A Twenty-eight-Year-Old Woman with Right Hand Mass
June 5, 2013


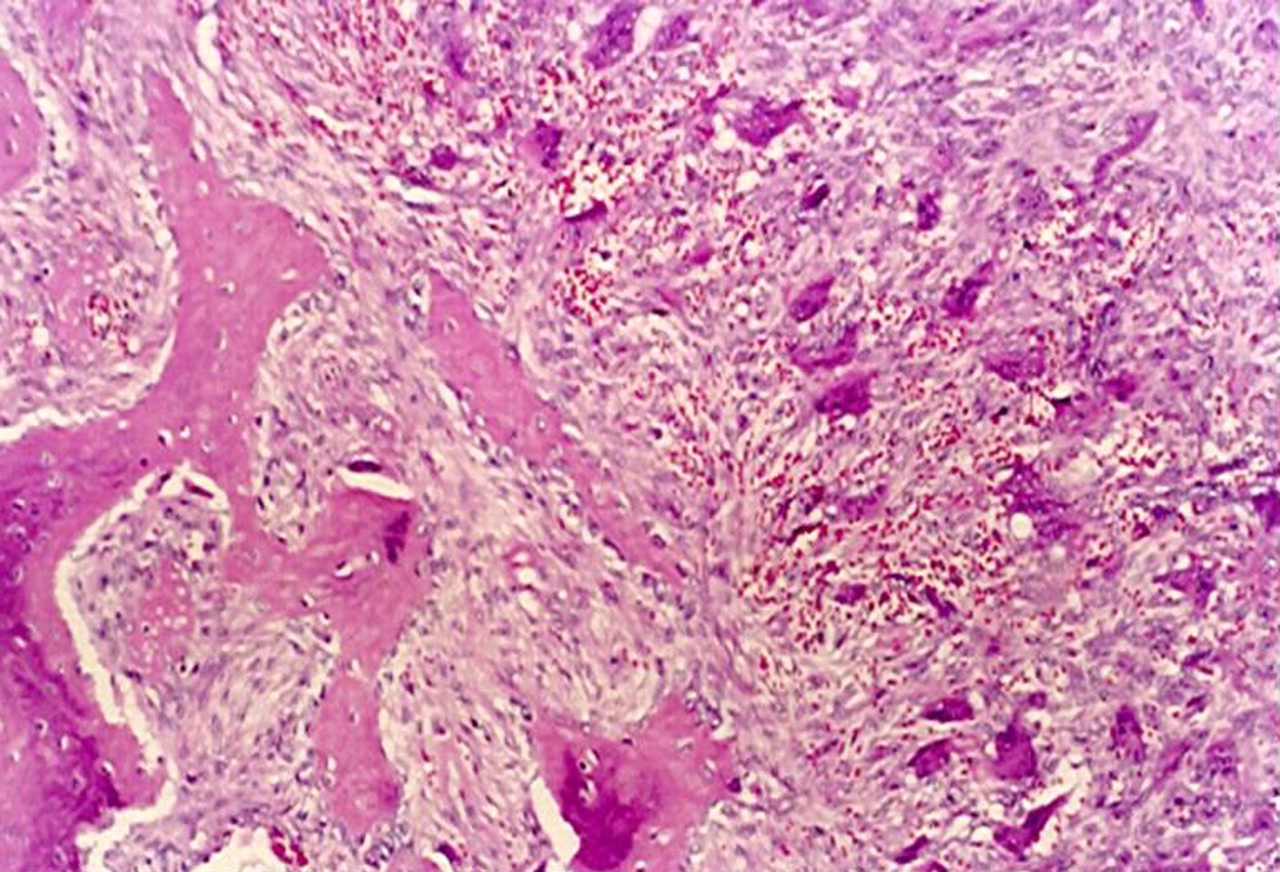

 Fig. 1
Fig. 1 Fig. 2
Fig. 2  Fig. 3-A
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 3-A
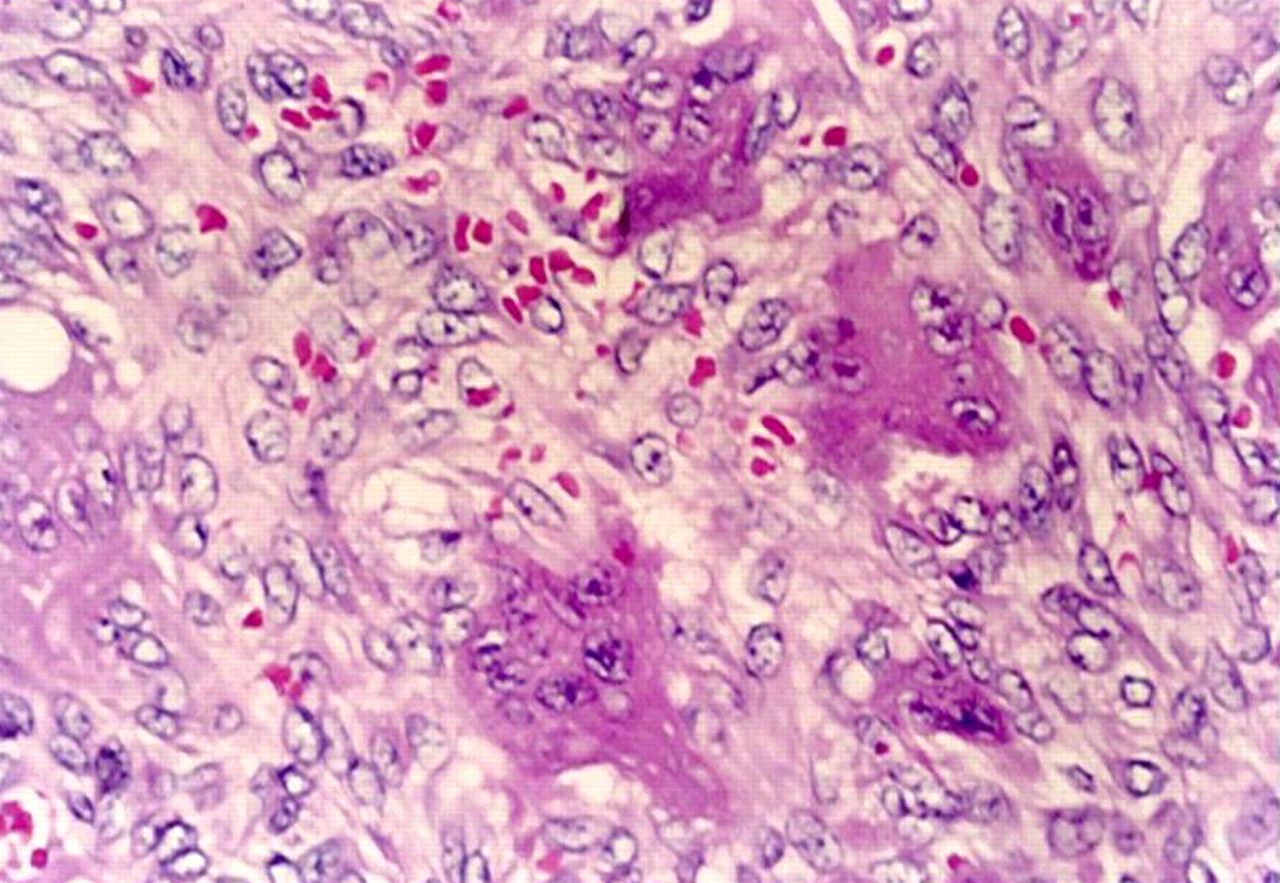
Fig. 3-A Fig. 3-B
Fig. 3-B Fig. 4
Fig. 4A twenty-eight-year-old woman who had been in purdah (no skin exposed in public except the hands and face) since she was thirteen years old presented with a 4 × 3-cm painful mass in the region of the fourth metacarpal of the right hand without redness or warmth (Fig. 1). Her hand movement was extremely restricted. Radiographs revealed an expansile lytic lesion of the fourth metacarpal as well as subperiosteal bone resorption of the phalanges (Fig. 2). Laboratory evaluation showed a serum level of calcium of 8.3 mg/dL (2.07 mmol/L) (normal, 8.5 to 10.2 mg/dL [2.12 to 2.54 mmol/L]), phosphate of 2.9 mg/dL (0.94 mmol/L) (normal, 2.5 to 4.5 mg/dL [0.81 to 1.45 mmol/L]), and alkaline phosphatase of 834 IU/L (normal, 50 to 140 IU/L); a urinary calcium of 87 mg/24 h (2.2 mmol/d) (normal, 80 to 320 mg/24 h [2.0 to 8.0 mmol/d]); and urinary phosphate of 276 mg/24 h (0.276 g/24 h or 9 mmol/d) (normal, 250 to 1000 mg/24 h [0.25 to 1.0 g/24 h or 8 to 32 mmol/d]). The results of liver and kidney function tests were normal. Dual x-ray absorptiometry showed a substantial reduction in bone mineral density (a Z score of −3.0 in the lumbar spine). A skeletal survey revealed a few other lytic lesions in the pubis. A technetium bone scan revealed increased uptake in the fourth metacarpal, the right pubic ramus, the calvaria, the mandible, and the sternoclavicular and costochondral junctions. She was not taking any medication and had no history of steatorrhea. She described very little ingestion of food that was rich in vitamin D. The patient had had weakness and a lack of energy on walking, especially on climbing stairs, for the last year. The expansile lesion of the fourth metacarpal was curetted, and histologic examination was performed (Figs. 3-A and 3-B).
