

 Fig. 1
Fig. 1 Fig. 2-A
Fig. 2-A Fig. 2-B
Fig. 2-B Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 4-A
Fig. 4-A Fig. 4-B
Fig. 4-B Fig. 5-A
Fig. 5-A Fig. 5-B
Fig. 5-B Fig. 5-C
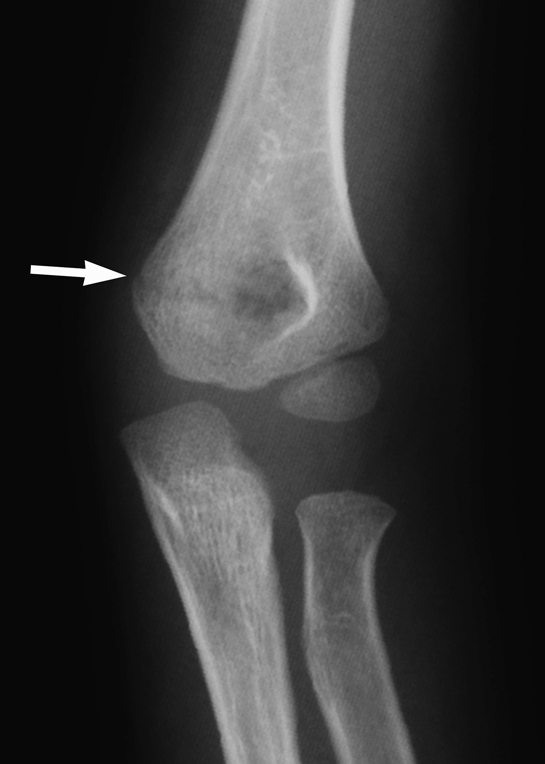
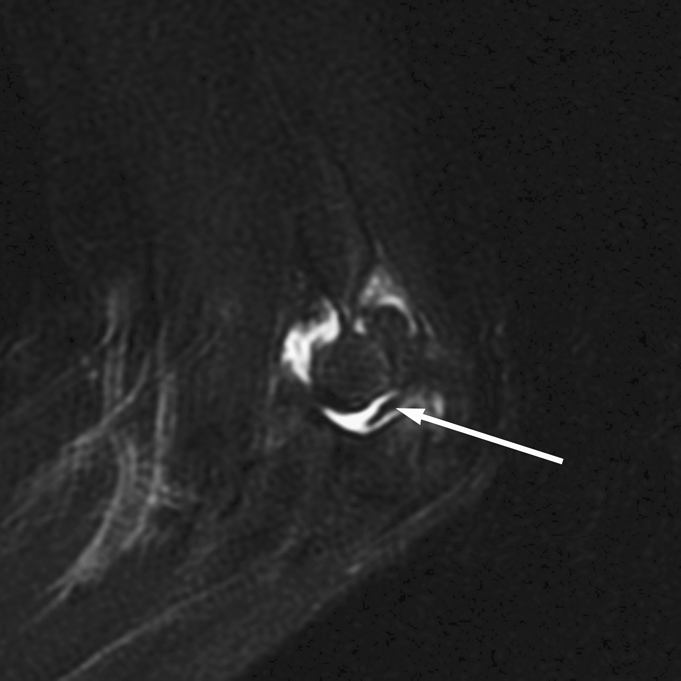
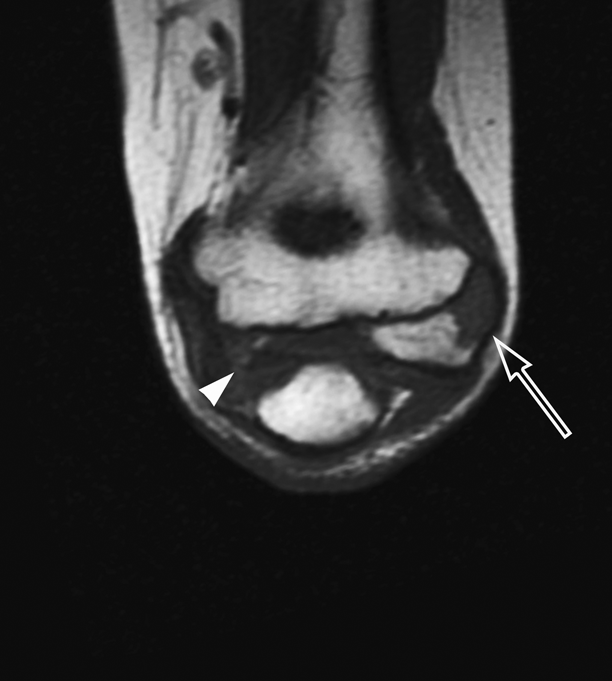
Fig. 5-CA ten-year-old boy was referred to our hospital with the symptom of locking during left elbow extension, which was accompanied with pain. The locking occurred suddenly when he turned a doorknob with the left hand. The medical history included a left supracondylar humeral fracture when he was five years old, which was treated conservatively by a local physician (Fig. 1). On the initial examination, no swelling or tenderness was observed in the left elbow. Although the active elbow flexion range was up to 137°, the active and passive extension loss was 75°, with painful locking. Passive extension induced pain on the posterolateral side of the lateral humeral condyle. The range of forearm motion was 90° for pronation and 80° for supination without limitation. Radiographs revealed an irregularly contoured ossification of the epiphysis in the lateral humeral condyle (Fig. 2-A), and computed tomography (CT) revealed irregular ossification of the medial trochlea (Fig. 2-B). Magnetic resonance imaging (MRI) revealed an abnormal low-intensity shadow on the T2-weighted sagittal imaging of the ulnohumeral joint; there was ossification of the medial trochlea and the capitellum on the T1-weighted coronal imaging (Figs. 3-A and 3-B).
