A Fifty-six-Year-Old Woman with Worsening Knee Pain
October 7, 2015
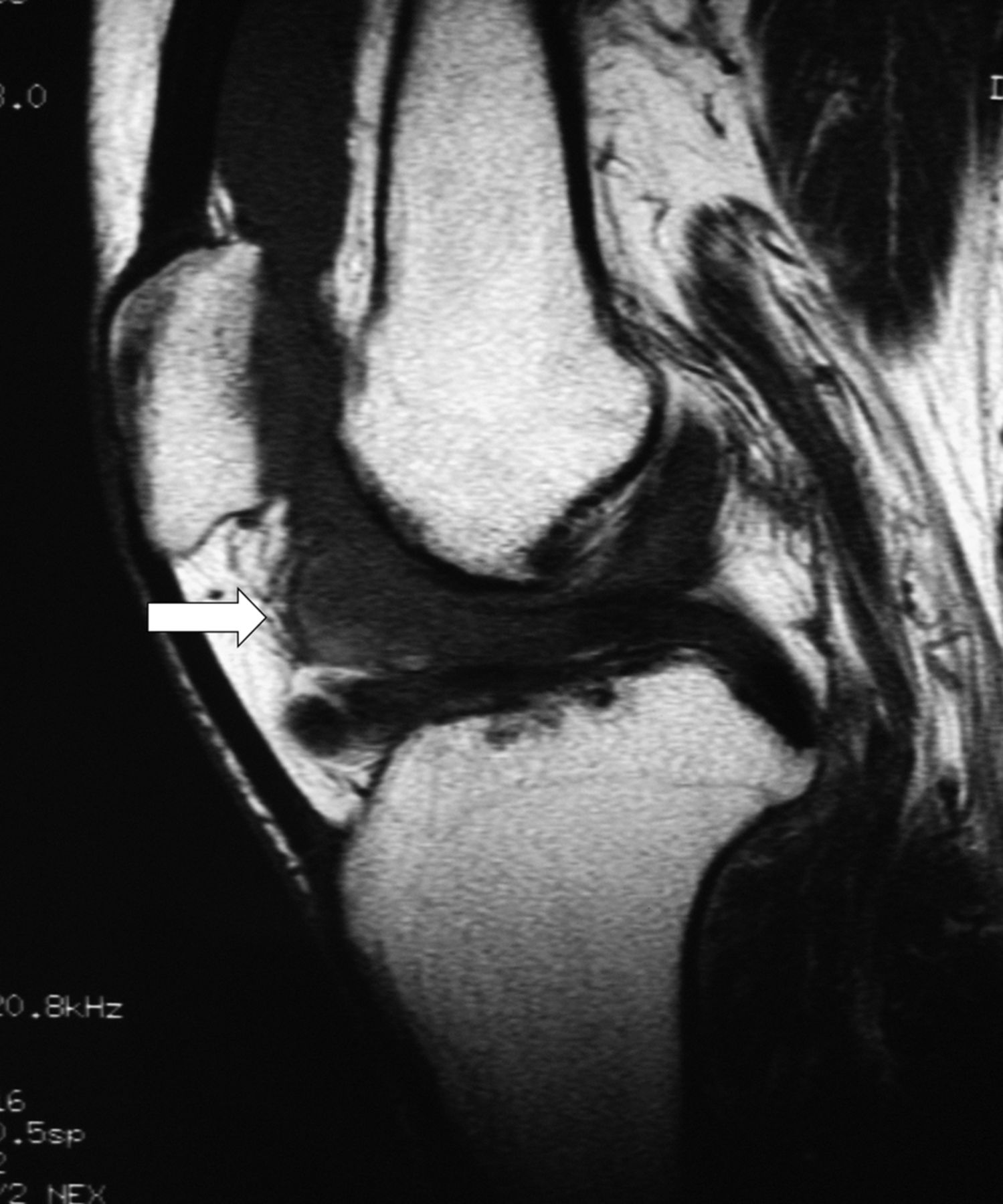
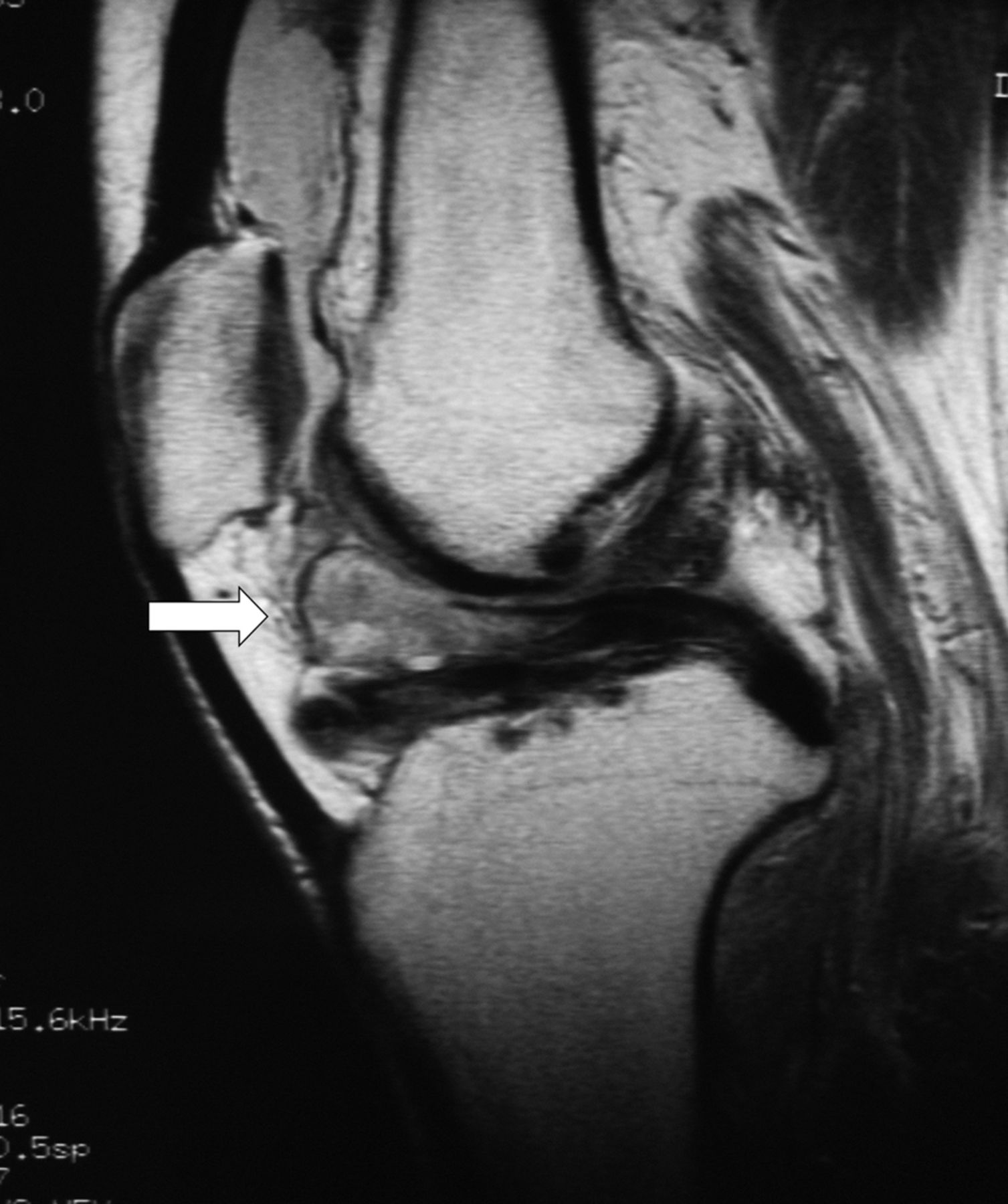
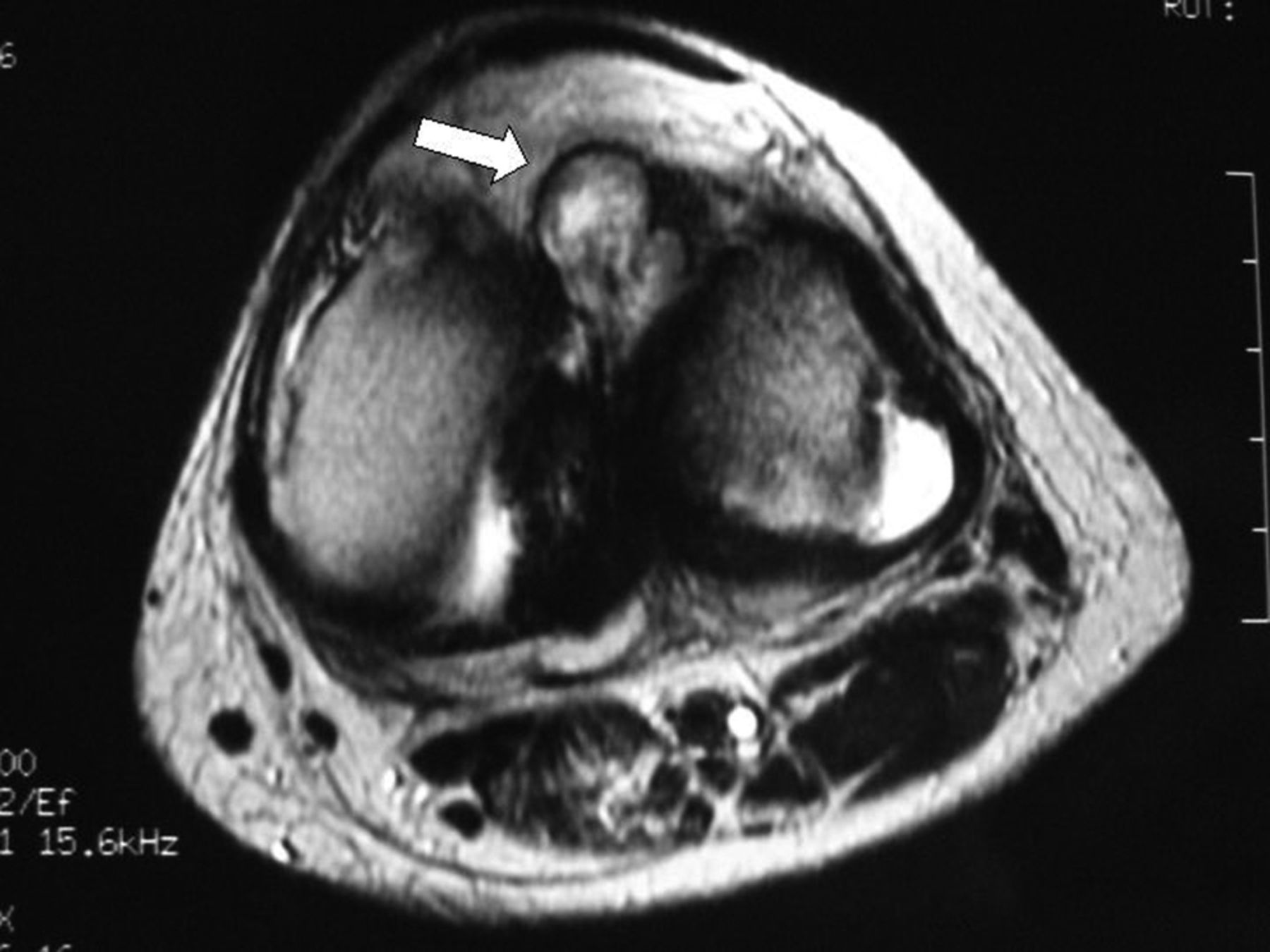
 Fig. 1-A
Fig. 1-A Fig. 1-B
Fig. 1-B Fig. 1-C
Fig. 1-C Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4-A
Fig. 4-A Fig. 4-B
Fig. 4-BA fifty-six-year-old woman was referred to our department because of recurrent hemarthrosis of the knee and exacerbation of knee pain. The patient had experienced a catching sensation in the left knee joint since the age of approximately thirty years, but she did not seek medical advice because she had no pain. Approximately one month before presenting to our department, she visited a physician because of swelling and pain in the left knee without apparent