A Thirteen-Year-Old Boy with Bilateral Knee Pain and Swelling
November 2, 2011
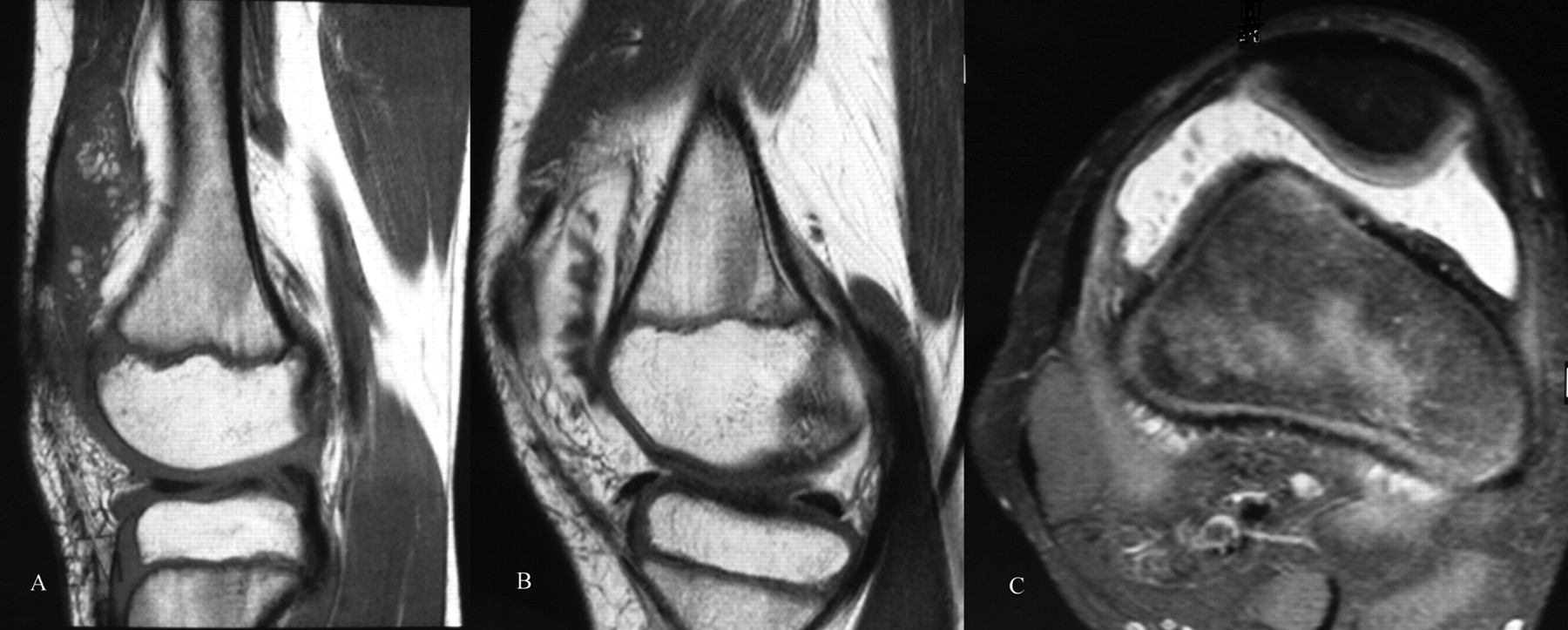
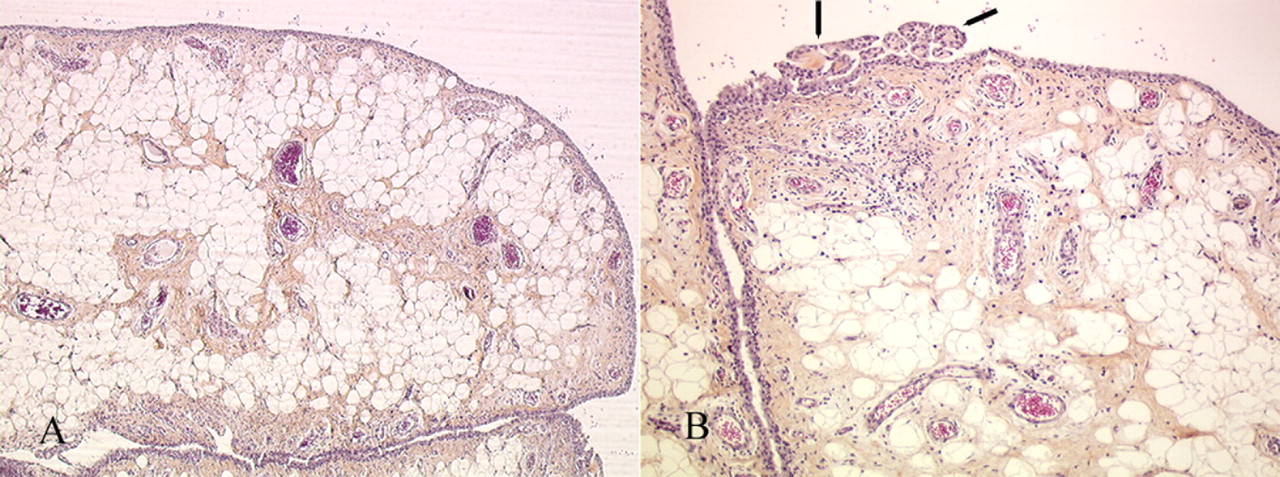
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 2
Fig. 2 Fig. 3
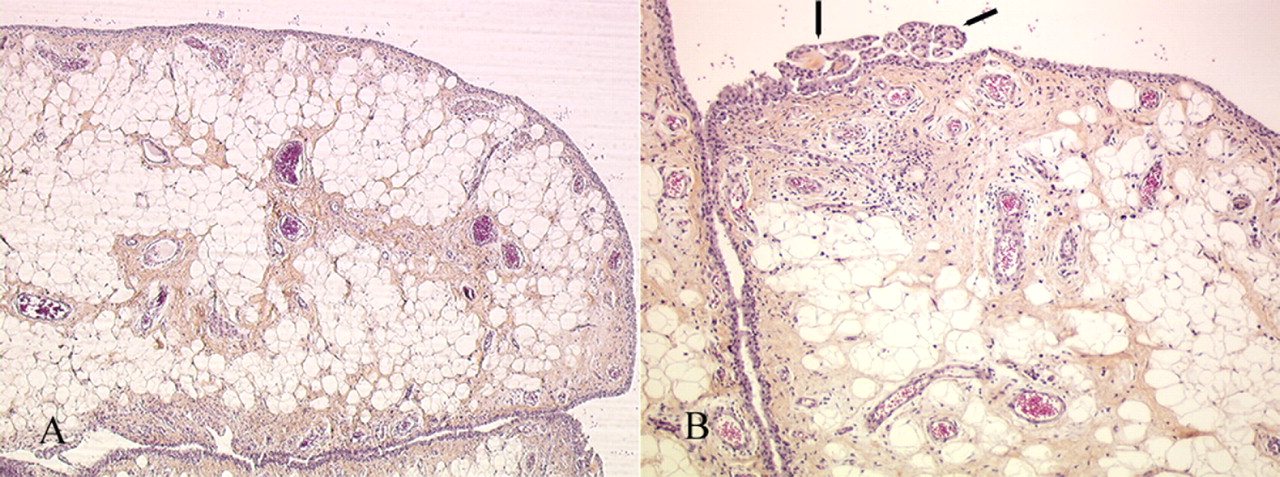
Fig. 3A thirteen-year-old boy was admitted to our hospital because of chronic pain in the left knee. He had no history of trauma or infection. The left knee had been painful for four weeks during walking and running, thus limiting his daily activities. There were no locking symptoms. The patient’s medical history and the family history were unremarkable. The boy was healthy and had a body mass index of 21 kg/m2. Physical examination revealed bilateral swelling of the knee joints. Both knees had a normal local temperature and normal skin coloration and were not tender to palpation. Both joints were more voluminous than expected, and a mild joint effusion was present bilaterally. Full extension and 140° of flexion were possible in both knees, and knee motion did not elicit pain. There was no tissue mass around the knees, and no laxity could be detected. The results of blood