Histologic examination revealed multinuclear giant cells adjacent to hemosiderin granules, consistent with a brown tumor (Figs. 3-A and 3-B). After the histologic diagnosis was made, the serum intact parathyroid hormone level was 777 pg/mL (780 ng/L) (normal, 10 to 72 pg/mL [10 to 70 ng/L]), while the 25-hydroxycalciferol level was 5 ng/mL (normal, 10 to 60 ng/mL). Oral calcitriol (0.5 µg daily) and elemental calcium (3 g daily) supplementation was commenced for two weeks until the serum vitamin-D levels and histopathologic evaluation were obtained. Three hundred thousand units of vitamin D was administered intramuscularly once. After discharge from the hospital, she was managed with ergocalciferol (1000 U daily) and oral calcium (1000 mg daily). Biochemical analysis performed three months later revealed a serum calcium level of 9.6 mg/dL (2.40 mmol/L), a phosphate level of 3.5 mg/dL (1.13 mmol/L), an alkaline phosphatase level of 156 IU/L, and a serum intact parathyroid hormone level of 78 pg/mL (80 ng/L). Over the next year, while maintaining the same dose of calcium and vitamin D, the patient had improvement in her level of energy and the radiographic changes of osteitis fibrosa cystica in the metacarpal and pubis regressed (Fig. 4). Serum calcium and phosphate levels were normal, but the serum parathyroid hormone level remained minimally elevated.
Proceed to Discussion >>Reference: Erturk E, Keskin M, Ersoy C, Kaleli T, Imamoglu S, Filiz G. Metacarpal brown tumor in secondary hyperparathyroidism due to vitamin-D deficiency. A case report. J Bone Joint Surg Am. 2005 Jun;87(6):1363-6.
Brown tumors are locally destructive bone lesions caused by rapid osteoclastic bone resorption due to severe hyperparathyroidism. For years, brown tumors have been considered to be characteristic of primary hyperparathyroidism. However, brown tumors also have been reported to occur in patients with severe hyperparathyroidism secondary to chronic renal failure, especially those on long-term hemodialysis. Hypocalcemia, hyperphosphatemia, and vitamin-D deficiency are the basic characteristics of chronic renal failure associated with secondary hyperparathyroidism. Osteomalacia is rare in developed countries, but it is still a problem in some areas of the world. Dietary deficiency of vitamin D and lack of exposure to sunlight are the main causes. Debilitated people living indoors, people living in high altitudes, individuals with malabsorption, and veiled women are at risk of a vitamin-D deficiency. The prevalence of vitamin-D deficiency in the Asian immigrant population in the United Kingdom has been reported to be as high as 24%. In a recent Australian study, 80% of eighty-two veiled or dark-skinned pregnant women were found to have a vitamin deficiency.
Reference: Erturk E, Keskin M, Ersoy C, Kaleli T, Imamoglu S, Filiz G. Metacarpal brown tumor in secondary hyperparathyroidism due to vitamin-D deficiency. A case report. J Bone Joint Surg Am. 2005 Jun;87(6):1363-6.


Brown tumor
Giant cell tumor
Aneurysmal bone cyst
Reparative granuloma
Cherubism