cause, which led to difficulty in walking. Bloody joint fluid was aspirated, but subsequently the hemarthrosis and knee pain recurred. The patient had a history of cervical spinal cord injury due to a traffic accident when she was thirty-nine years old, which had resulted in quadriparesis. She used a T-shaped stick while walking. At presentation, in addition to difficulty with walking, she had marked swelling and pain in the left knee. Instability of the knee was not demonstrated, but a large effusion was present. Left knee motion was −20° of extension and 60° of flexion (unaffected knee: −5° of extension and 125° of flexion). She had tenderness along the lateral joint line. Evaluation of the meniscus with the McMurray test and Apley test was difficult because of pain and a limited range of motion. Hip and ankle motion was normal, and no disturbance in sensation to painful stimuli was detected in the lower extremity. A radiograph demonstrated osteoarthritic changes of the lateral compartment in both knees. Magnetic resonance imaging (MRI) revealed a 2-cm-long mass lesion anterior to the intercondylar notch in the left knee, showing low signal intensity on the T1-weighted image and a mixture of low and high signal intensity on the T2-weighted image (Figs. 1-A and 1-B). A degenerative tear of the lateral meniscus was observed in both knees (Fig. 1-C). Serum tests showed mild anemia and an increased erythrocyte sedimentation rate. Biochemical and coagulation test results were normal. There was no history of a bleeding disorder or anticoagulant treatment.
