A Forty-two-Year-Old Woman with Left-Sided Thigh Pain
August 6, 2014

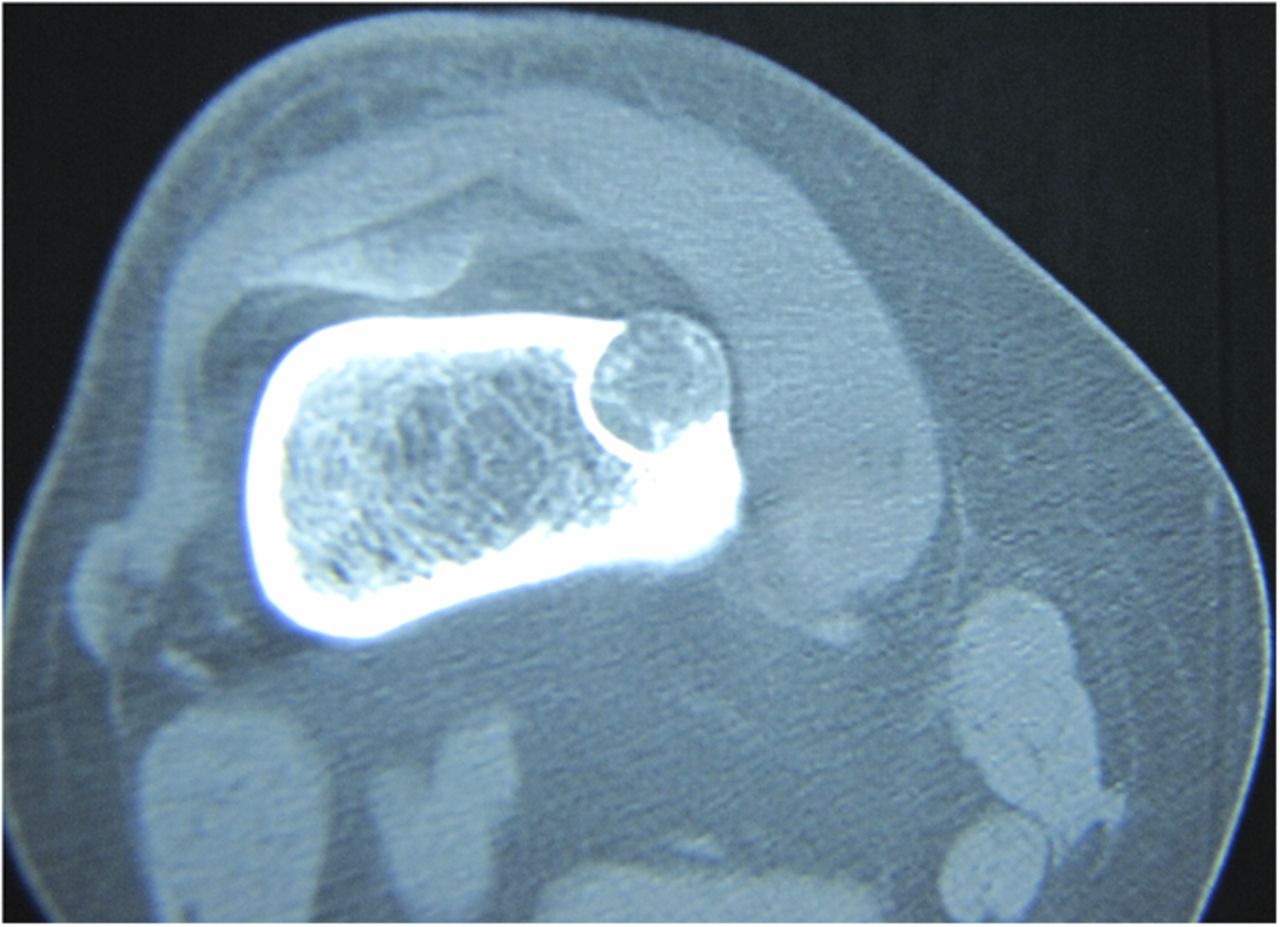

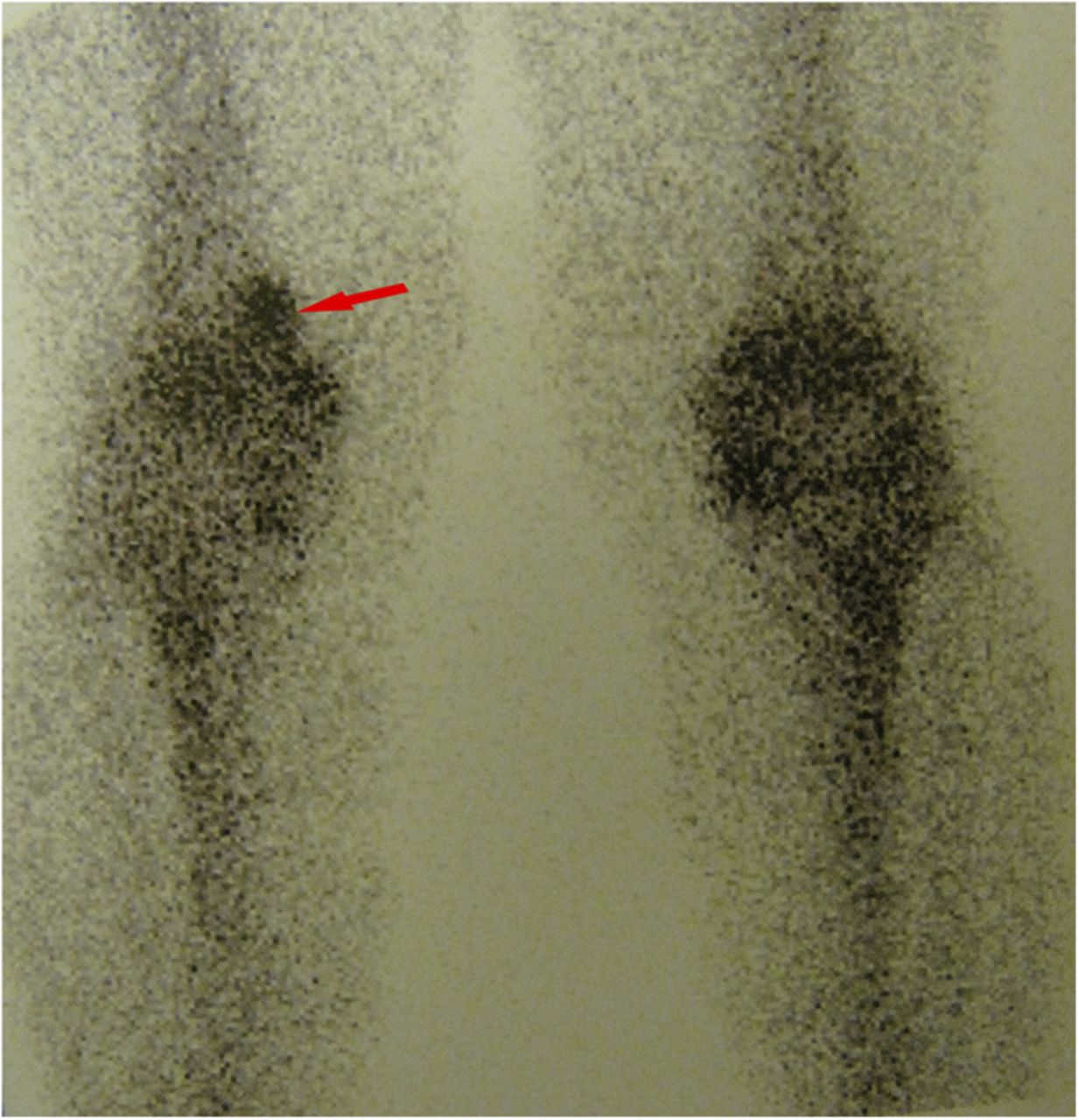
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4An otherwise healthy forty-two-year-old woman presented with a ten-month history of left-sided pain in the distal aspect of the thigh. The pain was mild, localized, and nonradiating, and did not contribute to any substantial sleep disruption. Treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) had a partial response. Physical examination showed local tenderness upon palpation. There were no other signs of swelling or edema at the site of the lesion. In addition, the patient had full active range of motion of the adjacent joints, which was not associated with pain. Radiographs showed a round lytic lesion in the anteromedial cortex of the left distal femoral metaphysis that was about 1 cm in diameter (Fig. 1). Computed tomography (CT) revealed that the lesion had arisen from within the anteromedial cortex and was surrounded by a rim of sclerosis in the medulla, with stippled calcification of the matrix (Fig. 2). Moreover, T2-weighted magnetic resonance imaging (MRI) sequences showed high signal intensity, with slight extension into the subperiosteum (Fig. 3). The technetium-99m (Tc-99m) bone scan also showed a slightly increased uptake (Fig. 4). Intralesional curettage was performed. Histopathologic sections revealed hyaline cartilage of low cellularity; there were no atypical features and the tumor was not surrounded by lamellar bone. The symptoms resolved after surgery. Three years later, the patient was pain-free and had good range of motion; there had been no local recurrence of the lesion.