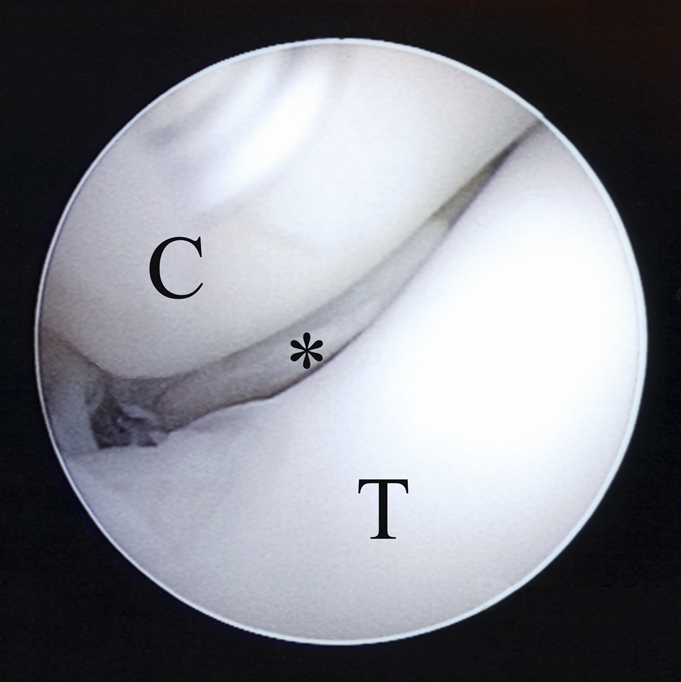
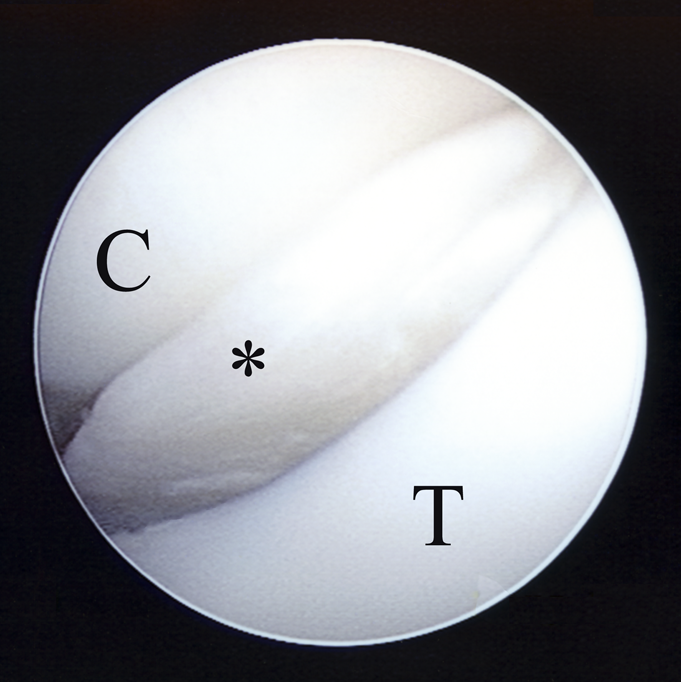
On the basis of these findings, we believed that the locked elbow joint was caused by a collateral ligament or synovial fold that was trapped in the lateral side or by intercalated loose bodies in the ulnohumeral joint. Subsequently, arthroscopic surgery was performed. During arthroscopy with an anteromedial portal, an intercalated cartilage fragment was identified between the coronoid process and the humeral trochlea. The fragment unified smoothly with the trochlear joint surface and extended inferiorly into the ulnohumeral joint on elbow flexion. It extended to and interposed within the joint on extension since it was attached to the posteromedial side of the lateral condyle as a cartilage flap. We believe that these findings explained the locking mechanism (Figs. 4-A and 4-B). The cartilage flap was resected through an open lateral approach because it was difficult to resect with use of arthroscopic equipment. Subsequently, the locking symptom disappeared. Follow-up continued until closure of the epiphyseal line occurred, and sequential follow-up radiographs revealed a fishtail deformity with a reverse-V-shaped humeral trochlea (Figs. 5-A, 5-B, and 5-C). At the final follow-up four years after the operation when the patient was fourteen years old, the range of elbow motion was 6° of hyperextension and 147° of flexion; there was no functional disability during daily and sports activities. The carrying angle was 16° on the affected elbow and 19° on the unaffected side.