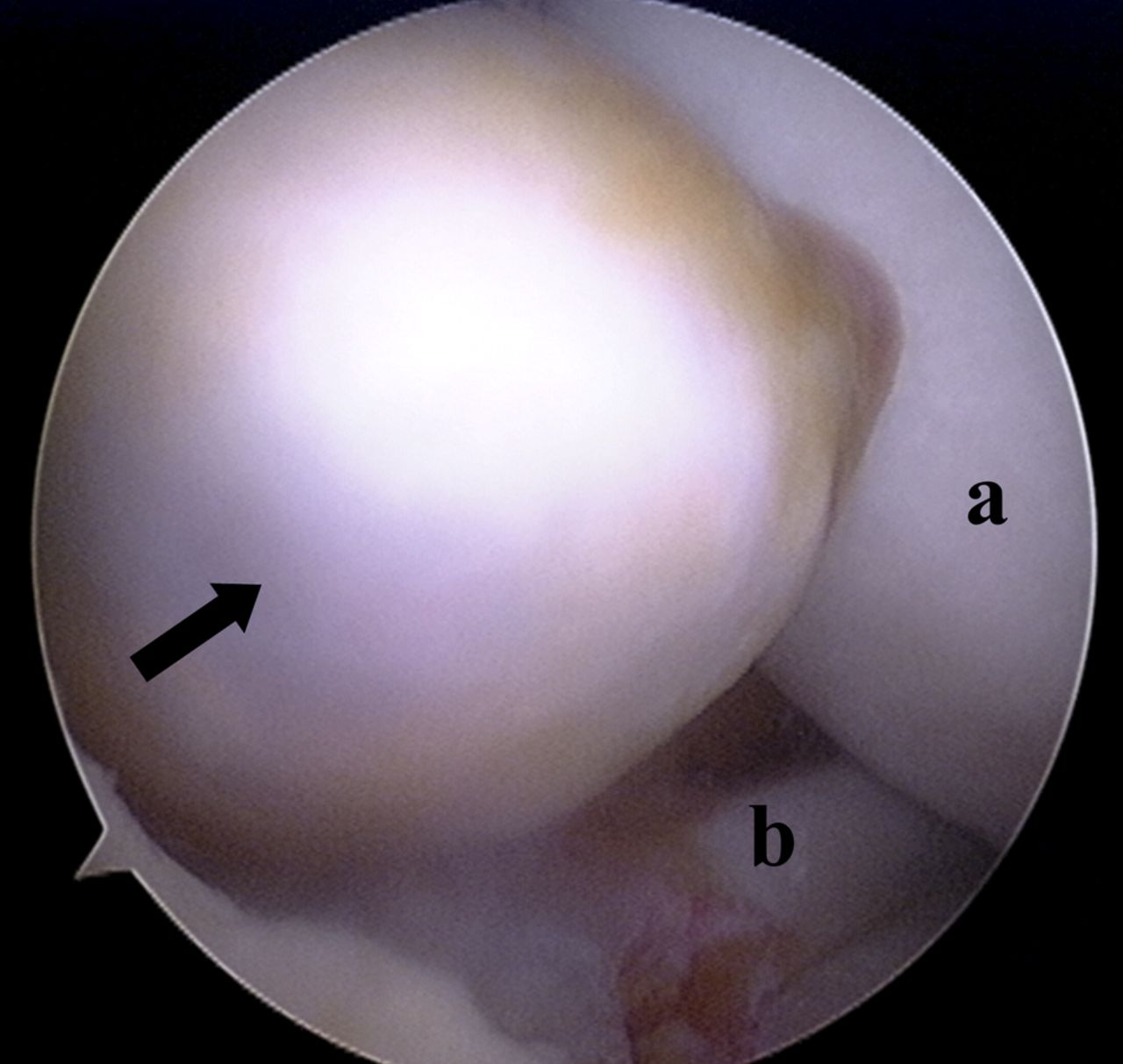
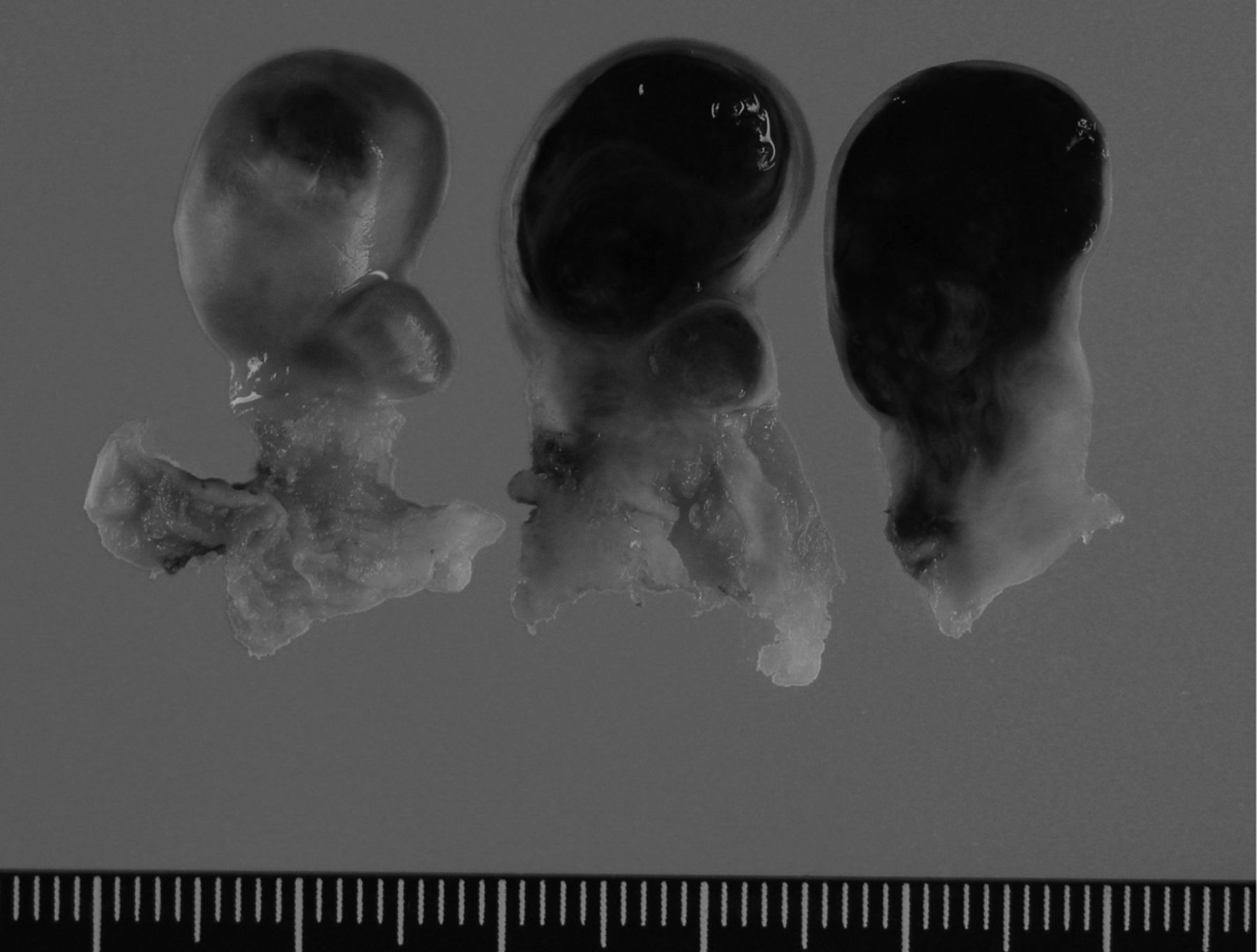
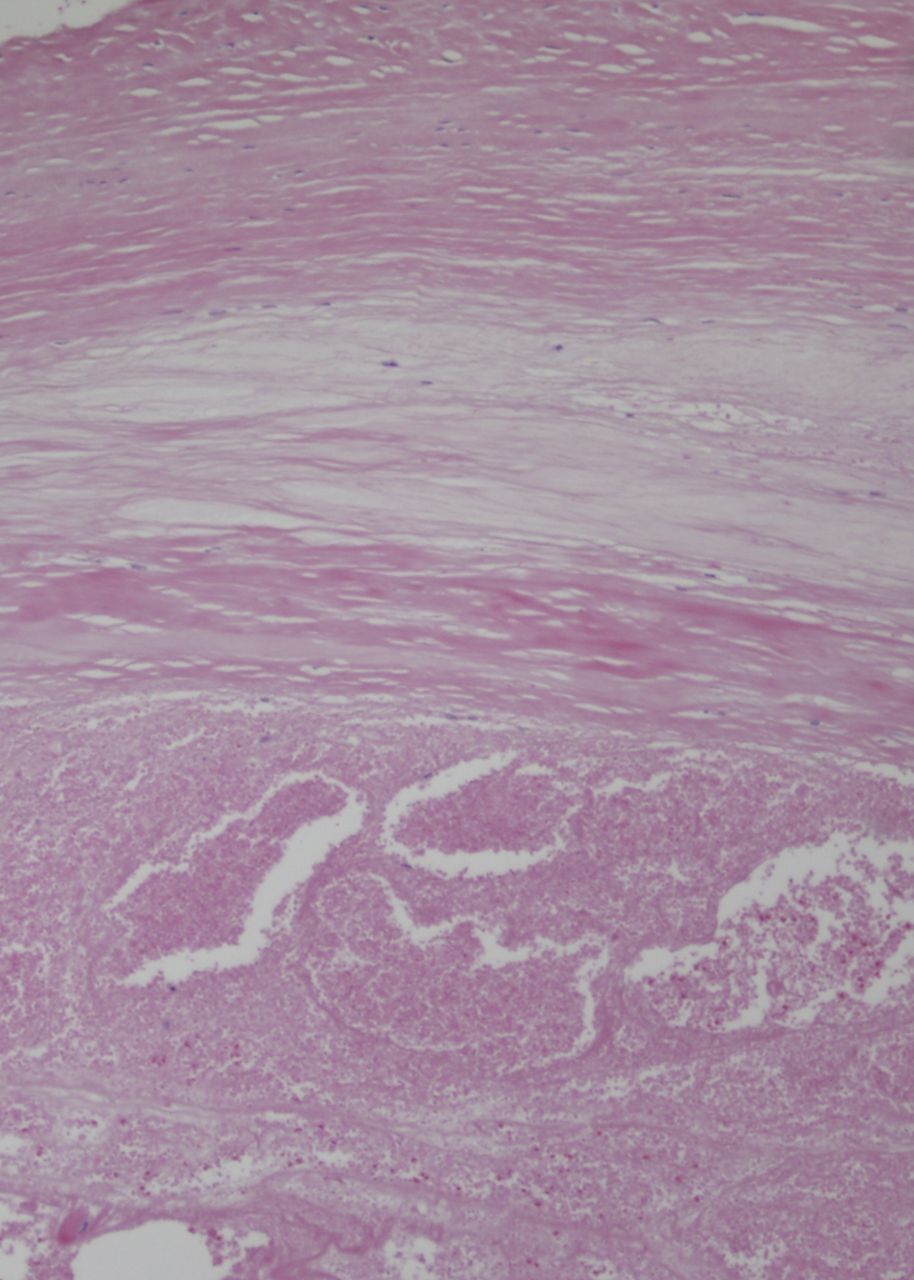
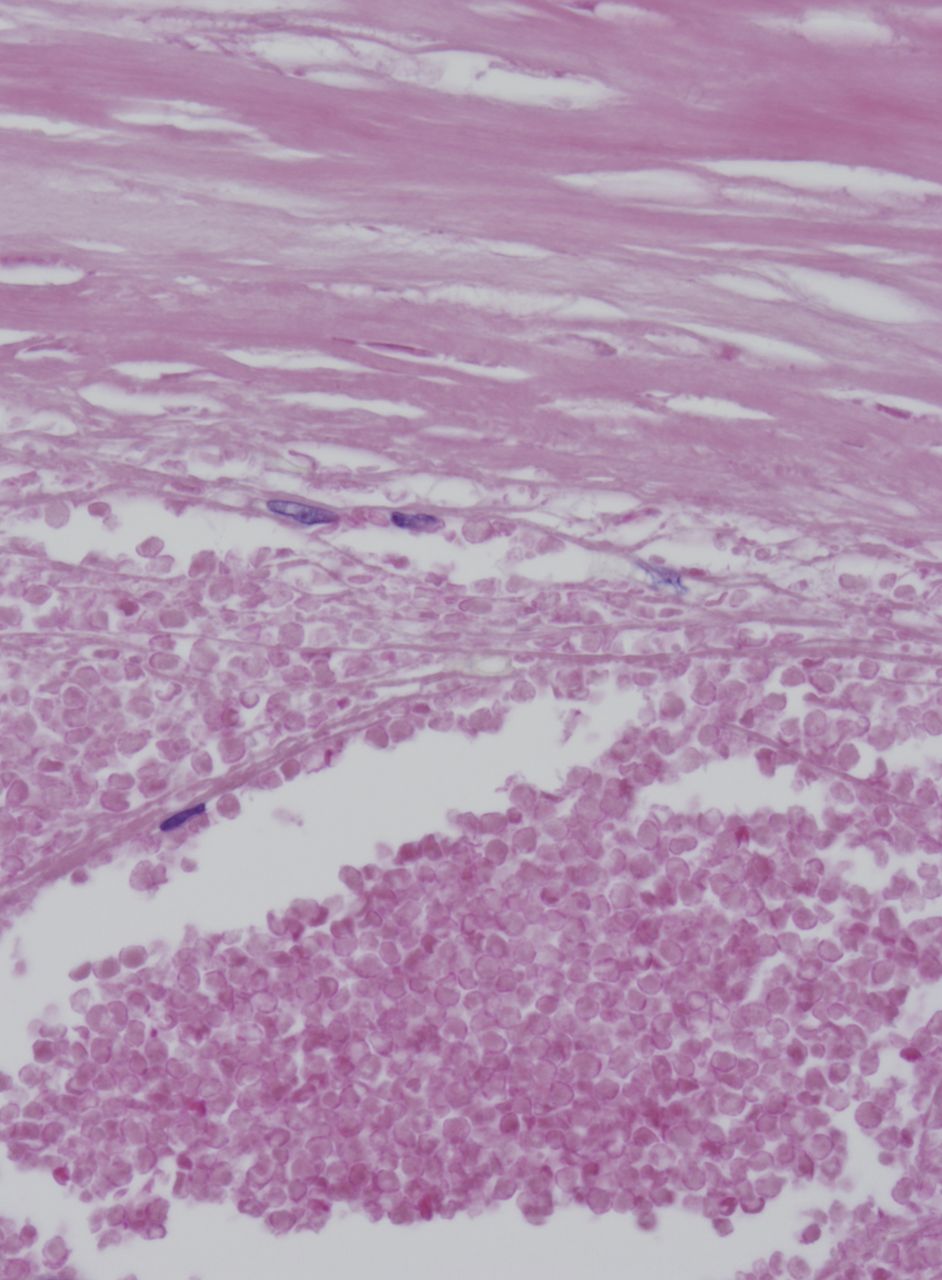
Because of the findings of an intra-articular mass and recurrent hemarthrosis, pigmented villonodular synovitis was suspected and arthroscopic surgery was conducted. Arthroscopic examination showed a bucket-handle tear adjacent to the lateral meniscus insertion site extending from the middle segment to the posterior horn, as well as a mass in the midportion of the bucket handle. The mass had a smooth surface and a membrane of elasticity like rubber. It appeared as a polyp-like elevation from the region of the bucket-handle tear and showed no continuity with other intra-articular structures (Fig. 2). The meniscal bucket-handle portion together with the mass was resected arthroscopically. Under arthroscopic viewing, although active bleeding was not observed, a blood clot was found around the tear of the lateral meniscus. The ruptured site of the lateral meniscus was suspected to be the source of bleeding, and hemostasis was achieved with