A Sixty-two-Year-Old Woman with Painful Triggering at the Metacarpophalangeal Joint of the Right Hand
October 1, 2014
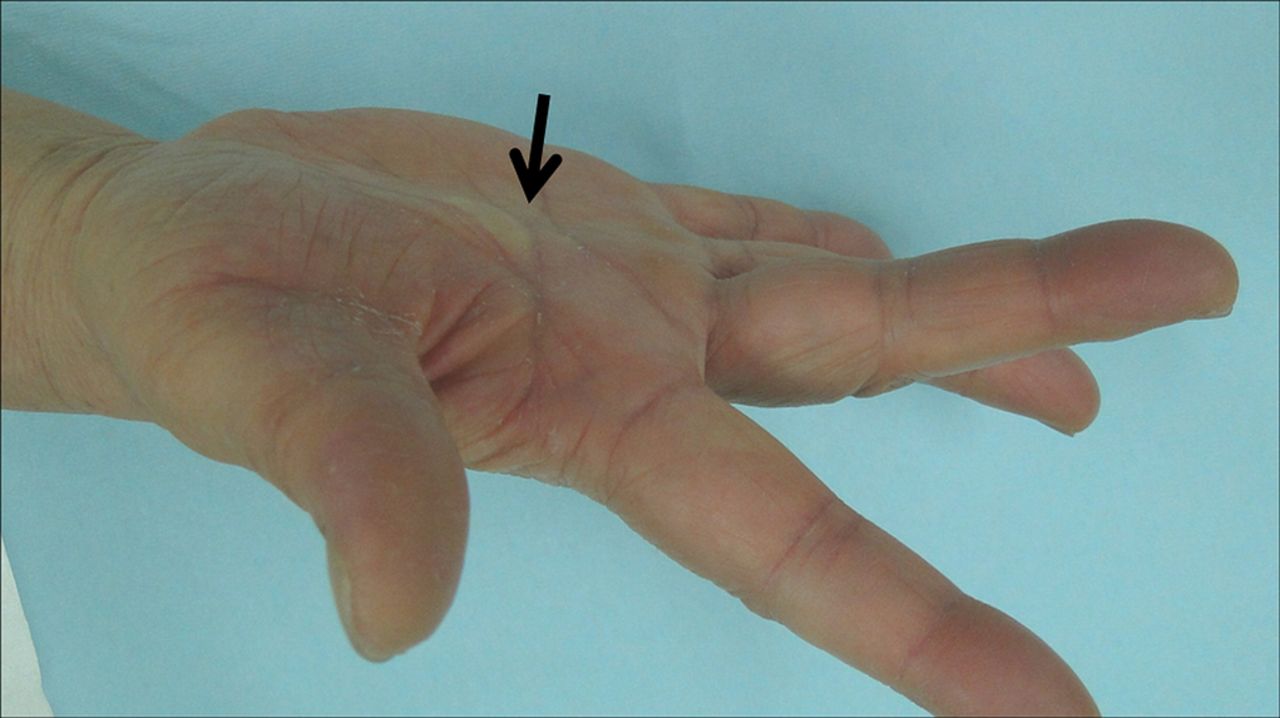
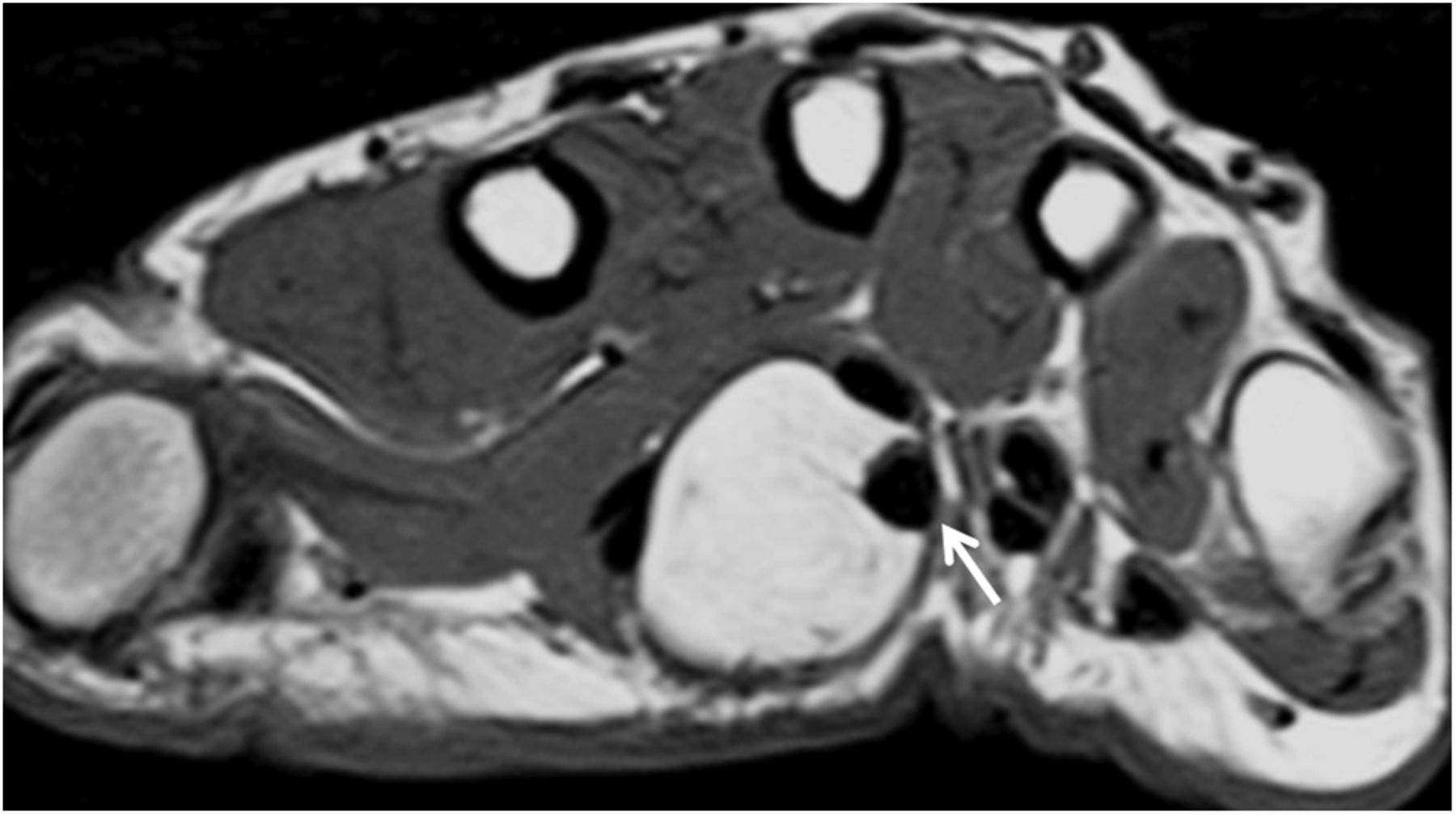
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5Over a two-year period, a sixty-two-year-old woman had experienced an extension lag at the metacarpophalangeal (MCP) joint of the right middle finger without evidence of a particular cause. She denied any prior experiences of the snapping phenomenon in the involved digit. Although passive extension initially had been possible, the patient had developed painful triggering at the MCP joint and eventually had difficulty with writing and keyboard use. Subsequently, she had noticed a soft and painless tumor on the right palm. Upon initial presentation to our institution, there had been no change in the size of the tumor, but there was numbness in the ulnar aspect of the right index finger. On physical examination, palpation revealed a 2 × 1-cm tumor in the center of the right distal transverse palmar crease. The tumor was soft and nontender. However, there was a positive Tinel sign that radiated to the ulnar aspect of the right index finger. The active range of motion for the right middle finger included flexion of 90° and extension of −15° for the MCP joint, flexion of 90° and extension of 0° for the PIP joint, and flexion of 80° and extension of 0° for the distal interphalangeal (DIP) joint (Fig. 1). Although the passive range of motion improved to 0° for the MCP joint, triggering and pain arose upon release, snapping back to flexion. There was no substantial difference in the crosswise direction on the standard flexor digitorum superficialis (FDS) test. Slight paresthesia was present in the ulnar aspect of the index finger pulp. The Disabilities of the Arm, Shoulder and Hand (DASH) score was 20 points. Both posteroanterior and lateral radiographs of the hand showed no obvious abnormalities. Magnetic resonance imaging (MRI) confirmed the presence of a tumor in the radial aspect of the FDS and flexor digitorum profundus (FDP) tendons, and its margins were clearly demarcated by a capsule (Fig. 2).