tests, including measurements of the erythrocyte sedimentation rate, rheumatoid factor, C-reactive protein level, histocompatibility antigen B27 (HLA-B27), and antinuclear immunoglobulin, were normal. Arthrocentesis revealed aseptic fluid, and testing of this fluid revealed a leukocyte count of 5500/mm3. Radiographs of both knee joints were normal. Magnetic resonance imaging showed a similar pattern for both knees. T1-weighted and T2-weighted axial and sagittal images showed a high-signal-intensity lesion consisting of lobulated material projecting into the suprapatellar pouch and intercondylar notch. On sagittal sections, the lesion was visualized as a frondlike or villous synovial proliferation. The proliferative tissue was limited to the anterior compartment of both knees and appeared with a high signal intensity on T1-weighted scans. After gadolinium injection, the synovium signal was enhanced on the T1-weighted images but there was no enhancement of the villous projections (Fig. 1). The condition of the joint was otherwise unremarkable except for a small effusion. Arthroscopy of the left knee was performed. The lesion appeared as multiple lobulated proliferations appended to the synovium of the suprapatellar pouch and the medial and lateral gutters. The femoral, patellar, and tibial articular surfaces had a normal appearance. In the femoral intercondylar notch, diffuse synovitis was observed surrounding the anterior and posterior cruciate ligaments. Histology of a biopsy specimen is shown in Figs. 2-A and 2-B.
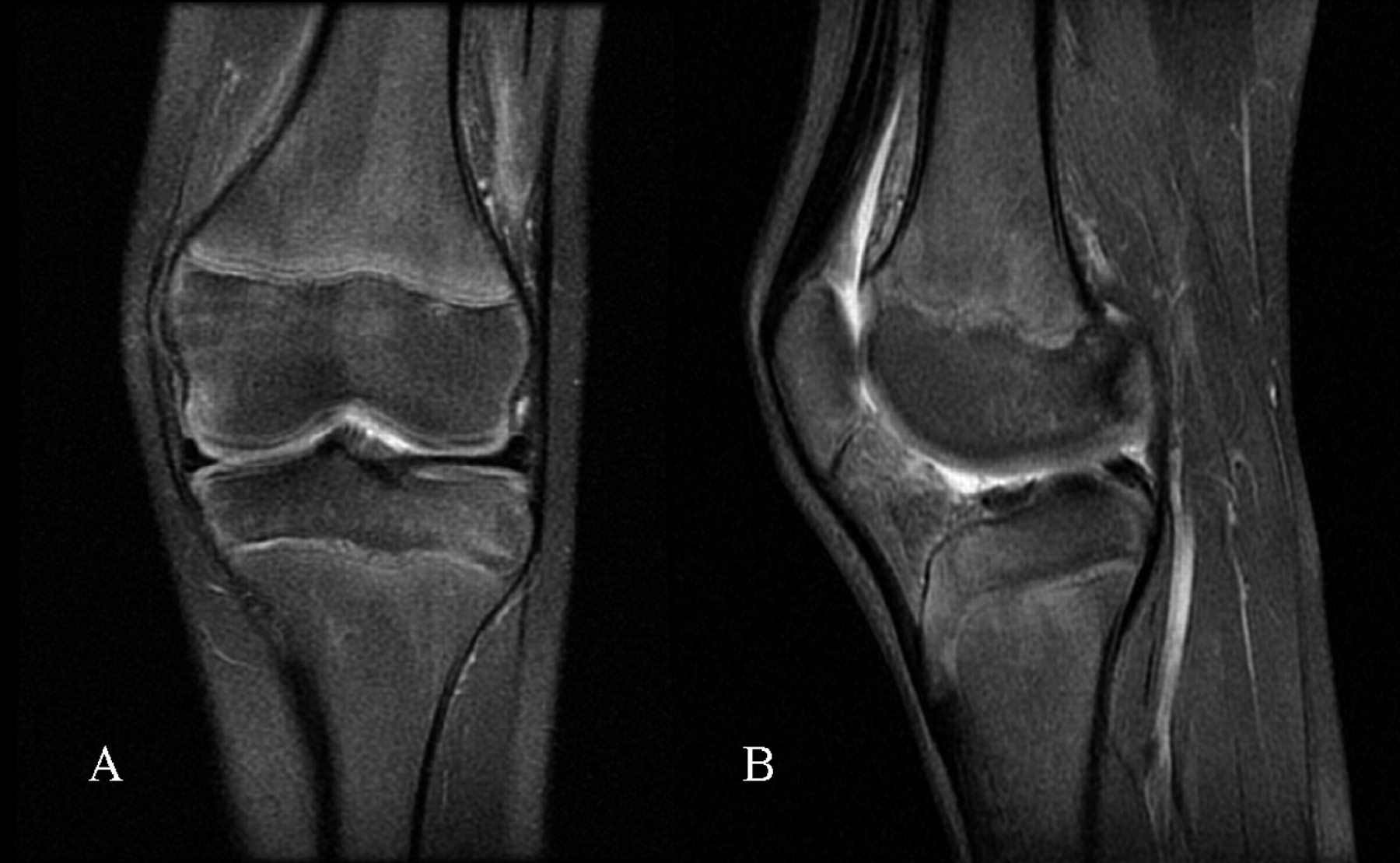
Arthroscopic anterior synovectomy of the knee was performed under constant irrigation. With use of punches and graspers, eight fragments of the proliferating lesion were taken from different compartments of the knee. All villous projections were then resected under direct vision with use of a 4.5-mm shaver. Following the synovectomy, arthroscopic inspection confirmed complete excision of the lesion. Histology All of the samples were similar and consisted of polypoid synovium with lobules of mature fat in the subsynovial tissue (Fig. 2-A). Small amounts of inflammatory cells, lymphocytes, and plasma cells were observed around capillaries (Fig. 2-B). Although these pathological findings of villous lipomatous proliferation of the synovial membrane are not specific by themselves, they do support the diagnosis of lipoma arborescens when considered in the clinical and imaging context. The postoperative course was uneventful. One month after the arthroscopic synovectomy, the swelling of the left knee had resolved and the patient had no symptoms and had regained the preoperative range of motion. Two months after the procedure, the patient renewed sport activities. At the time of this report, he had been followed for one year and had had no recurrence of symptoms. He had no limitations of activities, and the range of motion of the left knee was normal. Magnetic resonance imaging showed a minimal joint effusion without patterns of recurrence (Fig. 3). At the latest follow-up, the contralateral, right knee was not painful, had a normal range of motion, and had had no swelling for the previous ten months. As of this writing, no surgical procedure had been scheduled for the right knee.
Proceed to Discussion >>Reference: Sailhan F, Hautefort P, Coulomb A, Mary P, Damsin JP. Bilateral lipoma arborescens of the knee. A case report. J Bone Joint Surg Am. 2011;93:195-198.