electrocoagulation. Gross examination of the resected mass lesion showed a pedicled tumor with a smooth surface measuring 15 × 12 mm in diameter. The surface was covered with fibrous tissue, and the interior contained a black substance resembling a hematoma (Fig. 3). Histopathologically, the surface layer of the mass was fibrous connective tissue and the interior content was a blood clot composed of red blood cells and fibrin (Figs. 4-A and 4-B). No vascular structure was observed in the resected specimen. On the basis of the above findings, the diagnosis was meniscal hematoma associated with a lateral meniscal tear. As a preventive measure against rebleeding after surgery, the knee was immobilized in a plaster splint and weight-bearing was restricted. Knee motion exercises were started two weeks later. Full weight-bearing was permitted at four weeks after surgery. There was a transient recurrence of the hemarthrosis two months after surgery. Swelling of the knee was observed, and 7 mL of bloody joint fluid was aspirated. Thereafter, there was no recurrence of the hemarthrosis, and the subsequent course was uneventful through fourteen months of further follow-up. Motion of the affected knee improved to 5° of extension and 125° of flexion. The patient walked with a T-shaped cane.
Proceed to Discussion >>Reference: Ochiai S, Hagino T, Watanabe Y, Senga S, Haro H. A rare case of meniscal hematoma with hemarthrosis of the knee: a case report. J Bone Joint Surg Am. 2011 Sep 21;93(18):e104.
In both of the cases of meniscal hematoma that we identified in the literature, the hematoma developed in the medial meniscus, suggesting that the hematoma might have been caused by bruising or ligament rupture and that the etiology could have been a rupture of the vascular network at the meniscal margin due to mechanical stress. In our case, however, the meniscal hematoma arose without any apparent cause and involved the lateral meniscus. Furthermore, spontaneous knee hemarthrosis occurred concurrently, which differs from the two previously reported cases. We believe that spontaneous hemarthrosis was first reported in 1959 by Wilson, as a recurrent knee hemarthrosis of unknown cause associated with degenerative osteoarthritis in middle-aged