An 81-Year-Old Woman with the Inability to Walk After a Fall
July 7, 2022



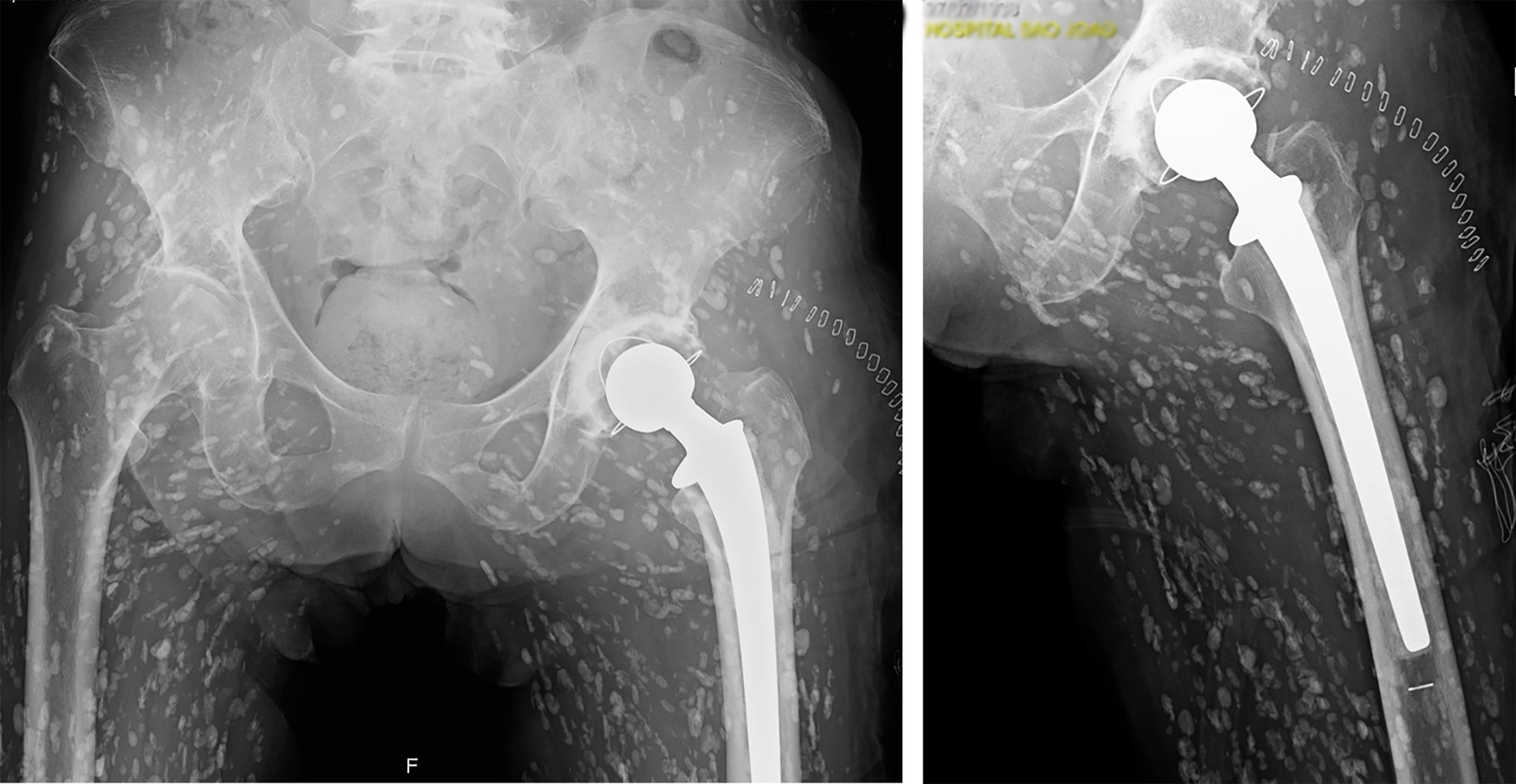
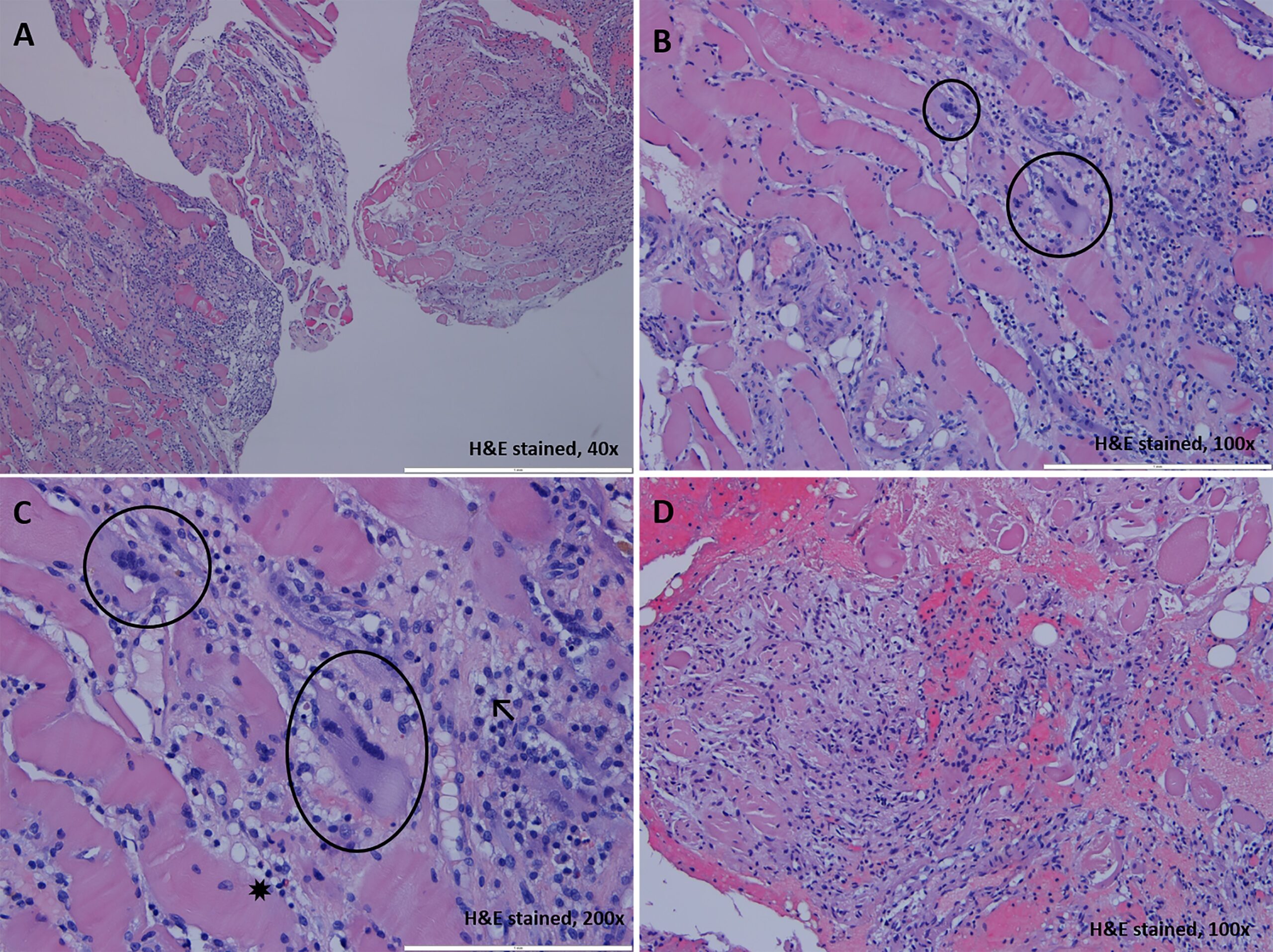
 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5An 81-year-old Portuguese woman, independently mobile, with antecedents of restrictive pulmonary disease and multinodular goiter, presented to the emergency department with lumbar and left hip pain and an inability to walk or bear weight after a low-energy fall. On examination, paravertebral lumbar discomfort and left groin pain with decreased passive and active ranges of motion were noted. A hip radiograph (Fig. 1) was made, revealing an acute left-sided femoral neck fracture. Also, a lumbar radiograph (Fig. 2) was made, revealing chronic osteoporotic vertebral fractures. These fractures were assessed by computed tomographic (CT) scan to determine displacement and comminution (Fig. 3). Incidentally, hundreds of oblong calcific specks were detected in a “rice-grain calcification” appearance (Figs. 1, 2, and 3).