Lipoma arborescens, first described in detail by Arzimanoglu, is an uncommon synovial disorder that most often presents during the fourth or fifth decade of life and seems to have an equal predilection for men and women. The knee is the most common site of involvement, although the hip, wrist, elbow, or ankle can be affected. Most cases of lipoma arborescens have similar presenting clinical characteristics, including the insidious onset of painless knee swelling followed by progressive intermittent pain. Mechanical symptoms of locking and popping are rare. Pain and limitation of the range of motion may develop progressively as joint effusion and/or fatty tissue increases in volume. Patients are usually symptomatic for several years. When this disease occurs in the knee, it often affects the suprapatellar pouch. The lesion is soft in consistency and is not tender to palpation. This condition usually occurs unilaterally. The clinical differential diagnosis of lipoma arborescens of the knee includes pigmented villonodular synovitis, a true intra-articular lipoma, synovial chondromatosis, synovial hemangioma, rheumatoid arthritis, and chronic inflammatory synovial proliferation. In the case of pediatric patients, chronic joint effusion and pain can be caused by various disorders, such as juvenile rheumatoid arthritis, acute rheumatic fever, vascular malformation, Behçet syndrome, meniscal malformation, or synovial chondromatosis. In the case of the patient in this report, these different diagnoses were ruled out through the combined use of imaging and laboratory studies. The published literature regarding lipoma arborescens mostly contains reports of unilateral cases. We are aware of only eleven cases of bilateral lipoma arborescens reported in the English literature. Bilateral involvement has been reported to occur in 20% of affected patients in some studies. Since lipoma arborescens is rare in children, especially when it involves both of the knee joints, it can easily be overlooked. The laboratory findings are generally unremarkable. The joint aspirate is negative for crystals, and cultures of the fluid are sterile. Plain radiographs may appear normal or show a soft-tissue density in the suprapatellar pouch; however, they may also show cyst formation, subchondral bone erosions, or osteoarthritic changes. Subchondral bone erosions may indicate synovial invasion. The appearance of lipoma arborescens on magnetic resonance imaging is likely to be of greater help in the preoperative diagnosis, as magnetic resonance imaging is the gold standard for the diagnosis of this condition. Magnetic resonance imaging shows a villous-like synovial mass with a signal intensity similar to that of fat on all sequences and also reveals the frondlike architecture. There is usually an associated joint effusion and no evidence of hemosiderin deposition. In contrast, pigmented villonodular synovitis typically demonstrates low signal intensity on both T1-weighted and T2-weighted scans. Imaging findings should be correlated with histology to confirm the diagnosis. Macroscopically, lipoma arborescens comprises broad-based polypoidal, grapelike, or fingerlike villi with a yellowish appearance. Histologically, there is abundant subsynovial mature adipose tissue with a diffuse distribution. In contrast, intra-articular lipoma represents a localized solitary defined tumorlike mass of adipose tissue with a round or oval contour. Also, an intra-articular lipoma, which may be covered by synovium, does not arise from or replace the subsynovial layer. Matsumoto et al. showed that many vessels are present beneath the capsule of the lipoma, accounting for capsular enhancement on magnetic resonance imaging. Neither villous proliferation of the synovial tissue nor fatty replacement of the underlying connective tissue should be seen. The recommended treatment for symptomatic lipoma arborescens is synovectomy. Arthroscopy preceding arthrotomy has been used for the diagnosis in several reported cases, but few authors have reported cases of lipoma arborescens of the knee treated by arthroscopic synovectomy alone. For the few patients treated with arthroscopic anterior synovectomy, the reported outcomes have been favorable at six months, one year, and two years. Arthroscopic treatment with a mini-open approach may also be performed to resect all of the suprapatellar mass. If the lesion is limited to the anterior compartment of the knee and, furthermore, if it is limited to the suprapatellar pouch, then it is amenable to arthroscopic resection. The etiology of lipoma arborescens remains unknown, and developmental, traumatic, inflammatory, or neoplastic origins have been postulated. A synovial reaction to a traumatic injury has been proposed, but most patients who have lipoma arborescens do not have a history of trauma. Jaffe suggested that it represents a nonneoplastic villous synovial proliferation in response to chronic irritation of the synovium. Most authors have accepted this hypothesis, as there is an association between lipoma arborescens and degenerative joint disease. In a retrospective series of thirty-two cases of lipoma arborescens, Vilanova et al. found that, on magnetic resonance imaging, 87% of the patients showed associated degenerative changes of the joint and 72% had a meniscal tear. The study by Vilanova et al. included mostly elderly patients, however, and a causal relationship is difficult to establish. Although rare and benign, bilateral lipoma arborescens of the knee should be considered in the differential diagnosis of bilateral swelling of the knee in children. When the condition causes pain and discomfort, surgical management is advocated and can be performed during an arthroscopic procedure (arthroscopic synovectomy).
Reference: Sailhan F, Hautefort P, Coulomb A, Mary P, Damsin JP. Bilateral lipoma arborescens of the knee. A case report. J Bone Joint Surg Am. 2011;93:195-198.
Lipoblastoma
Liposarcoma
Lipoma arborescens
Intra-articular lipoma