Proceed to Discussion >>Reference: Ishii T, Ikeda M, Kobayashi Y, Shimizu A, Saito I, Mochida J. Locked elbow joint due to a cartilage flap caused by osteonecrosis of the humeral trochlea: a case report. JBJS Case Connector, 2013 May 22;3(2):e52.
We concluded that the patient had locking of the elbow joint because of a trochlear cartilage flap that was a result of trochlear osteonecrosis following the supracondylar humeral fracture at the patient age of five years. Several etiologies have been reported for locked elbow joints, which include loose bodies derived from osteoarthritis, osteochondritis dissecans, and synovial osteochondromatosis of the elbow joint, as well as the presence of a synovial fold, a meniscus-like tissue, and an anular ligament interposed within the radiohumeral joint. However, the clinical presentation of a locked elbow joint is rare. Our patient had an uncommon locking mechanism caused by a trochlear cartilage fragment instead of loose bodies, a collateral ligament, or a synovial fold being trapped within the joint. The mechanism was observed during arthroscopy. The cartilage fragment originated from the lateral trochlea, the end of which was attached to the posterior trochlea like a flap. The cartilage flap smoothly unified with the trochlear joint surface on elbow flexion, whereas on extension, it protruded anteriorly, becoming interposed within the ulnotrochlear joint; this caused the locking at a 75° angle of flexion. Serial chronological radiographs of the elbow in the present case revealed that the sparse ossification of the medial trochlea was oblique and irregular, which also was observed on the preoperative coronal CT. As growth continued, the oblique medial trochlear ossification center continued to form the triangular-shaped medial trochlea, with growth of the capitellar ossification center in the lateral condyle. Subsequently, the characteristic fishtail deformity of the distal part of the humerus had progressed with the nondeveloping lateral trochlea. Although trochlear osteonecrosis after distal humeral fractures in children has been reported, the exact incidence is unknown. According to previous reports, osteonecrosis could occur irrespective of the degree of the initial fracture displacement or its management. This fishtail deformity of osteonecrosis has been categorized as type A according to the Rockwood classification of trochlear osteonecrosis; it usually occurs in very distal humeral fractures or those involving the lateral condylar physis. Because there was no additional history of elbow trauma since the initial fracture in our patient, this case was considered to have a very distal humeral fracture without displacement. We believe that osteonecrosis of the lateral trochlea could not have been detected with use of preoperative MRI because the fishtail deformity itself did not represent necrotic collapse but resulted from epiphyseal growth disturbance. Thus, we believe that osteonecrosis was present before the surgical intervention. Marshall et al. reported a symptomatic type-A trochlear osteonecrosis with delamination cartilaginous injury involving the capitellum and lateral trochlea in a thirteen-year-old gymnast. In our patient, we think that a similar delamination of the trochlear cartilage related to trochlear osteonecrosis was present, and that a particular action, such as turning a doorknob, produced partial detachment of the disturbed cartilage, which then began to move into the ulnohumeral joint and eventually interrupt the joint motion, causing the locking phenomenon.
Reference: Ishii T, Ikeda M, Kobayashi Y, Shimizu A, Saito I, Mochida J. Locked elbow joint due to a cartilage flap caused by osteonecrosis of the humeral trochlea: a case report. JBJS Case Connector, 2013 May 22;3(2):e52.



Osteochondritis dissecans
Distal humeral malunion
Lateral condyle articular cartilage flap
Lateral collateral synovial fold
Intra-articular osteocartilaginous loose body