A Twenty-six-Year-Old Woman with Right Thigh Pain
January 18, 2012
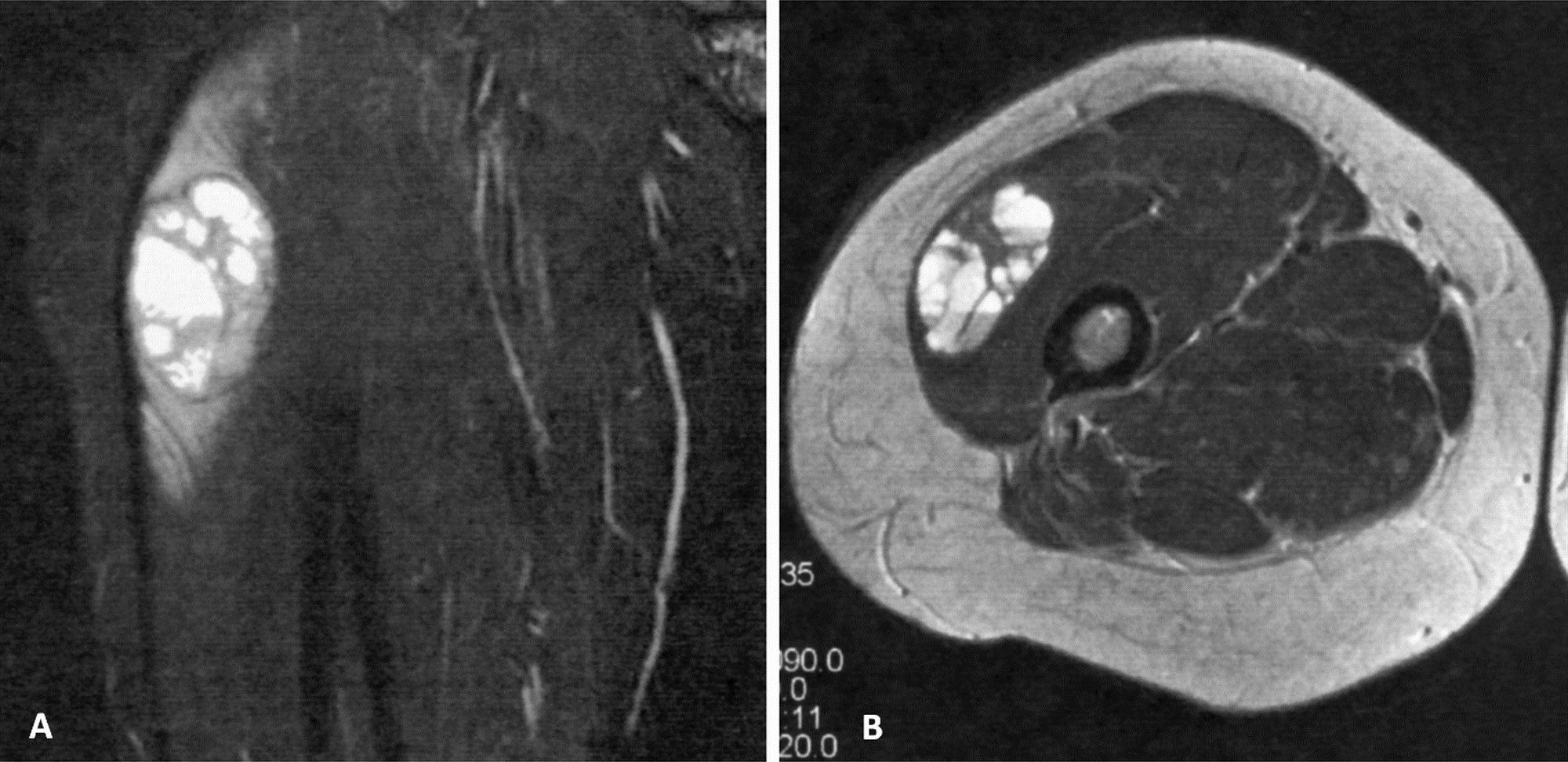

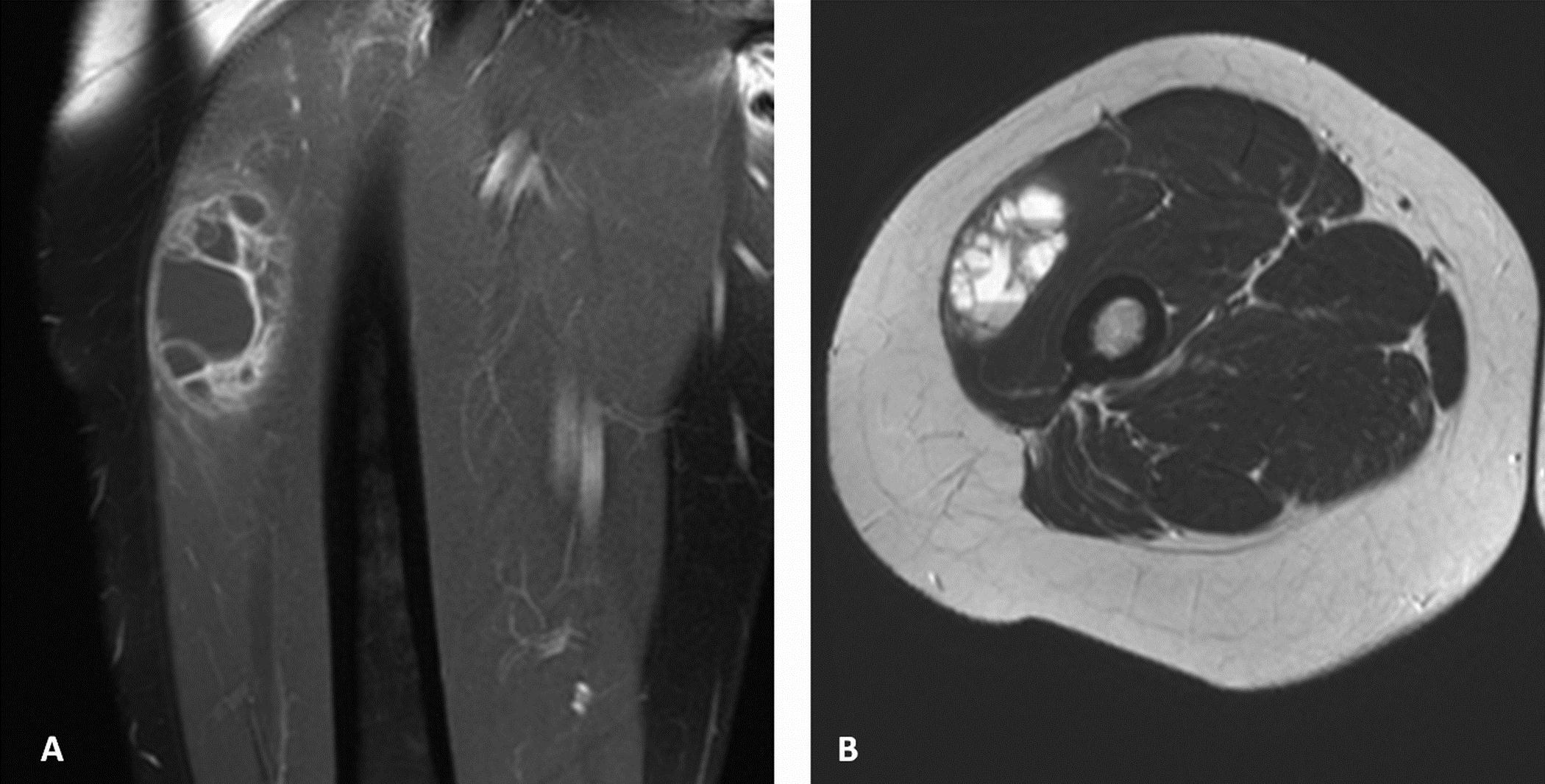
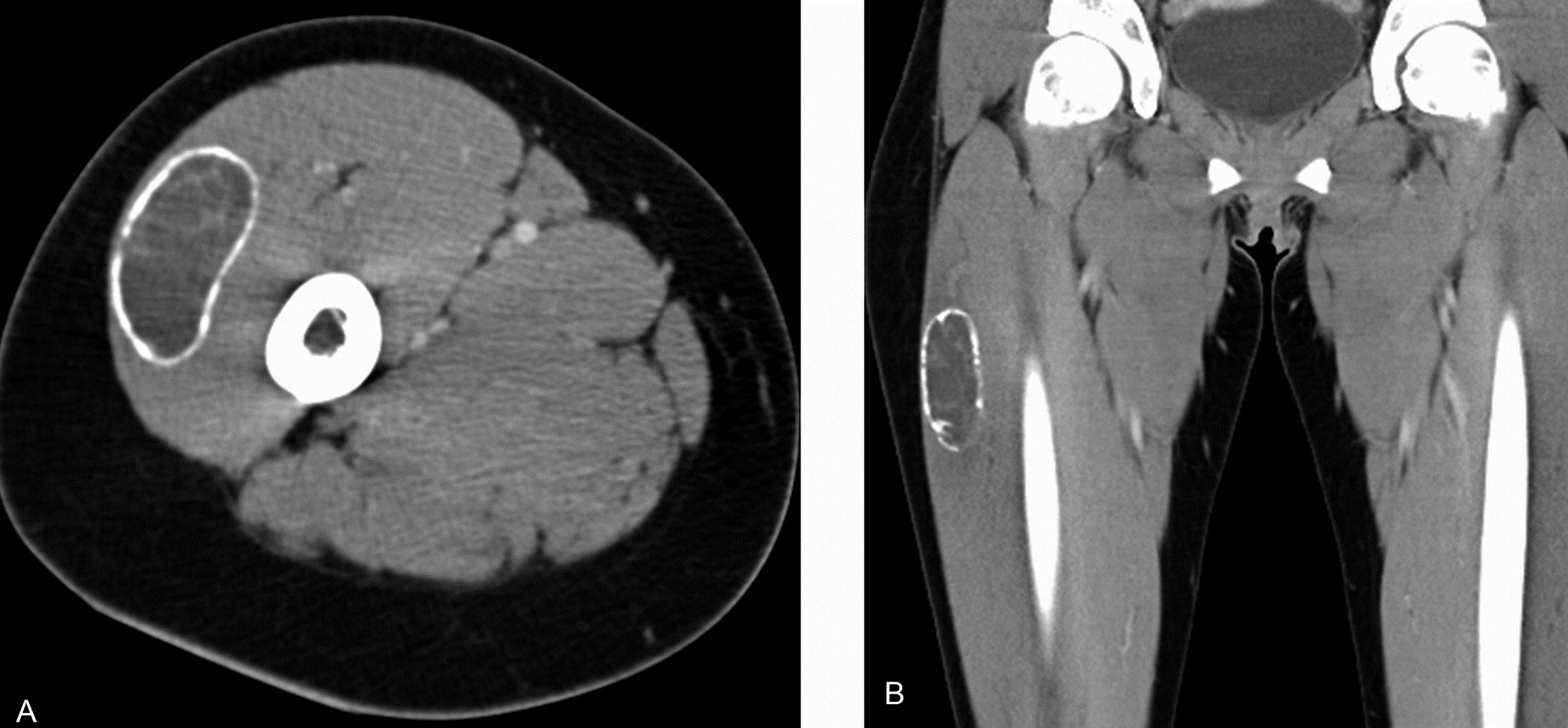

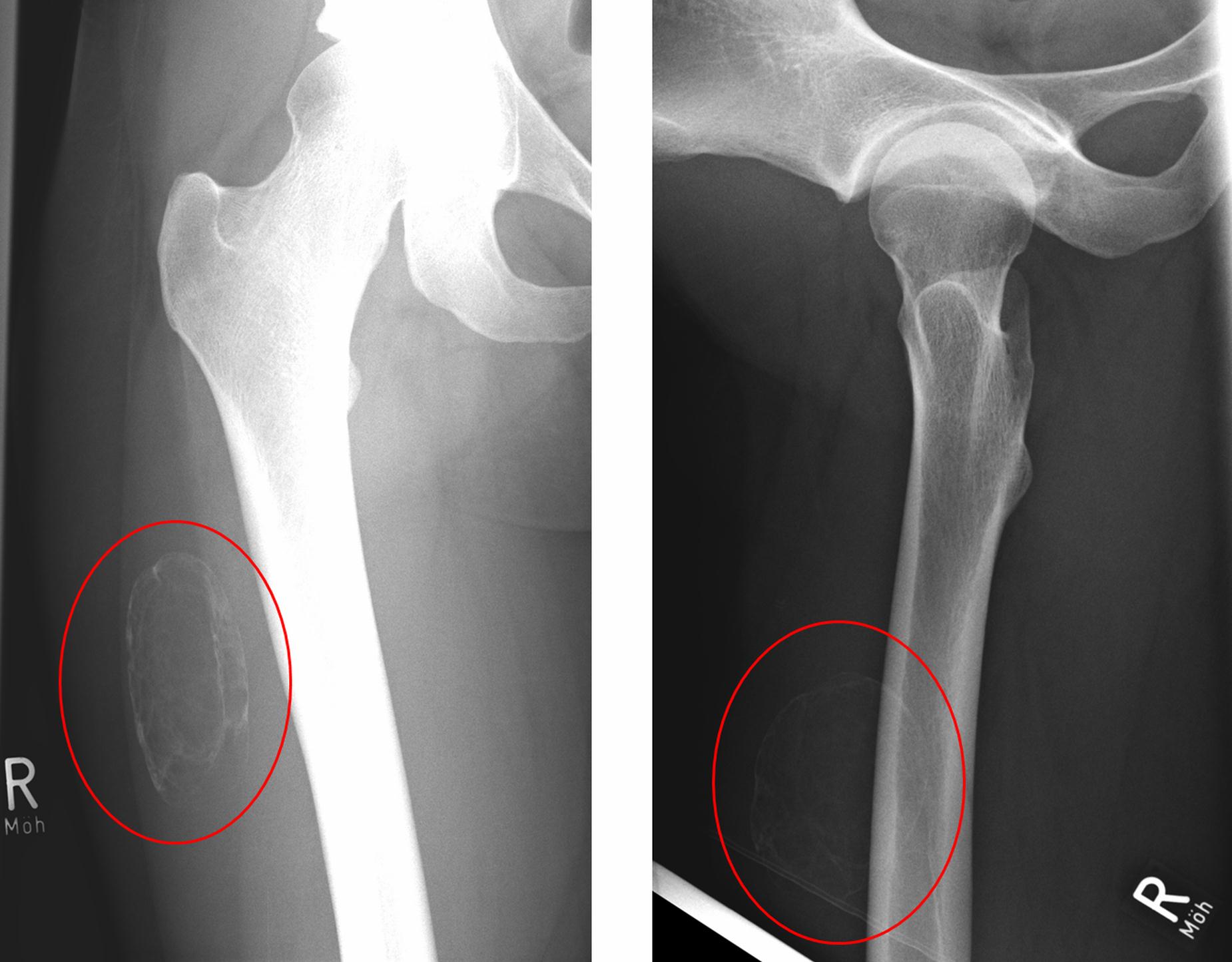
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 Fig. 2
Fig. 2 Fig. 5
Fig. 5 Table I
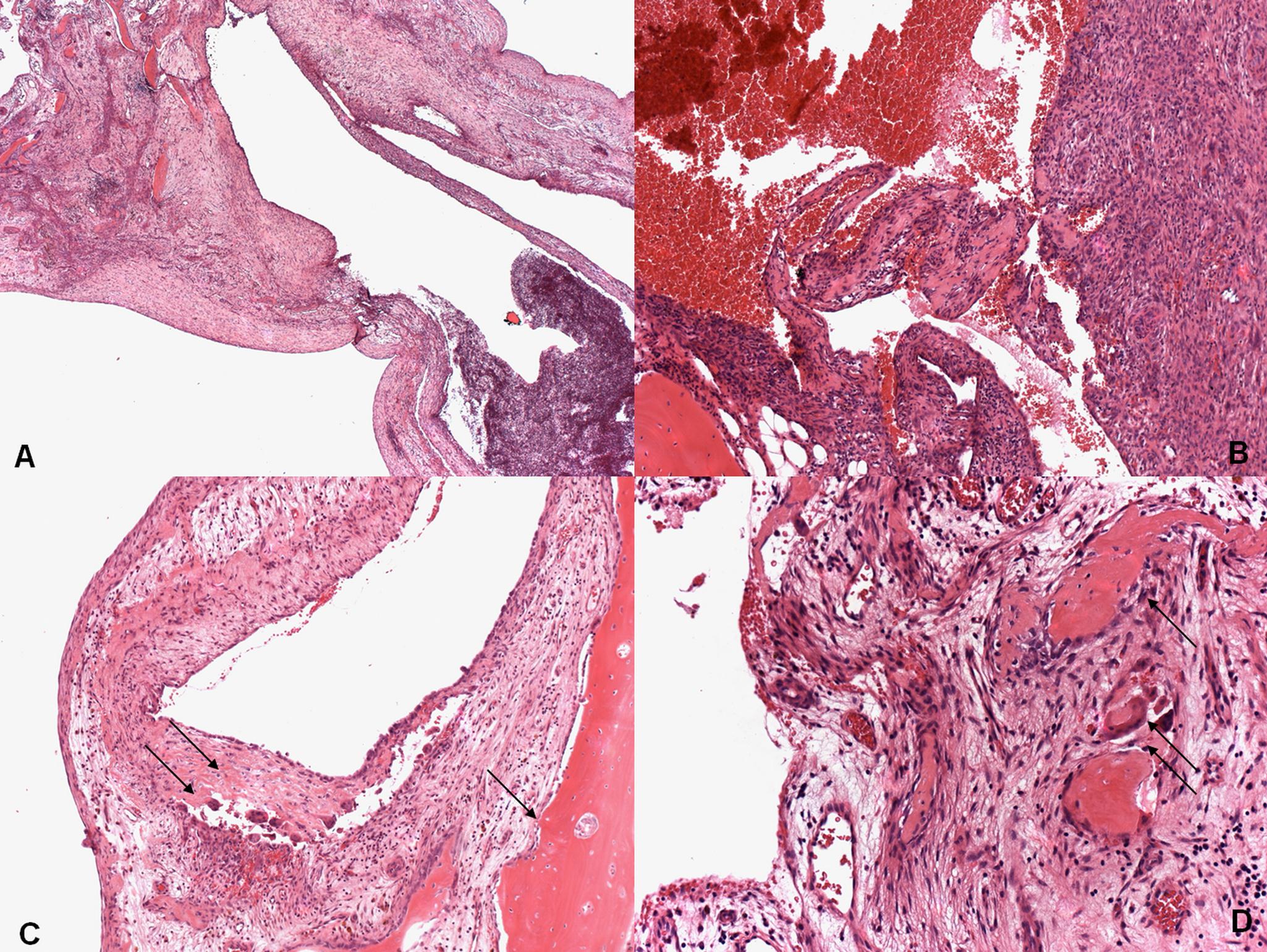
