A Thirty-eight-Year-Old Woman with Left Wrist Pain
November 7, 2012



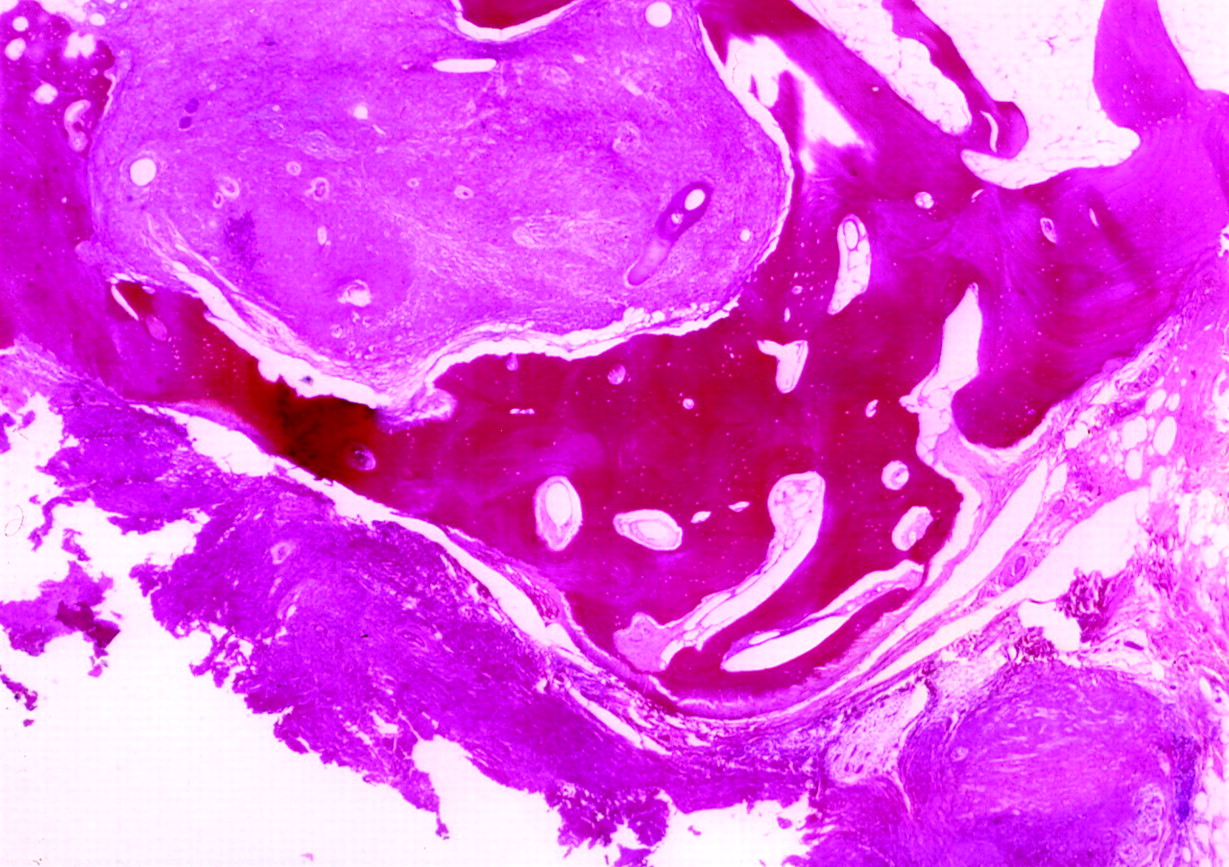
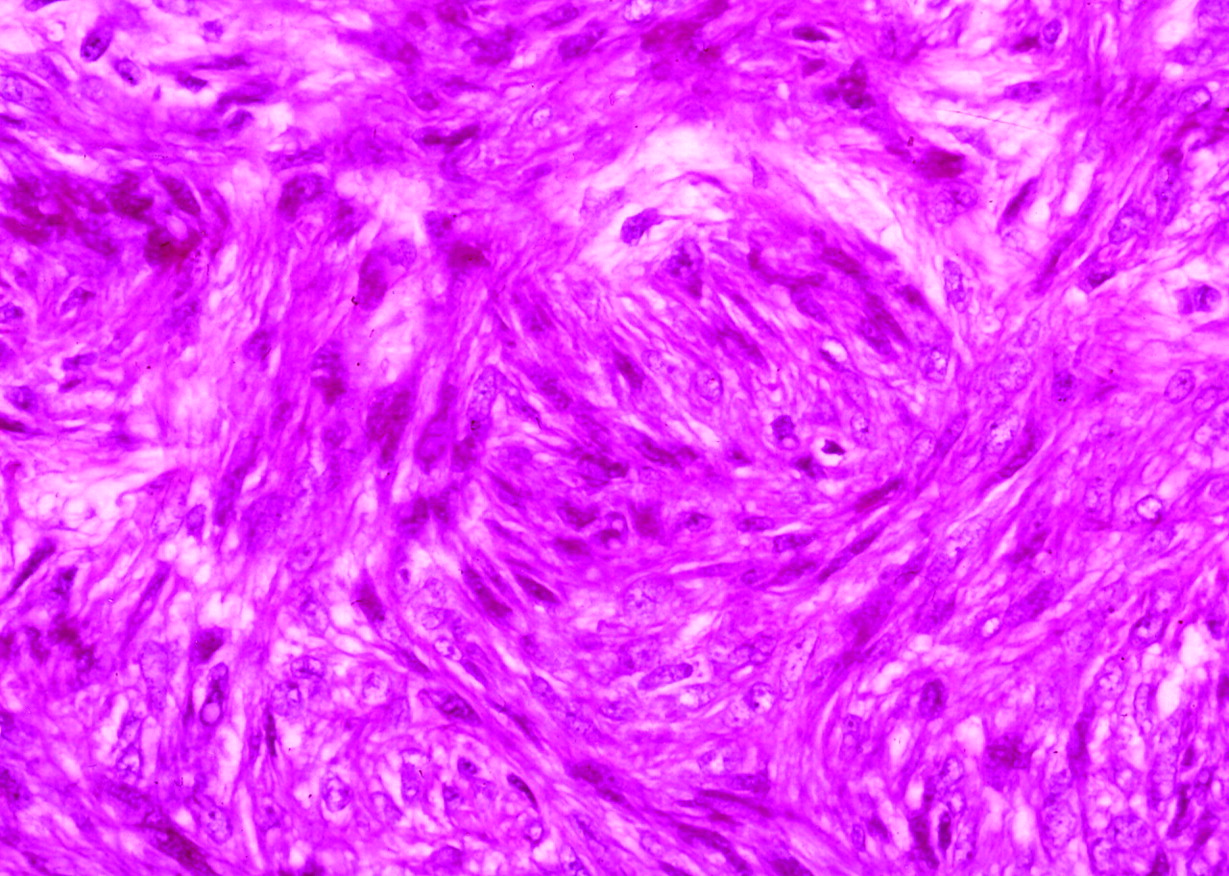
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5A thirty-eight-year-old, left-hand-dominant woman presented with a ten-year history of ulnar pain in the left wrist. The medical history, including that for gynecological disorders, was negative. Initially, the pain had been mild, but four years before the patient presented at our institution, the symptoms began to worsen. The patient took nonsteroidal anti-inflammatory medication for approximately three months, with transient relief of symptoms. However, two years later, the pain again worsened and began to limit the range of motion of the left wrist and forearm. Physical examination revealed moderate, diffuse swelling along the ulnar dorsal aspect of the left wrist. Palpation of the distal aspect of the ulna caused extreme pain that was centered mostly about the ulnar styloid and the region of the sixth dorsal compartment. No mass was discernable, but the distal aspect of the ulna appeared mildly prominent. Radiographs of the left wrist (Fig. 1) demonstrated an enlarged ulnar styloid but no other skeletal abnormality. The patient was diagnosed with extensor carpi ulnaris tenosynovitis and was treated with an injection of corticosteroid medication into the sixth extensor compartment. She was given a wrist immobilizer, and a course of nonsteroidal anti-inflammatory medication was prescribed. Three years later, the patient presented with wrist pain once again, but this time with a more restricted range of motion of the wrist. A magnetic resonance imaging scan showed nonspecific expansion of the ulnar styloid without evidence of a discernable mass (Fig. 2). There was also no evidence of a soft-tissue or periosteal lesion, and no medullary signal changes were noted. A computed tomographic scan (Fig. 3) revealed only cortical irregularities along the distal aspect of the ulna and enlargement of the ulnar styloid. The differential diagnosis at the time included periosteal chondroma, osteochondroma, osteoid osteoma, giant-cell tumor, and chronic stenosing tenosynovitis of the sixth extensor compartment. Because of the increasing pain and limitation of function in conjunction with the radiographic abnormalities seen at the distal aspect of the ulna, surgical exploration was scheduled. During the surgery, a localized cortical expansion at the base of the ulnar styloid was identified. An en bloc excision of the mass was performed and included a 1 to 2 mm margin of normal-appearing bone. The mass contained an ovoid, pink, subcortical intramedullary lesion that measured approximately 8 mm at its longest dimension. The histological photomicrographs of the lesions are shown in Figures 4 and 5.