Reference: Jamshidi K, Bagherifard A, Ghafarri B. Intracortical or transcortical chondroma: a report of two cases. JBJS Case Connect, 2014 Apr 23;4(2):e33.
In 1990, Abdelwahab et al. first introduced the term “intracortical chondroma,” a lesion that radiologically split the cortex and outer layer of the cortex over the lesion, which was ballooned but intact. Because histology demonstrated that the lesion was not fully covered by the cortex in their patient, they believed it was a periosteal chondroma with atypical appearance. Intracortical chondroma (IC) is a round or oval benign cartilaginous tumor that arises from the cortex, and cortical bone surrounds the entire lesion. In 2006, Jones et al. reported two cases of IC that were surrounded completely by cortical bone. They discussed the first two cases that had been presented in the literature, which they believed were not truly intracortical because the cortex overlying the lesions was protuberant. They assumed that the tumors arose from the periosteum and that over the years, periosteal bone had matured to produce neocortex over the tumors; therefore, they believed them to be periosteal chondromas. In 1952, Lichtenstein and Hall first introduced the entity of periosteal chondroma. They described this benign cartilaginous tumor as originating from or beneath the periosteum, which then causes erosion and sclerosing of the underlying cortex. DeSantos and Spjut analyzed the radiographic features of twenty-two cases of periosteal chondroma. They described all of the cases as arising in the cortex or periosteum without evidence of medullary cavity involvement. Boriani et al. reported twenty cases of periosteal chondroma and stated that this tumor arises from under the periosteum. Radiologically, the tumor has cortical erosion and sclerosing of the underlying cortex as well as elevated edges that form a craterlike excavation that is accompanied by the existence of a soft-tissue mass. Occasionally, a delicate shell of periosteal new bone surrounds the soft-tissue mass. We report a case of chondroma arising from within the cortex. Interestingly, the tumor extended beyond the cortex into the subperiosteum with no bone over it. The radiographic appearance was unusual and did not match the typical descriptions of periosteal chondroma. We propose that the tumor was a transcortical tumor because it arose from within the cortex. Perhaps it was able to split the cortex and continue to grow because of its location in the metaphysis, which had a thinner cortex compared with the diaphysis. While other benign intracortical lesions, excluding osteoid osteoma, do not produce pain, the mechanism of pain in ICs has not been identified. Hypothetically, it could be associated with the stretching of the periosteum, which contains pain receptors. Our case presented with regional pain. The differential diagnosis of ICs includes benign lesions such as osteoid osteomas, fibrous cortical defects, intracortical hemangiomas, intracortical chondromyxoid fibromas, intracortical fibrous dysplasia, intracortical chondroblastomas, and osteomyelitis, as well as malignant conditions such as intracortical chondrosarcoma and intracortical osteosarcoma. Babinet et al. described an intracortical chondrosarcoma that was located in the proximal femoral diaphysis and was radiologically similar to our case. Histopathology of our case showed hyaline cartilage of low cellularity without atypia, which differentiated the tumor from intracortical chondrosarcoma. Therefore, we diagnosed this patient with intracortical chondroma. The proper standard of care for ICs has yet to be identified, but simple intralesional excision of these tumors with curettage may be an acceptable treatment; our patient responded well to this approach. It is important to differentiate the malignant masses from IC because intralesional curettage will not suffice with malignant lesions. In conclusion, IC is a well-defined, painful, small, round or oval lesion with primary intracortical involvement. Tc-99m bone scans demonstrate mildly increased uptake. Sometimes, there is intralesional stippled calcification.
Reference: Jamshidi K, Bagherifard A, Ghafarri B. Intracortical or transcortical chondroma: a report of two cases. JBJS Case Connect, 2014 Apr 23;4(2):e33.
Periosteal osteoblastoma
Stress fracture
Intracortical chondroma
Brodie abscess
Chondroblastoma