Table IA twenty-six-year-old woman had a two-month history of pain in the right thigh. Although she worked in a gym, no specific traumatic event was identified. On examination, a painful lump, 7 × 5 cm, was identified in the anterolateral aspect of the right thigh. There was no sign of inflammation, and the findings on examination were otherwise unremarkable. Radiographs showed a mass with a thin peripheral shell of ossification not connected to bone. Magnetic resonance imaging (MRI) showed a mass with multiloculated cystic spaces in the superficial aspect of the vastus lateralis muscle (Fig. 1). As there was no sign of malignant disease, it was decided to follow the patient. Four months later, the patient reported a change in the pain and consistency of the lesion. Radiographs and computed tomography (CT) revealed increased ossification (Figs. 2, 3, and 4), and follow-up MRI showed an increase in the size of the lesion. Marginal excision of the lesion was performed. A histological photomicrograph of the lesion is seen in Figure 5.
The diagnosis of soft-tissue aneursymal bone cyst was made (Fig. 5). After recovery from the surgery, the patient remained free of pain and recurrence, with unrestricted physical activity, as noted at the time of the latest follow-up, at thirty-six months.
Proceed to Discussion >>Reference: Pietschmann MF, Oliveira AM, Chou MM, Ihrler S, Niederhagen M, Baur-Melnyk A, Dürr HR. Aneurysmal bone cysts of soft tissue represent true neoplasms. A report of two cases. J Bone Joint Surg Am. 2011;93:e45(1-8).