Histologic evaluation of the mass showed bone with a well-demarcated intramedullary tumor. The tumor cells were predominantly spindle-shaped with a rate of mitosis between zero and four per ten high-power fields and a mean mitotic count of two. There was moderate cellularity and no necrosis. Immunochemistry revealed the tumor to be positive for smooth-muscle actin and vimentin. The alpha-smooth-muscle actin stain was strong, diffuse, and unequivocal. The tumor showed negative staining for AE1/3 (a broad-spectrum marker of epithelial cytokeratins), CD34 (a marker that is often positive in mesenchymal tumors), CD117 (a marker that is commonly positive in gastrointestinal stromal tumors), and S100 (a marker that is often positive in tumors of nerve or nerve sheath or in those that originate from melanomas). The tumor was also negative for MAC387 and CD68, which are histiocytic markers and may be positive in fibrohistiocytic tumors. The diagnosis of a benign intraosseous leiomyoma was made. Two months after the operation, the patient had no pain in the wrist. There was substantial improvement in the range of motion in all planes, with wrist flexion to 65°, extension to 40°, and full pronation and supination. Two years after surgery, there was no evidence of recurrence of the tumor.
Proceed to Discussion >>Reference: Zikria BA, Radevic MR, Jormark SC, Huvos AG, Yang SS. Intraosseous leiomyoma of the ulna. A case report. J Bone Joint Surg Am. 2004 Nov;86(11):2522-5.
Leiomyomas are extremely rare in bone. Neviaser and Newman, in probably the largest series of upper-extremity leiomyomas described to date, reported on twenty-four leiomyomas of the hand and forearm seen over an eighteen-year period. Yet, there were no intraosseous leiomyomas among these cases. In his series of eight smooth-muscle tumors of bone, Mirra described one benign leiomyoma that involved the periosteum of the tibia; the rest were leiomyosarcomas. Tomoda and Iyama described an expansively growing angioleiomyoma within the proximal aspect of the tibia of a sixty-four-year-old woman. The authors claimed that this was the first report of an intraosseous leiomyoma in any extremity. Braun et al. reported an intraosseous leiomyoma in the femoral neck of a woman with a history of disseminated leiomyomatosis. She had previously undergone resection of a free peritoneal leiomyoma one year after a hysterectomy that was performed as treatment for a uterine leiomyoma. She subsequently had additional benign smooth-muscle lesions removed from the omentum. The remaining two reported cases of leiomyomas of bone involved the mandible. The histologic differential diagnosis for an intraosseous leiomyoma includes benign neural or fibrous lesions as well as leiomyosarcoma. Immunohistochemistry can be helpful in differentiating the histologic type of tumor. In the case of our patient, the tumor was positive for smooth-muscle actin and vimentin and negative for markers of epithelial and neural origin. Although leiomyomas of bone are rare, leiomyosarcomas may be somewhat more common. The criteria for distinguishing benign from malignant smooth-muscle tumors in bone have not been established; however, mitotic activity, cytologic atypia, and necrosis are the most important factors when these tumors arise in soft tissue. The tumor in our patient had rare mitoses and no atypical mitoses. Moreover, the small size and long duration of this lesion meant that a malignant disease was unlikely. To our knowledge, intraosseous leiomyoma in the upper extremity has not been reported previously. Smooth-muscle tumors in bone are rare but must be considered in the differential diagnosis of a symptomatic intraosseous lesion. Leiomyomas of bone can present with pain and radiographic evidence of an expansile, sometimes lytic lesion. Marginal excision is typically curative, and recurrences are uncommon.
Reference: Zikria BA, Radevic MR, Jormark SC, Huvos AG, Yang SS. Intraosseous leiomyoma of the ulna. A case report. J Bone Joint Surg Am. 2004 Nov;86(11):2522-5.
Leiomyoma
Low-grade fibrosarcoma
Fibrous dysplasia
Neurilemmoma
Low-grade spindle cell sarcoma