persons. Thereafter, a relationship between spontaneous hemarthrosis and a degenerative tear of the lateral meniscus as well as lateral compartment osteoarthritis of the knee was proposed. Sasho et al. reported that 89.5% of patients with spontaneous hemarthrosis had a degenerative tear of the lateral meniscus and 57.9% had osteoarthritis primarily in the lateral compartment. The main cause of recurrent hemarthrosis has been assumed to be bleeding from the peripheral arteries of the lateral meniscus due to traction caused by the torn meniscus. Other factors include anatomical characteristics—i.e., the fact that peripheral arteries distributed in the lateral meniscus have greater calibers and are closer to the meniscal margin compared with those in the medial meniscus—and the vascular fragility associated with severely osteoarthritic knees and aging. In the present case, degenerative and bucket-handle tears of the lateral meniscus were accompanied by extensive osteoarthritic changes of the lateral joint surfaces. We speculate that gap or cyst formation inside the meniscus due to degeneration, or breakage of fragile vessels inside or close to the meniscus, could have been involved in the formation of the meniscal hematoma. Furthermore, the swollen meniscus torn in a bucket-handle shape, together with the ruptured vessel branches, could have led to spontaneous hemarthrosis. The two previously reported cases of meniscal hematoma in the literature were treated with arthroscopic decompression. In our case, we performed endoscopic partial resection of the meniscus, including the hematoma, and hemostasis with electrocoagulation. Resection of the lateral meniscus has been recommended as a treatment for spontaneous hemarthrosis. The postoperative course of our case was uneventful. Meniscal hematoma should be considered as one of the differential diagnoses for an intra-articular mass with recurrent hemarthrosis of the knee.
Reference: Ochiai S, Hagino T, Watanabe Y, Senga S, Haro H. A rare case of meniscal hematoma with hemarthrosis of the knee: a case report. J Bone Joint Surg Am. 2011 Sep 21;93(18):e104.
Meniscal cyst
Meniscal hematoma
Pigmented villonodular synovitis
Degenerative meniscal tear
Synovial cell sarcoma