The patient was evaluated by an infectious disease consultant. A laboratory testing was requested, including white blood cell count, liver function, and inflammatory markers. The results did not suggest active infection; there was only a mild elevation of C-reactive protein, compatible with the post-traumatic period.
In spite of the calcifications, there was no contraindication for osteosynthesis or arthroplasty, so the patient underwent a total hip arthroplasty with cemented components (Fig. 4). A sample of muscle was obtained for histological analysis (Fig. 5) and showed fragments of skeletal muscle and adipose tissue with a mononucleated inflammatory infiltrate and multinucleated giant cells, as well as muscle cells with reactive features, suggestive of a chronic inflammatory muscular disease.
With the intramuscular “rice-grain” calcifications, the patient was diagnosed with intramuscular cysticercosis. The patient confirmed eating undercooked pork meat but reported no history of myalgia, soft-tissue nodules, neurological symptoms, or eye symptoms. Medical records from a private neurologist revealed a previous diagnosis of asymptomatic neurocysticercosis. No family history of muscular cysticercosis was found.
More than 1 year after the surgical procedure, the patient presented with good postoperative evolution, without pain, instability, or signs of infection.
Proceed to Discussion >>Reference: Relvas-Silva M, Pereira JS, Lopes J, Martins D, Leite MJ, Sousa AN. Muscular cysticercosis: an incidental finding in the developed world. JBJS Case Connect. 2021 Jun 10;11(2).e20.00707.
Intramuscular cysticercosis is rare and generally not fatal. Symptoms are variable, ranging from being asymptomatic to having painful and tender swellings. Fever is usually absent. There are 3 types of clinical manifestations according to the triggered immune response: (1) the myalgic type; (2) the mass-like, pseudotumor, abscess-like type; and (3) the uncommon pseudohypertrophic type. Because most muscular cysticercosis is associated with central nervous system disease and brain and eye infections cause the most morbidity, their involvement must be ruled out.
Because of nonspecific clinical presentation, the diagnosis can be difficult and delayed. Frequently, radiographs may raise suspicion of this diagnosis. The imaging findings depend on the cysticerci stage: in the active phase, cysticerci are rarely encountered in radiographs. In contrast, quiescent calcified cysts may be detected incidentally as millet seed-shaped elliptical calcifications with a characteristic starry-sky appearance (either on radiograph or CT scan). Although ultrasound is useful to identify the scolex (the head or anterior end of an adult tapeworm), magnetic resonance imaging (MRI) is the gold-standard technique for the diagnosis and evaluation of the disease stage. In most cases, currently available noninvasive imaging methods have obviated the need of definitive histologic validation.
No specific treatment is required, unless there are painful lesions. In this case, treatment may include surgical excision or anthelminthic medications (if a surgical procedure is unfeasible by the site or number of lesions). However, early appropriate diagnosis, by pattern recognition, is key to an adequate referral and treatment, optimizing health-care services and not jeopardizing the patient’s care.
This case is unique because it reports an incidental and uncommon finding in the developed world, namely a final stage of intramuscular cysticercosis. This form of disease is infrequent and has been rarely reported. Moreover, to the best of our knowledge, this is one of the first reports of hip arthroplasty in a patient with a history of parasitic infection (without the need for directed pathogen treatment).
Reference: Relvas-Silva M, Pereira JS, Lopes J, Martins D, Leite MJ, Sousa AN. Muscular cysticercosis: an incidental finding in the developed world. JBJS Case Connect. 2021 Jun 10;11(2).e20.00707.
What is the diagnosis?
Angiomatosis
Dermatomyositis
Intramuscular cysticercosis
Schistosomiasis
Calcium pyrophosphate deposition disease