced with palpation or movement of the affected muscle. Other associated symptoms include numbness, hyperesthesia, and weakness. Enzinger and Shiraki reported on a series of thirty cases of desmoid tumors in the shoulder girdle. All patients reported a firm fixed mass in the shoulder region. The mass had grown in size in all patients, and half of the patients had tenderness or pain over the tumor site. Several patients had evidence of impingement upon the brachial plexus by the infiltrating tumor. Seven patients were reported to have growth manifested in the anterior or posterior walls of the axilla. These tumors infiltrated the pectoralis major or the muscles forming the posterior axillary wall, particularly the subscapularis. Impairment of motion, ranging from stiffness of the affected limb to complete paralysis, was noted in several patients. In contrast to these patients, our patient presented with no perceptible mass, which was perhaps secondary to the deep location of the tumor and the relatively early detection. Additionally, there were no positive findings during physical examination of the rotator cuff, including specific examination of the subscapularis with the lift-off and belly-press tests, suggesting that these tests are not diagnostic for tumors located within the subscapularis muscle. The only clinical finding suggestive of a tumor involving the subscapularis muscle was that of isolated loss of external rotation with the arm held at the side. This case reinforces the use of magnetic resonance imaging as the imaging modality of choice when a tumor of the shoulder girdle is suspected. Although computed tomographic arthrography is very effective in identifying rotator cuff tears, it did not distinguish between the tumor and the subscapularis muscle in this patient, which caused a delay in the diagnosis. On the basis of the demographic, clinical, and radiographic findings, the differential diagnosis includes extra-abdominal desmoid tumor, elastofibroma, and, less likely, soft-tissue sarcoma (synovial cell sarcoma, fibrosarcoma, or malignant fibrous histiocytoma). If left untreated, desmoids may become extremely large. They infiltrate adjacent muscle, extend along fascial planes, engulf blood vessels and nerves, and become attached to and erode bone. Regional and distant metastases rarely occur. Additionally, the strong likelihood of involvement of local musculature can result in loss of limb function. At the muscle border, the tumor often extends between the muscle fascicles and replaces the perimysium and epimysium before isolating and engulfing the muscle. The tumors tend to grow between and around muscle fibers and thereby isolate the fibers, which undergo atrophy as a result. Appropriate treatment should include a wide resection of normal tissue surrounding the lesion because it is not possible to assess the true proliferation of the tumor either clinically or histologically. The rate of recurrence has been reported to be as high as 77% in patients who had not had a wide resection. Our patient demonstrated the propensity of desmoid tumors of the shoulder girdle to recur and the aggressive measures that may be necessary to resect these tumors. Attempts at wide resection of tumors involving the subscapularis, particularly those extending into its inferior portion, may disrupt the anterior humeral circumflex artery in a proximal enough location to compromise the arcuate branch of the ascending portion of the anterior humeral circumflex artery as well as the collateral flow. In summary, when a patient is seen because of isolated loss of external rotation of the shoulder, a tumor involving the subscapularis, although rare, must be suspected. A high index of suspicion that is based on clinical examination combined with early magnetic resonance imaging may lead to earlier detection of these tumors, resulting in a technically easier resection and reconstruction.
Reference: Sikka RS, Vora M, Edwards TB, Szabo I, Walch G. Desmoid tumor of the subscapularis presenting as isolated loss of external rotation of the shoulder. A report of two cases. J Bone Joint Surg Am. 2004 Jan;86(1):159-64.

Desmoid tumor
Elastofibroma
Synovial cell sarcoma
Fibrosarcoma
Malignant fibrous histiocytoma