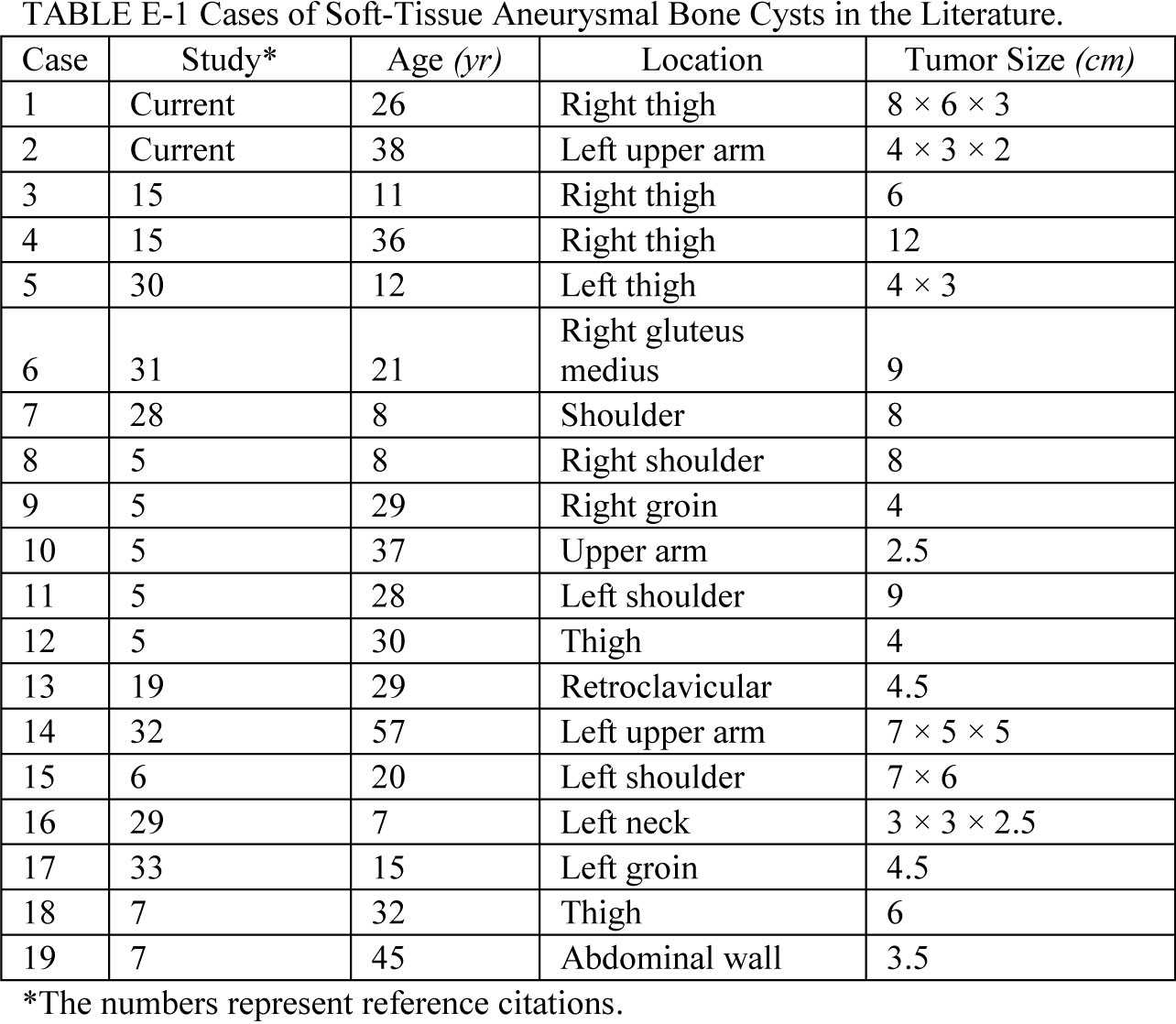
The first two cases of soft-tissue aneurysmal bone cyst were probably reported by Salm and Sissons in 1972. The number of published cases does not exceed twenty (Table I), with only a few epidemiological and histological reports. The appearance of soft-tissue aneurysmal bone cyst on radiographs and CT scans may be similar to that of myositis ossificans, but on MRI scans the presence of septa within the lesion and fluid-fluid levels help to differentiate it from myositis ossificans. Nevertheless, it can be difficult to distinguish myositis ossificans from soft-tissue aneurysmal bone cyst on the basis of radiographic features in some cases. Ossifying fibromyxoid tumor sometimes presents radiographically with bone formation at its periphery and can mimic soft-tissue aneurysmal bone cyst. Also, extraskeletal telangiectatic osteosarcoma may have fluid-fluid levels within the lesion similar to those of soft-tissue aneurysmal bone cyst. Histological features of soft-tissue aneurysmal bone cysts are indistinguishable from those of aneurysmal bone cysts within bone. The histological differential diagnosis of soft-tissue aneurysmal bone cyst includes giant-cell-rich and cystic lesions of soft tissue, which can be problematic. These lesions include benign conditions such as nodular fasciitis, ossifying fibromyxoid tumor, and giant-cell tumor of the tendon sheath as well as potentially malignant or malignant lesions such as giant-cell tumor of soft tissue and the telangiectatic subtype of extraskeletal osteosarcoma. Aneurysmal bone cysts have been shown to have recurrent rearrangements of the USP6 gene on chromosome 17p13. USP6—also known as TRE2 or TRE17—was first identified as a potential oncogene on the basis of its transforming properties when NIH-3T3 cells were transfected with Ewing sarcoma DNA. It encodes a ubiquitin-specific protease (USP) and a TBC domain that mediates binding to the Arf6 GTPase. USP6 has effects on cell adhesion and actin remodeling. Oliveira et al. reported, in 2004, that the product of this chromosomal translocation creates a fusion gene in which the osteoblast cadherin 11 gene (CDH11) promoter region on 16q22 is juxtaposed to the entire ubiquitin-specific protease USP6 (Tre2) coding sequence on 17p13. The fusion gene CDH11-USP6 and that USP6 rearrangement are specific for primary aneurysmal bone cyst and are not found in the so-called secondary aneurysmal bone cyst, which is commonly associated with giant-cell tumor, chondroblastoma, osteoblastoma, and fibrous dysplasia. Rearrangements of USP6 have been found in approximately 70% of aneurysmal bone cysts (70% sensitivity) but have not been found in other