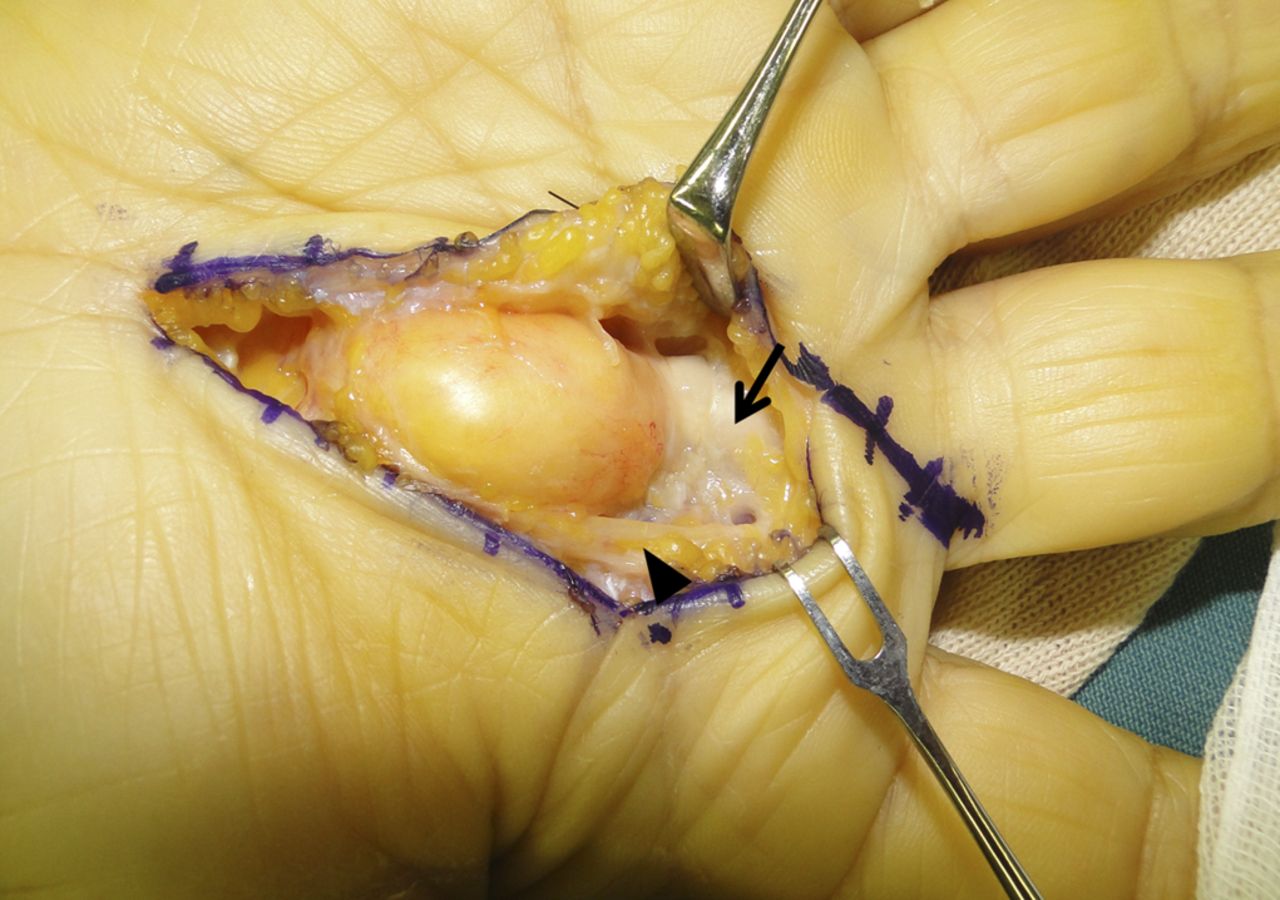
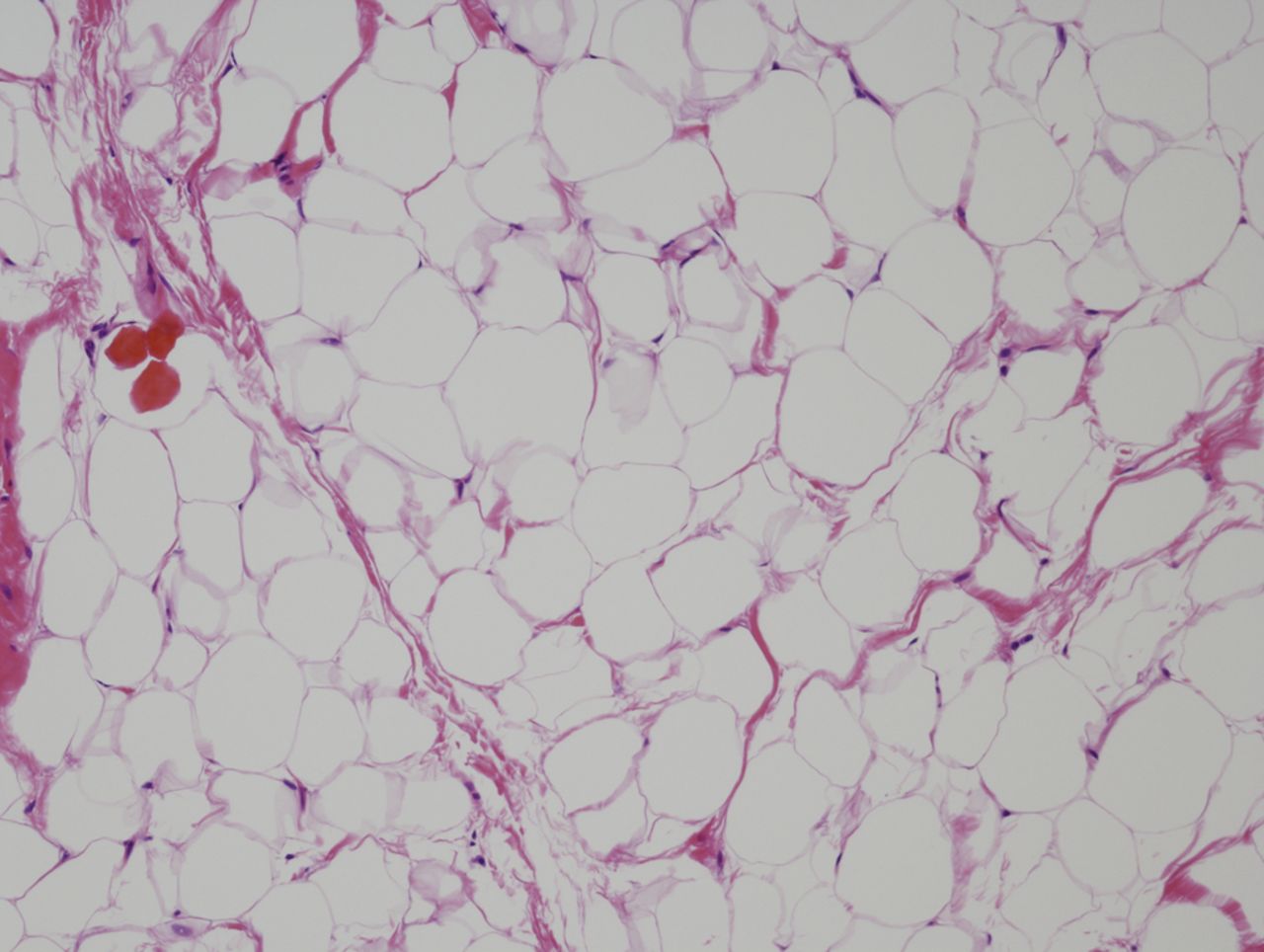
The patient was diagnosed with a locked MCP joint that resulted from a benign tumor in the flexor tenosynovium of the middle finger, and she was scheduled for surgery one month after the first medical examination. The surgical approach confirmed that the common palmar digital nerve was running on the surface of the tumor and compressing its radial aspect. The tumor was easily mobilized from the digital nerve. Because the tumor moved in conjunction with the FDS tendon and the A1 pulley was located on its distal region, the tumor compromised the full extension of the MCP joint of the middle finger by catching on the A1 pulley (Fig. 3). The A1 pulley was partially incised in order to remove the tumor. The tumor (2 × 2 × 1 cm) had a smooth yellow surface, and it was contiguous to the synovial tissue of the FDS tendon. After excision of the tumor, full range of motion was confirmed by passive extension. Histological examination revealed a mature lipoma with no atypical or necrotic tissue; the tumor was diagnosed as a benign lipoma (Fig. 4). The postoperative course was uneventful. Twelve months postoperatively, the patient had recovered full active motion, with no signs of the locked MCP joint (Fig. 5). There was no numbness at the ulnar aspect of the index finger. The DASH score had improved to 1.7. No recurrence was observed with imaging.