tumors (100% specificity). Petrik et al. described an aneurysmal bone cyst-like reaction in the left carotid artery bifurcation in an otherwise healthy seven-year-old. Since that time, there have been fewer than twenty case reports of soft-tissue aneurysmal bone cysts in the literature. The histological features of soft-tissue aneurysmal bone cyst are identical to those of intraosseous aneurysmal bone cyst except for its extraosseous location. Histological features of aneurysmal bone cyst overlap with those of other osseous lesions such as myositis ossificans, cherubism, and brown tumor. In a 2008 study, Sukov et al. looked for USP6 rearrangements in soft-tissue aneurysmal bone cyst, myositis ossificans, cherubism, and brown tumor and found no such rearrangements in cherubism or brown tumor. However, molecular cytogenetic studies revealed USP6 rearrangement in two of twelve specimens previously classified as myositis ossificans on the basis of their radiographic appearance. One of the two patients presented initially with classic radiographic features of myositis ossificans, but the radiographic appearance changed to that of an aneurysmal bone cyst over time. It is also of interest that no inciting trauma could be identified for this patient. These data reported by Sukov et al. were verified by the analysis of our patient, who had USP6 rearrangements and no history of trauma. Nielsen et al. reported five cases of soft-tissue aneurysmal bone cyst, with no patient having a known history of trauma. Nielsen et al. reported only one recurrence in their five patients with soft-tissue aneurysmal bone cyst, in whom an intralesional resection had been performed. The other four patients had been free of recurrence for sixteen months to ten years, findings in concordance with those in other reports of a long disease-free survival after resection of soft-tissue aneurysmal bone cyst. Given that soft-tissue aneurysmal bone cyst may be confused with other, similarly appearing lesions on radiographs, we believe that soft-tissue aneurysmal bone cyst might be more frequent than one would assume on the basis of the published literature. Therefore, fluorescence in situ hybridization analysis of USP6 rearrangement could be a very helpful tool for differentiating soft-tissue aneurysmal bone cyst from other soft-tissue tumors, especially myositis ossificans.
Reference: Pietschmann MF, Oliveira AM, Chou MM, Ihrler S, Niederhagen M, Baur-Melnyk A, Dürr HR. Aneurysmal bone cysts of soft tissue represent true neoplasms. A report of two cases. J Bone Joint Surg Am. 2011;93:e45(1-8).
Myositis ossificans traumatica
Ossifying fibromyxoid tumor
Aneursymal bone cyst of soft tissue
Brown tumor