Proceed to Discussion >>Reference: Kito M, Yoshimura Y, Aoki K, Uchiyama S, Uehara T, Kato H. Locked metacarpophalangeal joint of the middle finger caused by a lipoma in the flexor tenosynovium. A case report. JBJS Case Connect. 2014 Aug 13;4(3):e64.
The space-occupying lesions that occur in the surrounding tissues of the digital flexor tendon include giant cell tumors or fibromas of the tendon sheath and tenosynovial lipomas; these lesions also occur with synovitis. Symptoms of these space-occupying lesions depend on their location and size. Lesions occurring within the tendon sheath of the finger result in trigger finger, while lesions occurring within the carpal tunnel result in carpal tunnel syndrome or a flexor tendon entrapment at the transverse carpal ligament. To the best of our knowledge, there have been no previous reports of locking of the MCP joint caused by a tumor occurring in the tissues surrounding the tendon. In our patient, a lipoma that was believed to have originated from the FDS tenosynovium of the middle finger had impinged on the A1 pulley while extending the MCP joint, resulting in the locked MCP joint. Full extension was made possible by excising the tumor and incising the A1 pulley. Locking of the MCP joint is often difficult to differentiate from a locked trigger finger; however, unlike triggering, a locked MCP joint does not restrict flexion and extension of the proximal interphalangeal (PIP) and DIP joints. In our patient, snapping would have occurred if the lipoma had been small enough to pass through the A1 pulley and had allowed extension of the MCP joint. However, there were no such symptoms prior to the first visit to the hospital. Therefore, the lipoma most likely occurred proximally, and the symptoms of the locked MCP joint appeared as the tumor gradually expanded distally. A locked MCP joint caused by a tumor occurring in the flexor tenosynovium rather than by a lesion within the joint is rare. When evaluating a patient with a locked MCP joint of the finger, surgeons should pay close attention not only to the presence of conventional abnormalities of the metacarpal head demonstrated by radiographs or computed tomography, but also to any tumorous lesions over the flexor tendon that are revealed with meticulous palpation, ultrasound, or MRI.
Reference: Kito M, Yoshimura Y, Aoki K, Uchiyama S, Uehara T, Kato H. Locked metacarpophalangeal joint of the middle finger caused by a lipoma in the flexor tenosynovium. A case report. JBJS Case Connect. 2014 Aug 13;4(3):e64.

Giant cell tumor of tendon sheath
Lipoma of the flexor tenosynovium
Schwannoma involving common digital nerve
Ruptured lumbrical insertion
Synovial cell sarcoma of tendon sheath